Marine power loss/Loss of control
Arctic Wings and Rotors
Pilatus Britten-Norman BN2A-20 Islander
C-GMOP
Tuktoyaktuk, Northwest Territories 7.7 mi SE
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The pilot and passengers on board the Britten-Norman Islander were on a scheduled night visual flight rules flight from Tuktoyaktuk to Inuvik, Northwest Territories. Approximately four minutes after take-off, the pilot reported to the Tuktoyaktuk Flight Service Station that he had an engine problem and was returning to the airport. When the aircraft did not arrive, an air and ground search was initiated. The wreckage was located three hours later, on an ice-covered lake approximately eight miles southeast of the airport. There were no survivors.
The Board determined that a magneto impulse coupling, worn beyond the prescribed limits, resulted in the failure of the right engine. Following the engine failure, the pilot mistrimmed the rudder and was unable to maintain control of the aircraft.
1.0 Factual Information
1.1 History of the Flight
On 03 December 1993, a Britten-Norman BN2A-20 Islander, registration C-GMOP, owned and operated by Arctic Wings and Rotors, departed Tuktoyaktuk, Northwest Territories, on a night visual flight rules (VFR)Footnote 1 flight to the Inuvik townsite airstrip. On board were the pilot and six passengers. The pilot took off from runway 09 at 1706:34 mountain standard time (MST)Footnote 2, and had turned the aircraft to a southerly direction when the right engine (Textron Lycoming IO- 540-K1B5) lost all power (see Appendix A).
At 1710:40, the pilot reported to Tuktoyaktuk Flight Service Station (FSS) that he had an engine problem and was trying to get back to the airport. At 1711:44, he reported that he was "presently heading back to the airport at this time." At 1711:58, he reported "showing six miles back from the airport at this time." The FSS specialist asked if he was declaring an emergency, and the pilot's response was indecisive. During the last radio transmission, there were indications of stress in the pilot's voice; however, there was no further mention of the specific nature of the problem. The pilot did not report his altitude during the conversations with the FSS. The transmission lasted approximately 15 seconds and ended at 1713:03.
When the aircraft did not return to the airport, an air and ground search was initiated. The aircraft was located on an ice-covered lake approximately eight miles southeast of the airport. The aircraft struck the ice in a steep nose-down attitude. The engines and front of the aircraft penetrated the approximately two-foot-thick layer of ice. The remainder of the fuselage, wings, and empennage remained on the ice surface. The seven occupants were fatally injured.
The accident occurred during the hours of darkness at approximately 1713 MST, at latitude 6920′N, longitude 13256′W, at an elevation of approximately 50 feet above sea level (asl)Footnote 3.
1.2 Injuries to Persons
| Crew | Passengers | Others | Total | |
| Fatal | 1 | 6 | - | 7 |
|---|---|---|---|---|
| Serious | - | - | - | - |
| Minor/None | - | - | - | - |
| Total | 1 | 6 | - | 7 |
1.3 Damage to Aircraft
The aircraft was destroyed.
1.4 Other Damage
None.
1.5 Personnel Information
| Pilot-in-command | |
|---|---|
| Age | 27 |
| Pilot Licence | ATPL |
| Medical Expiry Date | 01 May 94 |
| Total Flying Hours | 3,224 |
| Hours on Type | 848 |
| Hours Last 90 Days | 298 |
| Hours on Type Last 90 Days | 208 |
| Hours on Duty Prior to Occurrence | 8 |
| Hours Off Duty Prior to Work Period | 12 |
The pilot held a valid licence with a Class I instrument rating. He occupied the left front seat, and was at the controls at the time of the accident. The right front seat was unoccupied.
The pilot received his private pilot licence in 1986, his commercial licence in March 1987, a seaplane rating in May 1987, and multi-engine and instrument rating in April 1988. His recent flying, during training on the PA-31 Navajo with the chief pilot, was described as "very professional", and it was noted that he "seemed to have all the procedures down pat."
The pilot's last pilot proficiency check (PPC) on the Islander was on 30 April 1993. His most recent Transport Canada (TC) PPC and instrument renewal ride was on a Piper PA-31 Navajo, on 25 November 1993.
The pilot had previously flown Islander aircraft for a former employer in northern British Columbia. He commenced employment with Arctic Wings and Rotors in April 1993. According to the aircraft journey log-books, he flew approximately 406 hours during the previous four months on the Cessna 185, Cessna 207, Piper PA-32 Cherokee Six, Piper PA-31 Navajo, and the two Britten-Norman BN2A-20 Islanders.
The pilot had not received any on-type night training on the BN2A aircraft. Air Navigation Order (ANO) VII, No. 3, Para 46. (1) (b) (iii) states that the flight training provided by an air carrier for a pilot before he serves as a pilot flight-crew member in a multi-engine aircraft shall include, in each type of aeroplane he is to fly, flight instruction and practice in take-offs and landings by night if he is to fly at night. The pilot's last night flying training was on 20 November 1993 on the PA-31. The pilot had limited IFR experience, and did not receive any IFR training on the BN2A aircraft. No other aspects of night flying, such as the handling of emergencies at night, are singled out for mandatory training by this ANO.
The pilot reportedly had good sleep habits and adequate rest the previous night. He had a bronchial asthmatic condition that was treated with prescription medication and inhalers as required. The pilot was respected by his peers and described as a dedicated, well organized, conscientious individual who loved flying, and was proficient on the aircraft he flew.
1.5.1 Pilot's Work Schedule
On the day of the accident, the pilot's first flight was from Inuvik to Tuktoyaktuk and return. The departure from Inuvik was at 1245; the return flight landed in Inuvik at 1405. The second flight (the accident flight) was also an Inuvik/Tuktoyaktuk/Inuvik flight with a scheduled departure from Inuvik at 1600. His flight time for the day was 2.2 hours, and his duty time was approximately eight hours (duty time is estimated to be one hour before departure and one-half hour after return to base). The previous evening he reportedly went to bed at 2230; he arose at 0720 and had breakfast.
The previous day, 02 December, he had a flight time of 3.1 hours and duty time of approximately 12.5 hours. On 01 December, he had a flight time of 2.9 hours and a duty time of approximately 11 hours. On 30 November, he had a flight time of 9.7 hours and duty time of 15 hours.
The pilot had a flight time of 93 hours during the last 30 days, and 298 hours the last 90 days. According to the aircraft journey log-books, there was a total of 13 days since 01 August when the pilot did not fly. His most recent non-flying day was 11 November.
Days off were on an irregular, unscheduled basis and generally subject to the seasonal workload. Days on which a pilot was not scheduled to fly were considered as days off. The residence for most of the company pilots was located adjacent to the base of operations, and pilots were normally available to take a flight on very short notice. Occasionally, a pilot would return to duty and complete a flight on a day he was not scheduled to fly. Generally, this was a mutually satisfactory arrangement between the pilots and the company.
1.6 Aircraft Information
| Manufacturer | Pilatus Britten-Norman Limited |
| Type | BN2A-20 Islander |
| Year of Manufacture | 1974 |
| Serial Number | 398 |
| Certificate of Airworthiness (Flight Permit) | Issued |
| Total Airframe Time | 9,391 hr |
| Engine Type (number of) | Lycoming IO-540-K1B5 (2) |
| Propeller/Rotor Type (number of) | Hartzell HC-C2YK-2CUF (2) |
| Maximum Allowable Take-off Weight | 6,600 lb |
| Recommended Fuel Type(s) | 100/130 |
| Fuel Type Used | 100 LL |
1.6.1 Aircraft Records
The company had operated the aircraft since February 1993. Prior to that, the aircraft had been leased to another operator in Inuvik. Examination of the aircraft maintenance records and log- books, to the extent possible, revealed no outstanding aircraft defects. The aircraft journey log- book was retrieved from the water during the on-site investigation and dried out. Some entries had been made in water-soluble ink, and the entries were illegible. The last entry in the aircraft technical log-book was on 13 October 1994, 116 hours prior to the accident.
The aircraft and maintenance records were incomplete, and it was not possible to determine if an unserviceability had been reported, rectified, or deferred, or to determine who had performed the work and what parts may have been repaired or changed. No documentation or worksheets were found for work completed or components changed between inspections.
According to the aircraft journey log-book, a 100-hour inspection was completed on C-GMOP on 07 November 1993 at 9,313.0 aircraft hours, and a 50-hour inspection was completed on 02 December 1993 at 9,385.1 hours.
1.6.2 Weight and Balance Calculations
The aircraft weight at the time of the accident was calculated to be approximately 6,200 pounds, and the centre of gravity (C of G) was within the prescribed limits at 23.9 inches aft of datum. The C of G limits are 20.9 to 25.6 inches aft of datum.
1.6.3 Aircraft Performance
Pilatus Britten-Norman provided performance data based on a test flight and calculations for a temperature of minus 19 degrees Celsius.
At a gross weight of 6,200 pounds, the expected stall speed and the minimum single-engine control speed (VMCA) with the flaps in the take-off position would be approximately the same. With the engines at idle rpm (no data available for stall speeds with the engine operating at high power settings), the stall speed would be 48 knots with the wings level, 50 knots in a 20-degree bank, and 57 knots in a 40-degree bank at a constant altitude.
At low gross weights, the aircraft will reach VMCA before the stall, and at high aircraft weights, the stall will occur before reaching VMCA. The manufacturer's report indicates that if the airspeed decays below the VMCA and the aircraft has not stalled, the result will be the start of a slow turn; there will be no sudden catastrophic event.
At 6,200 pounds, the estimated single-engine rate of climb would be approximately 315 feet per minute (fpm) at 60 knots, and 360 fpm at 70 knots. Information provided by the manufacturer indicates that an ice buildup of 1/16 to 1/8 inch would not adversely affect the flight characteristics of the aircraft under normal flying operations.
1.6.4 Single Engine Procedures
The Britten-Norman Owner's Handbook, Section 4, Emergency Operating Procedures, states that, in the event of an engine failure after take-off, the recommended procedure is as follows:
Apply take-off power to both engines, mixture full rich on both engines, identify the inoperative engine, select the mixture control lever to IDLE CUT-OFF, feather the inoperative engine, ensure that the generator on the operating engine is ON, allow the airspeed to build up to 65 knots IAS (best single-engine rate of climb), select the flaps UP, and ADJUST the rudder trim as necessary for the climb.
1.7 Meteorological Information
1.7.1 Weather Synopsis
A weather analysis for the period covering the occurrence was provided by the Atmospheric Environment Service, Arctic Weather Centre for the Inuvik and Tuktoyaktuk regions. A weak surface trough of low pressure extended from north of Barter Island, Alaska, southeast through Tuktoyaktuk to eastern Great Slave Lake. The trough was moving northeast at about five knots and remained weak. During the morning and early afternoon, scattered cloud was observed at Tuktoyaktuk. At 1300 the cloud base was 700 feet, and at 1500 the base had risen to 1,100 feet with tops at 1,800 feet. At the time of the crash, the conditions remained the same, with light southwesterly surface winds.
1.7.2 Hourly Observations
The 1700 weather observation for Tuktoyaktuk was aircraft ceiling 1,100 feet overcast, 15 miles visibility and light snow. The wind was from 200 degrees true at eight knots. The temperature and dew point were minus 19 degrees and minus 21 degrees Celsius, respectively. The altimeter setting was 29.65 inches of mercury.
The 1700 weather observation for the Inuvik Airport (six miles southeast of the townsite, at an elevation 210 feet higher) was balloon ceiling 500 feet overcast, visibility six miles in ice fog; temperature and dew point, minus 23 degrees and minus 27 degrees Celsius, respectively. The wind was calm. The pilot was provided the Inuvik weather by the FSS specialist while taxiing for take-off.
Civil twilight (darkness) on 03 December 1993 occurred at 1623.
1.7.3 Pilot Reports
On landing at the Tuktoyaktuk Airport, the Islander pilot reported to the FSS that the cloud base was about 1,100 feet above ground level (agl). Another pilot, approximately one hour earlier, had reported the cloud base at 1,100 feet and the tops of the cloud layer at 1,800 feet.
1.7.4 VFR Flight at Night
An overcast night without a visible horizon provides few, if any, visual cues to the pilot, and is similar to instrument meteorological conditions (IMC), in that the conditions require the pilot to make careful reference to the aircraft flight instruments.
A 1990 TSB report, VFR Flight into Adverse Weather, Section 2.1, VFR Weather Minima, states that:
Canadian regulations are, in many ways, more stringent for commercial operations than for private operations. However, the criteria for weather minima during day VFR operations for commercially-operated aircraft are the same as those governing VFR flight, placing a large number of fare-paying passengers at risk.
This comment applies to an even greater extent to night flight under VFR.
1.7.5 Night VFR in Commercial Operations
Pilots fly aircraft either by VFR or by instrument flight rules (IFR). Flight operations in accordance with VFR at night are safe provided that visual reference and flight visibility are adequate to manoeuvre the aircraft with reference to the horizon and ground features. Sometimes cues necessary to fly an aircraft at night by outside references are not available. Even in conditions of good night visibility, it can be difficult to fly by visual reference over dark or sparsely lit terrain.
When pilots flying at night encounter conditions of poor visual cues, they must possess the skill to fly by instruments, and must be adequately trained for instrument flight. Transport Canada's Flight Training Manual.(FTM), page 178, indicates that flying by reference to the ground or water can be difficult at night:
Night flying does require that you readjust to a relatively different environment, especially outside the cockpit. Reference points such as the horizon, topographical features, and even the ground itself, all so vital in establishing aircraft attitude by day, are indistinct, obscure, and sometimes invisible.
Commercial flights for aircraft of 12,500 pounds or less conducted under IFR are required to meet the standards outlined in ANO VII, No. 3 ( Standards and Procedures for Air Carriers Using Small Aeroplanes in Air Transport Operations ., Part IV, 39. (3), which requires two pilots, or, under Schedule C, 1(b)Footnote 4 application, one pilot and a two-axis autopilot. For a night VFR flight, commercial operators are not required to meet these standards; however, the pilot must have an instrument rating, and the air carrier must fly along airways, air routes, or company routes.
1.7.6 Training Environment vs. Operational Environment
Training for a pilot up to the level of small air carrier operations consists of practice and simulating emergency procedures. During dual instruction or on a flight with a training pilot, the pilot is generally prepared for abnormalities, and expects to have to demonstrate his ability to deal with emergency exercises.
In contrast, emergency and abnormal situations in an operational environment are authentic and usually unexpected by the pilot. The Islander emergency occurred at night in marginal visual meteorological conditions (VMC), with few, if any, visual references, likely with no horizon visible.
1.7.7 Training Requirements: ANO VII No. 3 vs. ANO VII No. 2
Training requirements for air carriers operating under ANO VII, No. 3, differ from the more comprehensive requirements for air carriers operating under ANO VII, No. 2 ( Standards and Procedures for Air Carriers Using Large Aeroplanes.. Some of the specific elements that are required under ANO VII No. 2 but not required under ANO VII No. 3 are as follows: flight training on rejected landings from 50 feet with simulated IFR conditions from 100 feet; demonstrated knowledge of the route being flown plus route checks and route currency; PPCs every six months including certain assessments under IFR or simulated IFR conditions; demonstrated pilot ability to fly circling approaches; demonstrated pilot ability to fly missed approaches including a failure of a critical engine under simulated IFR or in a simulator.
Pilots flying a twin-engine aircraft such as the BN2A, to which the requirements of ANO VII No. 3 apply, are required to have 1.5 hours air time of flight training per year on-type. Pilots who are not trained under the more comprehensive requirements of ANO VII No. 2 are more likely to encounter circumstances on operational flights that they have been unable to practice for in a realistic way.
Normally, a commercial pilot of small, multi-engined aircraft must demonstrate competency on each aircraft type during an annual Transport Canada pilot proficiency check (PPC); however, Transport Canada may grant a carrier an aircraft PPC "grouping." Under the grouping system, a pilot who successfully completes a PPC on one aircraft is endorsed on up to two other multi- engine aircraft types. A different type of aeroplane flown by the pilot should be used each successive year for the conduct of the PPC. A PPC grouping does not exempt the operator from conducting ground and flight training on each type of aircraft.
Transport Canada policy letter no. 9 outlines the policy for the grouping of aircraft: "... The grouping of aeroplane types and models (for PPC purposes) is based upon those having sufficiently similar handling characteristics and performance." Transport Canada's grouping policy does not require that factors such as aircraft systems, limitations, cockpit layout, or control configuration be considered prior to grouping.
There is an approved grouping list for aircraft having a Maximum Certified Take-Off Weight (MCTOW) of over 7,000 pounds; however, there is no similar grouping list for aircraft below MCTOW 7,000 pounds, and only general guidance is provided for the grouping of aircraft. Each regional director of Transport Canada Air Carriers branch may determine aircraft groupings below 7,000 pounds MCTOW.
In this accident, the operator had been granted a grouping for the BN-2 Islander and the Navajo PA-31; therefore, the PPC flown by the pilot on the PA-31 the week prior to the accident fulfilled his proficiency requirement for the Islander. The BN-2 Islander and the Navajo PA-31 flying characteristics are quite different. The PA-31 Navajo has low wings, retractable landing gear and has much higher climb and cruise performance, and can be controlled down to 78 knots with one engine operating (VMCA). In contrast, the Islander has high wings, fixed landing gear, and the cruise speed and VMCA are about 30 knots slower than the Navajo's.
1.8 Aids to Navigation
A non-directional radio beacon (NDB) is located on the Tuktoyaktuk Airport, and serves as an approach aid for runway 09, as published in the Canada Air Pilot. The aircraft was equipped with a Trimble Global Navigation System (GPS). The aircraft was not equipped with an autopilot.
1.9 Communications
Communications between the pilot and the Tuktoyaktuk FSS were established and satisfactory.
1.10 Aerodrome Information
The Tuktoyaktuk Airport is situated adjacent to the hamlet of Tuktoyaktuk. The airport reference point elevation is 15 feet asl. The runway is oriented 088 degrees (09) and 268 degrees (27) magnetic, and is 5,000 feet long by 150 feet wide, with a gravel surface. It is equipped with runway end identification lights (AS) and medium intensity (ME) runway edge/end and threshold (TE) lights. A two-bar visual approach slope indicator system (VASIS) is installed at both ends of the runway. The lighting equipment was reported to be operating normally.
1.11 Flight Recorders
The aircraft was not equipped with a flight data recorder (FDR) or a cockpit voice recorder (CVR), nor was either required under existing regulations.
1.12 Wreckage and Impact Information
1.12.1 Aircraft Wreckage
The aircraft struck the ice at an impact angle of approximately 65 degrees nose down while rotating in a clockwise direction. The forward section of the aircraft, both engines, and the propellers broke through the ice and were submerged in water. Both engines were torn from the mounts, and remained attached to the wing by wires and engine control cables. The propellers remained attached to the engines. The right propeller was found in the feathered position with slight damage to the blades. The right throttle was at the idle position, and the right propeller control lever was in the feathered position. The left propeller blade damage and twist were consistent with considerable power being produced at impact. The left throttle and propeller levers were found in the full throttle and high rpm positions, respectively.
On impact, the right wing leading edge made an imprint in the snow, then rotated rearward nine feet, as measured at the wing tip. The fuel cells in both wings ruptured and fuel sprayed forward in front of the left wing and aft behind the right wing, as evidenced by fuel stains in the snow. This indicates that the aircraft was rotating in a clockwise direction on impact. The wings remained on the ice surface on top of the partially submerged fuselage.
The empennage was intact, but impact forces had driven the horizontal stabilizer forward a distance sufficient to fracture the rudder tab actuating rod that drives the rudder trim mechanism. The trunnion nut on the rudder tab actuating rod was found one turn from the upper limit of travel. The leading edge of the horizontal stabilizer had accumulated 1/16 to 1/8 inch of rime ice. Because of the impact damage to the wings, it could not be determined whether or not a similar amount of ice had accumulated on the leading edge of the wing.
1.12.2 Instrument Examination
The TSB Engineering Branch examined the airspeed indicator and the gyro suction gauge to determine their indications at impact. The instrument face of the airspeed indicator showed two impact marks, one in the range of 126 to 128 knots and the other at approximately 119 knots.
On the gyro suction gauge, the left vacuum red inoperative button (left engine) was captured behind the dial face in the retracted position. The right button (right engine) was in the extended position. A minimum pressure of one inch of mercury is required to retract the button to the retracted position.
1.12.3 Instrument Lights
The lighting on the right side of the instrument panel and on the overhead panel was reportedly unserviceable, leaving only the left-side instrument panel lights. A passenger on the inbound trip to Tuktoyaktuk, who was seated behind the right front seat, reported that the pilot was using a flashlight to view the right side of the instrument panel. Extensive damage to the electrical system precluded testing of the lighting system. There was no record of the defect in the aircraft journey log or maintenance records.
1.12.4 Stall Warning
The aircraft was equipped with a pre-stall warning system to provide both an aural and visual signal at a speed between four and eight knots above the stall speed. It was reported that the pre-stall warning device was unserviceable while airborne, but worked on the ground when tested by maintenance personnel. There was no record of the defect, or of corrective action taken, in the log-books or maintenance records. After the accident, the device could not be tested due to the extensive damage to the leading edge of the wing and the electrical system. The stall warning was not audible on the FSS magnetic tape recording.
1.12.5 Engine and Propeller Examination
The TSB Engineering Branch analyzed the magnetic tape from the Tuktoyaktuk FSS to determine propeller rpm during the flight. The spectral analysis indicated that both engines were operating at a propeller speed of approximately 2,355 rpm when the pilot reported airborne at 1706:34, and that one engine was operating at 2,640 rpm when the pilot reported he had an engine problem at 1710:40. During the several transmissions made by the pilot between 1710:40 and 1713:03, the propeller rpm ranged from 2,561 rpm to 2,642 rpm.
Both engines were dismantled and examined at the Regional wreckage examination facility by TSB personnel, with an observer from Textron Lycoming in attendance.
The left engine showed no evidence of pre-impact damage. No mechanical defects were found that would have prevented the engine or accessories from normal operation. Examination of the left propeller revealed that the blades were in the low pitch (high rpm) position at impact.
Examination of the right engine accessory section found the main crankshaft drive-gear bolt- threads stripped, and the alignment dowel pin sheared. The crankshaft drive-gear drives all the engine accessories, including the two Bendix magnetos, through idler gears and magneto drive gears. Gear teeth were missing from the left idler gear and magneto drive gear. An impulse coupling flyweight, mounted on the end of the left magneto, was found jammed against the stop pin mounted on the magneto housing.
1.12.6 Engine Magneto
The right engine was fitted with two Bendix magnetos (S6LN-1227). The left magneto had excessive wear between the flyweight and axle pin, which allowed the flyweight to extend and jam against the case-mounted stop pin. The sudden stoppage of the magneto overloaded the secondary gear train for the left magneto, sheared the alignment dowel, and stripped the retaining bolt threads on the main crankshaft drive gear. When the crankshaft drive gear stopped, all the accessories stopped, including the right magneto.
The impulse coupling consists of two flyweights and spring assemblies which are part of the magneto drive coupling (see Figure 1). During engine starts, the toe of the flyweight contacts a stop pin on the magneto housing, preventing the magneto from turning. As the engine turns, the magneto drive gear winds the spring until it releases and rotates the magneto rapidly to send a very intense spark to the sparkplug. As engine rpm increases, centrifugal force pulls the tail of the flyweight outward, which rotates the toe inward, preventing the toe of the flyweight from contacting the stop pin.
The flyweight pivots on an axle, which, if worn excessively, will permit the heel of the flyweight to strike the stop pin and eventually jam. The clearance between the flyweight and axle pin was found to be worn beyond the prescribed limits of .016 inches. The side-play between the axle pin and the flyweight that jammed was found to be .046 inches, and between the opposite axle pin and the flyweight there was .076 inches. The area between the heel and the toe of the flyweight exhibited an indentation that corresponded with a groove worn in the stop pin.

1.12.7 Service Bulletins and Airworthiness Directives
Bendix Service Bulletin (SB) 599B (which is applicable to this magneto), issued July 1982, specified that the magneto inspection must occur after no more than 475 operating hours since new or overhaul, and at 500-hour intervals thereafter. The SB provided detailed instructions on checking the clearance between each impulse coupling flyweight and each stop pin to determine axle wear. The minimum specified clearance between the axle and flyweight was .016 inches. Teledyne Continental Ignition Systems SB 599D, issued January 1992, required that the inspection interval be 100 hours. Textron Lycoming issued a mandatory SB 425B, March 1992, that required compliance with Teledyne Continental SB 599D.
The SBs were mandated by Airworthiness Directive (AD) 78-09-07 R3, 17 January 1983, which required all S-1200 series magnetos incorporating impulse couplings to be removed, inspected, and replaced if necessary, in accordance with Bendix SB 599B or a Federal Aviation Administration (FAA) approved equivalent. The AD required that the compliance time, magneto make, model, and serial number be entered in the log-book after the work was accomplished.
No entries were found in the log-book of C-GMOP to indicate that AD 78-09-07 R3 or the SBs were complied with. A maintenance worksheet dated 10 July 1993contained an entry that Lycoming SB 425 was "done"; however, there was no reference to the compliance time, magneto make, model, or serial number.
The history of the failed magneto could not be definitely determined since the serial number on it (86510049) was not consistent with the serial number (8651004) recorded on the engine overhaul sheets. On the manufacturer's metal data tag, affixed to the magneto, the top portion of the last digit appeared to be a "9", but was not clearly identifiable as a figure nine. The three other magneto serial numbers were traceable back to the last overhaul. According to the engine times since overhaul recorded in the log-books, the magneto had approximately 1,478 hours in service with no record of an inspection of the magneto impulse coupling. Despite the ambiguity in the record keeping on the failed magneto, all evidence points to its having been continuously installed on the engine since the overhaul 1,478 hours before.
1.12.8 Aircraft Controls Examination
The control surfaces were accounted for, and all damage was attributable to the severe impact forces. Control cable continuity was checked to the extent possible, and no abnormalities were found. The flaps were in the up position at impact.
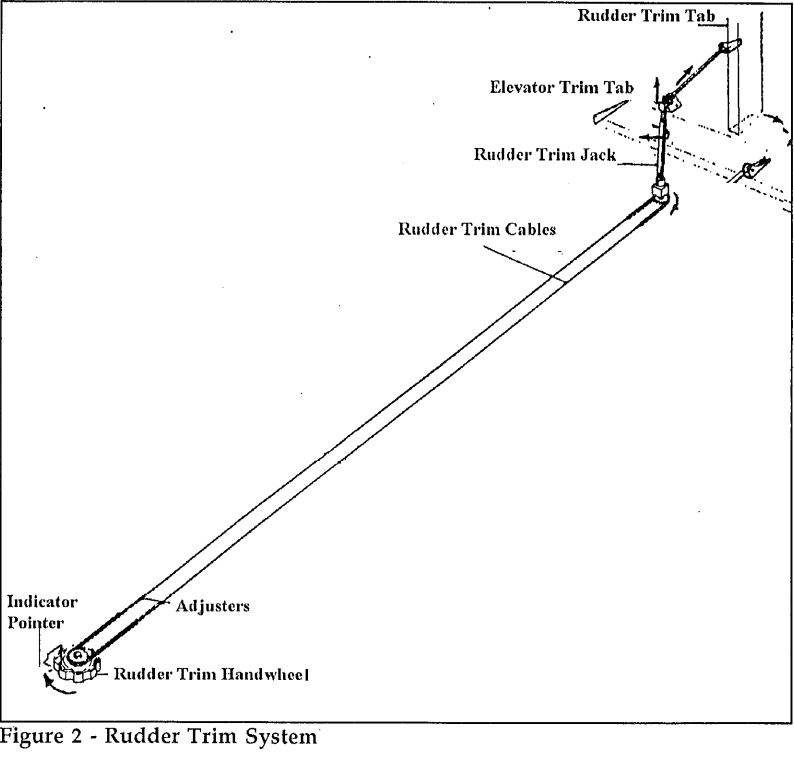
The Islander rudder trim system is conventional, in that rotating the trim wheel moves a rudder tab which displaces the rudder in the appropriate direction while in flight (see Figure 2). The rudder trim system is operated by a trim wheel on the cockpit ceiling. A pointer located forward of the trim wheel indicates the rudder trim setting. The trim wheel is connected to the rudder tab actuating mechanism in the tail of the aircraft by a chain and cable system. Turning the trim wheel counter-clockwise (as viewed from the pilot seat) moves the trim tab left and rudder to the right; opposite rotation moves the trim tab to the right and rudder left, in flight.
The rudder trim tab is actuated by a tubular rod assembly. The lower end is supported by a bearing housing mounted on the front of the horizontal stabilizer spar, and an upper bracket mounted on the rudder spar. The top end of the rod is threaded and rotates in a trunnion nut that moves up or down, depending on which direction the trim wheel is rotated. The trunnion nut is linked to and actuates the rudder tab by a lever and rod assembly. With the rudder tab in the neutral position, the trunnion nut is positioned approximately midway on the threaded rod end. The trunnion nut was found one turn from the upper limit of travel, positioning the rudder tab to the left.
Examination of the actuating rod and associated linkages to the rudder tab revealed that the lower end of the rod was bent forward and fractured at the base of the rudder, above the lower bearing housing on the horizontal stabilizer. The fracture surfaces on the ends of the rod indicate that the rod was bent forward approximately 40 degrees before fracturing. The bending occurred as the horizontal stabilizer was jammed forward during the impact sequence.
1.12.9 Rudder Trim Operation
Islander pilots interviewed after the accident related that they frequently rotated the trim wheel the wrong direction, initially, when trimming for an engine shutdown situation during practice sessions. However, the error was readily identified by feedback through the rudder pedal onto the foot. Rudder pedal foot pressure increases if the rudder trim wheel is rotated the wrong way and, conversely, foot pressure decreases if the trim wheel is rotated correctly. They reported that the aircraft required a 1/4 to 1/3 turn on the trim wheel to neutralize the rudder pressure during simulated engine-failure training exercises.
Other types of aircraft fitted with rudder trim systems differ in where the trim wheel is located. Aircraft that have the trim wheel located in front of the pilot require the pilot to reach forward and rotate the trim the direction he wants the aircraft to go. If the pilot wanted to turn the aircraft to the right, he would rotate the rudder trim wheel clockwise (from above); if the pilot wanted the aircraft to turn to the left, he would rotate the rudder trim wheel counter-clockwise (from above). Because the occurrence aircraft had the rudder trim wheel located on the ceiling, above the pilot's head, the wheel had to be gripped with the palm up; therefore, rotating the trim wheel counter-clockwise (from below) turned the aircraft right and, conversely, rotating the trim wheel clockwise (from below) turned the aircraft left.
1.13 Medical Information
Although medication inhalers for the treatment of asthma were found in the pilot's pockets, there was no evidence that he was suffering from an asthma attack at the time of the crash. There were no other natural disease processes identified that would have caused or contributed to the accident. The toxicological tests for ethanol and carboxyhemoglobin were entirely negative.
1.14 Fire
There was no evidence of fire either before or after the occurrence.
1.15 Survival Aspects
The pilot's seat was not equipped with a shoulder harness. The impact deceleration forces were of a magnitude considered to be non-survivable. Calculations of the deceleration load factors were in the range of 55 to 63 G's; however, the peak load factors would have been higher.
The emergency locator transmitter (ELT) activated on impact, and facilitated locating the wreckage.
1.16 Tests and Research
1.16.1 Britten-Norman Test Flight
A Britten-Norman test flight, on a similar Islander, determined that a foot-force of approximately 250 pounds on the left rudder was required to maintain a heading at an IAS of 65 to 75 knots with maximum throttle (2,700 rpm) on the left engine, the right engine shut down, right propeller feathered, and full nose right rudder trim applied.
1.17 Additional Information
1.17.1 Company Operations
Arctic Wings and Rotors commenced operations in 1991. The company received its operating certificate for a Domestic Non-Scheduled and International and Specialty Air Service with single and multi-engine aircraft on November 1993. The approved points were Inuvik, Aklavik, and Tuktoyaktuk, Northwest Territories. The operating certificate authorized day VFR operations from the company's main operational base at Inuvik Townsite, and IFR/night VFR from the Inuvik Airport.
At the time of the accident, the company operated a Cessna 185, a Cessna 207, two Britten Norman Islanders, a Piper PA-31 Navajo, a Piper PA-32 Cherokee Six, and a de Havilland DHC- 3 Single Otter.
The company was authorized by TC, as an Approved Maintenance Organization (AMO), to perform maintenance, other than specialized work, on commercially operated company aircraft, in accordance with the Airworthiness Manual.Chapter 573. The Maintenance Control Manual.(MCM) was approved by TC on 12 March 1991. At the time of the accident the company employed two licensed aircraft maintenance engineers (AME).
1.17.2 Maintenance Management
A TC operational audit was completed on 26 November 1993. The last TC maintenance audit before the occurrence was in November 1992. Several of the maintenance audit findings related to non-conformance with the procedures outlined in the MCM.
Some of the problems which had been highlighted by the audit findings were still present during the occurrence investigation. Maintenance records were found to be incomplete, and flight-crew-initiated aircraft defects were not being recorded in the aircraft log-books. Recent examples of items reported as not working, or items not being recorded in the aircraft log-book at some time prior to the accident flight, are as follows: the stall warning was not functioning in the air; the right side instrument panel and overhead lights were not functioning; and compliance with the ADs and component SBs was not being entered in the aircraft log-books.
MCM Section 4.2 requires that the pilot-in-command enter into the aircraft journey log any defect which develops so that maintenance personnel can rectify or defer the defect, depending on whether the defect is an airworthiness or non-airworthiness item, before further flight.
Maintenance records of recurring defects between inspections and correction action taken were not completed by maintenance personnel.
Periodic Britten-Norman SBs were recorded in C-GMOP's log-book; however, applicable ADs and component SBs were not.
MCM Section 4.8 requires ADs and SBs to be complied with as directed by the issuing authority, and entered in the appropriate log-books as prescribed by ANO Series VII, No. 2 and No. 3, and the Airworthiness Manual, Chapter 575.
Airworthiness Manual.AMA 593/1 para 3.2 states, "Failure to comply with an airworthiness directive will cause the Certificate of Airworthiness to be out of force and make it an offence to fly the aircraft."
Records of the TC audits were examined to determine why some audit findings had not been corrected. It was noted that the operator had completed the Corrective Action section of the Non-Conformance Finding Forms to indicate that shortcomings had been corrected. At the time of the investigation, the corrective action had not taken place.
TC has conducted an audit since the accident, in February 1994.
1.17.3 Pilot Duty Times
ANO VII, No. 3, 42.1 prescribes the maximum flight time, maximum flight duty time, and minimum rest period for flight crew members as follows:
(4) The maximum flight times for a flight crew member are
(a) 120 hours of flight time in any period of 30 consecutive days;
(b) 300 hours of flight time in any period of 90 consecutive days;
(c) 1,200 hours of flight time in any calendar year.
(5) The maximum flight duty time for a flight crew member is 15 hours in any period of 24 consecutive hours.
(9) ...a minimum rest period that allows flight crew to obtain
(a) adequate rest prior to flight duty time, calculated by taking into account the number and type of flight crew duties that precede and follow the rest period; and
(b) at least one rest period of not less than 24 consecutive hours
(i) once each seven day period, or
(ii) 13 times within each calendar quarter.
1.17.4 Pilot Fatigue
A 1986 report by the Canadian Aviation Safety Board, (CASB) entitled Fatigue-Related Accidents and Crew Flight Time and Duty Limitations, found that, of any category of fixed-wing operations, commercial charter operators had the highest average 90-day and 30-day flight times. The report identifies two forms of fatigue: acute and chronic.
Acute fatigue results from intense flying activities over a relatively short period which usually involves multiple tasks repeated regularly.
Chronic or long-term fatigue is defined as fatigue resulting from the accumulation of long flight and duty times acquired over an extended period.
According to the CASB study, pilot fatigue can, after an emergency or abnormality is detected, lead to errors in judgement.
1.17.5 Transfer Errors
A pilot who is current on different aircraft types could be prone to the misapplication of procedures or habits from one type to the next, or the incorrect operation of controls if the control operates differently; these errors are more commonly known as "transfer" errors. Transfer errors are more likely when a person is operating under stressors such as fatigue, or emergency situations.
2.0 Analysis
2.1 Introduction
The analysis will focus on maintenance management, the engine failure, the aircraft altitude and position at the time of engine failure, the pilot's reactions, fatigue, the aircraft rudder trim, the loss of control, and pilot training.
2.2 Maintenance Management
Some of the deficiencies identified during the 1992 TC audit were apparent during the occurrence investigation. Aircraft defects were not being consistently recorded in the aircraft log-books; nor were there records to show the status of recurring defects between inspections. Compliance with ADs and component SBs was not being entered in the aircraft log-books as required under ANO VII, No. 2 and No. 3, and the Airworthiness Manual, 575. Had the magneto impulse coupling inspection been completed as required by AD 78-09-07 R3, the wear patterns could have been detected and rectified before the magneto failed.
Although TC audits had identified such shortcomings and the company had reported corrective action, many of the shortcomings were still present at the time of the accident.
2.3 The Engine Failure
The magneto impulse coupling flyweights were worn beyond the prescribed limits. When the flyweight jammed against the stop pin, the secondary gear train failed and the engine stopped abruptly.
2.4 Altitude and Position on Departure
The altitude and position of the aircraft when the pilot encountered the engine problem could not be determined with certainty. The pilot did not report his altitude during the transmissions with the FSS.
On the inbound trip from Inuvik, the pilot remained below the cloud base and, if he followed his past flying habits, he likely would have remained below the 1,100-foot cloud layer for the return trip.
The thin layer of rime ice on the tail of the aircraft could have accumulated either inbound to Tuktoyaktuk, or on the departure. The possibility also exists that the pilot could have inadvertently entered cloud while handling the emergency.
2.5 Pilot Reactions
Two scenarios were studied to help understand why the pilot was unsuccessful in flying the aircraft back to the airport on one engine. There was no way to determine which of the two scenarios is more likely; however, it is clear from the evidence that the aircraft was not in controlled flight when it hit the ice.
The first scenario examines the possibility that the pilot climbed into or above the cloud layer. If this were the case, the lower cloud bases at Inuvik would likely have necessitated an IFR approach to the Inuvik Airport, after which the pilot could have continued VFR to the townstrip. While the pilot held an IFR rating, the aircraft was not equipped with an autopilot and, since there was only one pilot on board, IFR would have contravened ANO VII, No. 3.
The second scenario examines the possibility that the pilot remained VFR below the clouds. The lights from the Tuktoyaktuk Airport and hamlet would have been behind him. In this case, he would have had few visual references and little or no horizon to provide attitude reference. If he was successful in turning the aircraft toward the airport, with the reported 15 miles visibility, the lights should have become visible. If he turned the aircraft using the ground lights as a visual reference, and if he was, at the same time, preoccupied with carrying out the engine failure emergency procedures, he could have become disoriented and lost control of the aircraft. However, it could not be determined how much of the turn back to the airport was accomplished.
Given the existing conditions and the fact that the pilot was instrument rated, it is concluded that he would have referred to the aircraft flight instruments while handling the emergency, and probably the GPS and/or the Tuktoyaktuk NDB for directional information.
2.5.1 Fatigue
The pilot reportedly had good sleep habits, and had adequate rest the previous night. His duty day and flight times on the day of the accident were within established limits. However, according to the aircraft log-books, his most recent non-flying day was 11 November, 22 days prior to the accident. During the last four-month period there were 13 days when he did not fly. ANO VII No. 3 specifies one rest period of at least 24 hours in each seven-day period, or 13 times each calendar quarter.
Typically, small air carriers do not have a clearly delineated policy that distinguishes between "rest days" and non-flying days. Frequently, pilots may not be scheduled to fly on a certain day, but are available if needed for flying and/or related duties.
It could not be determined if the pilot's work schedule during the last four months led to some degree of fatigue which could have affected his judgement and reactions to the emergency.
2.6 Aircraft
2.6.1 Stall Warning and Instrument Lighting
It could not be determined to what extent, if any, the apparent unserviceability of the stall warning and the cockpit lighting affected the pilot's performance. However, if he needed to refer to the rudder trim indicator on the overhead panel, it would have been difficult to read the indication if he was not using his flashlight.
2.6.2 Single-Engine Procedures/Performance
The throttle and propeller controls were found in a position that would indicate that the pilot properly identified the failed engine and followed the emergency engine shutdown procedure.
According to the manufacturer's calculations, at a gross weight of approximately 6,200 pounds (400 pounds below the maximum gross weight), and a C of G of approximately 23.9 inches aft of datum, the aircraft would have been capable of returning to the airport on one engine.
Based upon information received from the manufacturer concerning aircraft performance in icing conditions, it is concluded that 1/16 to 1/8 inch of ice on the leading edge of the wings and the horizontal stabilizer would not have played a significant role in the loss of control.
2.6.3 Rudder Trim
With the right engine inoperative and the left engine operating, the aircraft would have a tendency to yaw and roll into a turn to the right. The pilot would have had to apply constant foot pressure on the left rudder to stop or limit the yaw and roll. To relieve the foot pressure on the rudder pedal, the pilot would normally rotate the rudder trim wheel in the appropriate direction.
Normally pilots rely on feedback through the appropriate rudder pedal onto the foot to confirm whether they are applying rudder trim in the appropriate direction. This method of control feedback is reliable if the aircraft is in level flight, but can be misleading if the aircraft is already in a turn when the trim selection is made. It is not known why the pilot did not correctly interpret the rudder feedback; however, the evidence suggests that he rotated the trim wheel in the direction that would yaw and roll the aircraft to the right rather than left. With the trim wheel mounted on the ceiling, above the pilot's head, it is more difficult to determine which way to turn the trim wheel.
The investigation attempted to determine what effect, if any, being current on five aircraft types, one of which had a rudder trim which was mounted on the overhead panel, might have had on any tendency to make an incorrect trim selection. While no direct link could be established, intuitively one would expect that this situation would increase the likelihood of making an incorrect trim selection on the BN2A, especially when under the stress of responding to an engine failure. Since other Islander pilots, interviewed after the accident, related that they frequently rotated the trim wheel in the wrong direction initially while trimming for an engine shutdown during practice sessions, the installation design itself is probably creating some confusion.
Once the pilot made an incorrect trim input and did not recognize the error, possibly because he may have been preoccupied with other tasks, he could have attributed the aircraft's right turning/rolling movement to thrust created by the operating left engine and an inoperative right engine. As the airspeed decreased, the rudder would have become less effective and the turning tendency greater; if subsequent trim applications continued in the wrong direction, eventually the aircraft would have rolled to the right and/or stalled.
2.6.4 The Loss of Control
The Britten-Norman test flight report demonstrated that, to maintain heading, approximately 250 pounds of foot/leg pressure was required on the left rudder pedal to overcome the combined forces of a mistrimmed rudder and asymmetric thrust created by the operating left engine and failed right engine. If the foot force on the rudder was relaxed and ailerons were used to counter the right roll, there would have been a large increase in drag, a decrease in airspeed and climb capability, and a loss of control.
The wreckage impact marks indicated that the aircraft was rotating to the right on impact with the snow-covered ice surface.
2.7 Pilot Training and Workload
The pilot had flying experience typical of pilots who fly for small commercial operators. He had completed the normal periodic training and proficiency checks required by his company; however, he did not receive on-type night training as required by TC. Considering the workload demands by this type of emergency on a pilot flying alone, it is questionable whether the 1.5 hours per year of training required by TC's ANO VII, No. 3 would have adequately prepared the pilot for the situation.
Transport Canada's policy allows the grouping of aeroplanes which have similarities in handling and performance. However, the BN-2 Islander and the PA-31, which were so grouped, have substantially different handling and performance characteristics. There are fundamental differences in cockpit layout and its systems. Therefore, it is unlikely that a demonstrated proficiency on one of these aircraft types would ensure proficiency on the other.
The recent preparation for and completion of the PPC on the Navajo may have contributed to a "transfer error" by reinforcing a rudder trimming action inappropriate to an engine failure in an Islander.
For commercial multi-engine IFR operations, ANO VII, No. 3, requires two pilots, or one pilot and a two-axis autopilot. These requirements recognize the more demanding nature of aircraft control by reference to instruments during periods of peak workload. Night VFR flight over featureless terrain and without a visible horizon--the environment for the accident flight--is at least as demanding of instrument flying skills.
3.0 Findings
- The pilot was licensed in accordance with existing regulations.
- The right engine lost all power within four minutes after the aircraft took off, when the left magneto impulse coupling jammed.
- The magneto impulse coupling flyweight-to-axle clearance was found to be worn beyond the manufacturer's prescribed limits.
- There was no evidence found that Bendix SB 599B or AD 78-09-07 R3, requiring magneto inspection at 500-hour intervals, had been complied with.
- Periodic Britten-Norman SBs were recorded in C-GMOP's log-book; however, applicable ADs and component SBs were not. Airworthiness Manual.AMA 593/1 states that when an AD is not complied with, the Certificate of Airworthiness is not in force.
- Shortcomings identified by a 1992 TC maintenance audit were still present at the time of the accident.
- The rudder trim mechanism was found in the nearly full-right rudder position, opposite to the direction required for a right engine failure.
- The foot force required on the left rudder pedal to overcome the combined forces of the rudder trimmed to the right and right engine drag was demonstrated to be approximately 250 pounds.
- The ice accumulation on the aircraft would not have played a significant role in the loss of control.
- The pilot had not received the on-type night flying training required by ANO VII, No. 3.
- Because of the absence of visual cues at the time of the engine failure, it is likely that the pilot had to fly the aircraft by reference to flight instruments.
- Considering the workload demand on a single pilot when dealing with this type of emergency at night, the 1.5 hours per year of training required by Transport Canada is considered inadequate.
- While it cannot be determined that fatigue contributed to this accident, the pilot's recent work schedule was conducive to fatigue.
- The crash impact forces were not survivable.
- The ELT functioned and facilitated in locating the aircraft.
3.1 Causes
A magneto impulse coupling, worn beyond the prescribed limits, resulted in the failure of the right engine. Following the engine failure, the pilot mistrimmed the rudder and was unable to maintain control of the aircraft.
4.0 Safety Action
4.1 Action Taken
4.1.1 Magneto Inspection
In March 1994, the TSB forwarded an Aviation Safety Advisory to TC regarding magneto inspection and maintenance requirements. In response, TC sent a letter to the FAA querying whether AD 78-09-07 R3 would be amended to include the more stringent periodic inspection requirement of SB 599D. There has been no reply to date. This matter was also featured in TC's Aviation Safety Maintainer .ewsletter, issues 3/94 and 1/95.
4.1.2 Mandatory Service Bulletin MS645
On 04 April 1994, Teledyne Continental issued Mandatory Service Bulletin MSB 645, which superseded SB599D. The reason for the bulletin was to decrease operational wear rates on impulse couplings and to prevent engine stoppage. The bulletin requires 100-hour inspections of riveted impulse couplings. Couplings which do not meet the detailed coupling inspection criteria are to be replaced with new snap ring assemblies.
4.1.3 Regulatory Audits and Surveillance
Analysis and information from this and 18 other accidents led to the identification of shortcomings in the regulatory overview process of air carriers. In particular, it was found that TC's audits sometimes lacked depth, and that the verification of corrective action following the audits was sometimes inadequate. Therefore, the Board recommended that:
The Department of Transport amend the Manual of Regulatory Audits (MRA) to provide for more in-depth audits of those air carriers demonstrating an adverse trend in its risk management indicators;
Transportation Safety Recommendation A94-23
The Department of Transport ensure that its inspectors involved in the audit process are able to apply risk management methods in identifying carriers warranting increased audit attention;
Transportation Safety Recommendation A94-24
The Department of Transport develop, as a priority, a system to track audit follow-up actions;
Transportation Safety Recommendation A94-25
The Department of Transport implement both short and long term actions to place greater emphasis on verification of required audit follow-up action and on enforcement action in cases of non-compliance.
Transportation Safety Recommendation A94-26
In response to these recommendations, TC has indicated that both recommendations A94-23 and A94-24 will be taken into consideration during amendments to the MRA. Also, TC will ensure that the Audit Procedures training program for inspectors takes into account recommendation A94-24 so that risk management methods are clearly understood and applied.
TC's reply to recommendations A94-25 and A94-26 indicates that the MRA will be reviewed to ensure that clear policy direction is given to ensure that effective audit follow-up systems are in place. Furthermore, TC intends to have an enhanced National Aviation Company Information System (NACIS) operational soon to track audit follow-up on a national basis. In the interim, a policy directive will be issued to regions to require a review of respective regional follow-up systems.
4.2 Action Required
4.2.1 Night VFR Commercial Operations
Commercial flights for aircraft of 12,500 pounds or less conducted under IFR are required to have either a crew of two pilots, or one pilot and a two-axis autopilot. These requirements recognize the demanding nature of maintaining aircraft control and situational awareness with reference to instruments only.
Night VFR flights over featureless terrain and without a visible horizon also demand instrument flying skills. As such, the regulatory requirements for commercial night VFR operations contain some safeguards; e.g., in consideration that the flight may temporarily encounter instrument meteorological conditions or poor ambient lighting, the pilot must be instrument rated; and to minimize the risk of collisions with terrain or obstacles, the flights must be conducted along airways, air routes, or approved company routes. However, these requirements do not address the added pressures placed on aircrew in severely deteriorated flight conditions or emergency situations.
Legally, night VFR commercial flights may be conducted with only one pilot and with no autopilot. The aircraft in this occurrence was certified for single pilot use in VFR operations, day or night; yet, this same aircraft used for commercial flight operations under IFR would have required two pilots. In the Board's view, coping single-handedly with weather diversions or an emergency during a dark night VFR flight would be very demanding, comparable to trying to handle these situations single-handedly on an IFR flight. However, on an IFR flight, another pilot would provide an added safety factor.
The differences in dispatching requirements for crew and in equipment requirements between commercial VFR and IFR flights are an economic consideration for operators. With VFR single- pilot crewing, manpower costs are lower; and the "nil" requirement for an autopilot reduces equipment and servicing expenses. Also, with VFR flight planning requirements for alternate airports and fuel reserves being less restrictive than the IFR requirements, the operator could have greater flexibility in meeting the routing and scheduling demands of his customers.
Although economic pressures are a factor to be considered by operators in the passenger- carrying business, from the fare-paying public's point of view, the level of safety should not be a function of the type of operation (i.e., VFR or IFR) or the time of day.
Aircrew in single-pilot commercial night VFR operations do not have the same level of safety back-up as their IFR counterparts in terms of equipment and crew requirements to safely cope with unforeseen situations. The Board is concerned that such night VFR flights do not afford the fare-paying public a level of safety equivalent to that on similar flights under IFR. Therefore, the Board recommends that:
The Department of Transport raise the regulatory requirements for the conduct of commercial passenger-carrying night VFR flights to provide a level of safety comparable to that provided on IFR flights with similar aircraft.
Transportation Safety Recommendation A95-16
4.2.2 Training
4.2.2.1 Night Training
In order to carry passengers at night on multi-engine aircraft, an operator is required to provide specific on-type night training for company pilots. The pilot in this occurrence had not received this training; nor had this shortcoming been detected by Transport Canada inspectors during the audit of the company's operation one month prior to the accident.
In January 1993, following the investigation of a twin-engine turbo-prop aircraft accident at Moosonee (TSB report A90H0002) in which neither of the pilots involved had received the required night training and the regional Transport Canada inspectors had not observed that the training had not been conducted, the Board recommended that:
The Department of Transport validate its current procedures for checking that air carriers provide the required multi-engine night training.
Transportation Safety Recommendation A93-05
TC responded in August 1993 that the Manual of Regulatory Audits.(MRA) (published since occurrence A90H0002) directed the audit staff to check the companies' flight training programmes. In addition, TC notified the regional Air Carrier staff of this matter and instructed its Quality Assurance Review team to ensure that the verification of night training did occur.
This occurrence is another example of a night accident in which the pilot had not received the required night training. Notwithstanding Transport Canada's continuing efforts to strengthen its processes for regulatory audit and surveillance, some commercial pilots are still not receiving the required night training. Since the skills required for safe night operations require reinforcement through periodic night training, the Board recommends that:
The Department of Transport conduct a special one-time audit to confirm that commercial pilots involved in night multi-engine operations are receiving the required night training.
Transportation Safety Recommendation A95-17
While TC audit procedures continue to miss inadequacies in the night training of commercial pilots, it is recognized that TC inspectors cannot be continuously on site to ensure that operators are providing this training. Individual operators must be held accountable for any failure to provide mandatory training. Therefore, the Board recommends that:
The Department of Transport evaluate the effectiveness of its current practices for dealing with those operators who are not providing mandatory training for pilots.
Transportation Safety Recommendation A95-18
4.2.3 Aircraft Grouping for Pilot Proficiency Checks (PPC)
TC had authorized the grouping of the Islander and the Navajo aircraft for PPCs for this operator. (The grouping of these two aircraft has reportedly been authorized at other carriers as well.) The policy regarding the grouping of aircraft for PPCs requires only that the aircraft be grouped according to performance and handling characteristics. However, significant differences apparently exist in both the handling characteristics and performance of the Navajo and Islander aircraft. Differences in the direction of application of the rudder trim between the two aircraft may have been critical in this accident.
The Board understands the desirability for operators to group aircraft for the conduct of PPCs. However, the Board believes that guidelines for the grouping of aircraft must ensure that a proficiency check on one aircraft of a group will consistently be an accurate indicator of pilot proficiency on other aircraft in the same group. Inappropriate groupings may lead the pilot, operator, and flight examiner to believe that the pilot's ability to handle all aircraft in the group is better than it actually is; such pilots will be vulnerable to encountering situations beyond their demonstrated capabilities. Therefore, the Board recommends that:
The Department of Transport confirm the suitability of all existing PPC aircraft groupings such that proficiency on one type is truly representative of all aircraft in the grouping.
Transportation Safety Recommendation A95-19
A pilot who is current on several aircraft types is prone to applying the specific procedures or practices for one type to another; this includes the possible incorrect operation of controls if the control functions are significantly different from one aircraft to another. Such errors in the performance of an operation or procedure are known as "transfer errors." Individuals are more susceptible to transfer errors during periods of stress caused by high workloads. The incorrect application of rudder trim during an engine failure in a multi-engine aircraft would be a typical transfer error if the procedure to apply the trim varied significantly between different aircraft on which the pilot was current. Differences in cockpit layout, in the operation of flight and engine controls, in the major aircraft systems, and in the critical emergency procedures could promote transfer errors. To minimize aircrew susceptibility to making transfer errors, aircraft groupings should be based on more than general similarities in aircraft handling and performance. Therefore, the Board recommends that:
The Department of Transport revise the guidelines for grouping aircraft for PPCs to take into account the susceptibility to transfer errors by aircrew.
Transportation Safety Recommendation A95-20
Transport Canada has established an approved list of groups of aircraft for aircraft above 7,000 pounds Maximum Certified Take-Off Weight (MCTOW). It is understood that a comprehensive analysis of the differences and similarities between the aircraft in each group was conducted to ensure the compatibility of aircraft. Such an approved list is not available for commercial aircraft below 7,000 pounds MCTOW. Ad hoc groupings of aircraft based on superficial similarities between aircraft can lead to fundamentally dissimilar aircraft being grouped together (e.g., Navajo and Islander), creating conditions conducive to transfer errors under high cockpit stress. Therefore, the Board recommends that:
The Department of Transport, where practicable, establish an approved list of aircraft groupings for PPCs of aircraft having a Maximum Certified Take-Off Weight (MCTOW) of under 7,000 pounds.
Transportation Safety Recommendation A95-21
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, Chairperson John W. Stants and member Zita Brunet authorized the release of this report on , pending ratification by the full Board.
Appendices
Appendix A - Flight Locale - C-GMOP
Appendix B - Map of Flight Path - C-GMOP
Appendix C - List of Supporting Reports
The following TSB Engineering Branch reports were completed:
- LP 173/93 - FSS Recording Analysis;
- LP 16/94 - Instruments Examination;
- LP 6/94 - Crankshaft Bolt; and
- LP 63/94 - Impact Loads.
These reports are available upon request from the Transportation Safety Board of Canada.
Appendix D - Glossary
- AD
- Airworthiness Directive
- agl
- above ground level
- AME
- aircraft maintenance engineer
- AMO
- approved maintenance organization
- ANO
- Air Navigation Order
- AS
- runway end identification lights
- asl
- above sea level
- ATPL
- Airline Transport Pilot Licence
- C of G
- centre of gravity
- CASB
- Canadian Aviation Safety Board
- CVR
- cockpit voice recorder
- ELT
- emergency locator transmitter
- FAA
- Federal Aviation Administration
- FDR
- flight data recorder
- fpm
- feet per minute
- FSS
- Flight Service Station
- FTM
- Flight Training Manual
- G G
- load factor
- GPS
- global positioning system
- hr
- hour(s)
- IAS
- indicated airspeed
- IFR
- instrument flight rules
- IMC
- instrument meteorological conditions
- lb
- pound(s)
- LL
- low lead
- MCM
- Maintenance Control Manual
- MCTOW
- maximum certified take - off weight
- ME
- medium intensity runway lighting
- mi
- mile(s)
- MRA
- Manual of Regulatory Audits
- MST
- mountain standard time
- N
- north
- NACIS
- National Aviation Company Information System
- NDB
- non - directional beacon
- PPC
- pilot proficiency check
- rpm
- revolutions per minute
- SB
- service bulletin
- SE
- southeast
- TC
- Transport Canada
- TE
- threshold lights
- TSB
- Transportation Safety Board of Canada
- UTC
- Coordinated Universal Time
- VASIS
- visual approach slope indicator system
- VFR
- visual flight rules
- VMC
- visual meteorological conditions
- VMCA
- minimum single - engine control speed
- W
- west
- ′
- minutes(s)
- ″
- second(s)
- °
- degree(s)