Collision with Terrain
Transwest Air
Beech A100 King Air C-GFFN
Sandy Bay, Saskatchewan
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
Transwest Air Flight 350 (TW350), a Beech A100 King Air (registration C-GFFN, serial number B190), departed La Ronge, Saskatchewan, at 1930 central standard time under instrument flight rules to Sandy Bay, with two flight crew members and two emergency medical technicians aboard. TW350 was operating under Part VII, Subpart 3, Air Taxi Operations, of the Canadian Aviation Regulations. At 1948, air traffic control cleared TW350 out of controlled airspace via the Sandy Bay Runway 05 non-directional beacon approach. The crew flew the approach straight-in to Runway 05 and initiated a go-around from the landing flare. The aircraft did not maintain a positive rate of climb during the go-around and collided with trees just beyond the departure end of the runway. All four occupants survived the impact and evacuated the aircraft. The captain died of his injuries before rescuers arrived. Both emergency medical technicians were seriously injured, and the first officer received minor injuries. The aircraft sustained substantial damage from impact forces and was subsequently destroyed by a post-impact fire. The accident occurred at 2002 during the hours of darkness.
1.0 Factual Information
1.1 History of the Flight
1.1.1 Pre-Flight Preparation
At about 1830, Footnote 1 the Sandy Bay Health Centre contacted an ambulance dispatch centre to request air transport for a patient transfer from Sandy Bay, Saskatchewan, to Flin Flon, Manitoba. The ambulance dispatch centre called the Transwest Air (TWA) Footnote 2 duty officer at La Ronge, Saskatchewan, to confirm that a standby King Air aircraft and crew were available, and then dispatched two emergency medical technicians (EMTs) to the La Ronge Airport. The TWA duty officer immediately alerted the captain and first officer.
The captain and first officer met at the airport and divided the pre-flight duties. The captain obtained a weather briefing using a computer terminal in the company hangar and filed an instrument flight rules (IFR) flight plan to Sandy Bay with La Ronge as the alternate, using the call sign TW350. The first officer did a pre-flight inspection of the aircraft, computed a weight and balance using a handheld computer, and prepared the operational flight plan (OFP).
The captain was seated in the left seat and the first officer, in the right seat. During the after-start check, the captain designated the first officer as the pilot flying (PF) for the flight to Sandy Bay. The captain taxied the aircraft to Runway 36 while the first officer obtained the IFR clearance from La Ronge radio.
1.1.2 Departure, En Route, and Descent
TW350 departed La Ronge at 1930, with the first officer as PF and the captain as pilot not flying (PNF). After take-off, the captain contacted air traffic control (ATC) and TW350 was cleared to climb and maintain 11 000 feet above sea level (asl). The crew members completed the cruise power check upon reaching this altitude and advised ATC that they had levelled off at 11 000 feet. En route, the crew reviewed the 1800 Flin Flon weather observation.
In preparation for the approach, the first officer transferred control of the aircraft to the captain using the standard phrase in the standard operating procedures (SOPs) in order to review the Sandy Bay instrument approach procedure. The captain verbally indicated that he was accepting control of the aircraft from the first officer.
The first officer planned a straight-in approach to Runway 05 and the captain concurred with this plan. The first officer conducted a briefing for the non-directional beacon (NDB) approach to Runway 05. Footnote 3 The crew had the global positioning system (GPS) programmed direct to the Sandy Bay aerodrome (CJY4) waypoint from the GPS database, and the first officer planned to use the GPS distance to go to the aerodrome to establish a descent profile of 300 feet per nautical mile (nm). The captain transferred aircraft control back to the first officer following the approach briefing.
Approaching Sandy Bay, the captain broadcast an arrival advisory on 126.7 MHz. ATC cleared TW350 to depart controlled airspace via the Sandy Bay Runway 05 approach, with descent at the crew's discretion. After the captain acknowledged the clearance, the controller provided altimeter settings for The Pas (29.68 inches of mercury [in Hg]) and Lynn Lake (29.63 in Hg), and instructed TW350 to switch to en route frequencies. Shortly thereafter, the crew commenced the descent using the Lynn Lake altimeter setting.
The captain broadcast a second arrival advisory on 122.8 MHz and the crew activated the Sandy Bay aerodrome lighting. The crew descended and positioned the aircraft for a straight-in approach based on the 25-mile minimum safe altitude of 2600 feet and the minimum descent altitude (MDA) for the approach, 1780 feet.
1.1.3 Approach
The flaps were extended to the approach setting and the first officer called for the landing check about 5.5 nm from the aerodrome. The crew confirmed that the landing gear indicated down and locked, checked the brakes, and the captain indicated that the landing lights would remain off because the aircraft was still in cloud.
Approximately 4.5 nm from the aerodrome, the captain acquired visual reference with ground lighting at a hydroelectric dam and the town. Both crew members acquired visual reference with the aerodrome at about 4.2 nm from the runway while the aircraft was still in descent toward the MDA. On short final, another arrival advisory was broadcast and the propeller speed was set to high.
At about 3 miles final, the flaps were extended to the landing position. At 2.5 nm final, the aircraft was on profile for the approach and a determination was made by the crew members that they should be down to 600 feet above ground level (agl) by the time they reached 2 nm. At 2001:37, the crew turned on the landing lights.
At 2001:44, the captain identified that the aircraft was high on the approach, reduced the engine power to about 400 foot-pounds of torque, and began coaching the first officer to increase the aircraft descent angle. The captain's coaching continued and, at 2002:05, the first officer suggested that they conduct a go-around. At 2002:06, the captain instructed the first officer to continue the approach and the first officer focused on flying the aircraft to a landing. The captain continued to coach the first officer through the approach and into the landing flare. At 2002:15, the captain instructed the first officer to bring the power off and put the aircraft on the runway and, at 2002:18, the power was reduced to flight idle.
1.1.4 Go-Around
The captain decided to abandon the landing attempt and, at 2002:19, communicated this decision to the first officer. At 2002:23, the captain advanced the power levers to a high-power setting.
The first officer perceived pressure on the control column and observed the captain's hand on the control column. Believing the captain to be taking control, the first officer released the control column. Neither pilot verbally announced or acknowledged the transfer of control.
At 2002:29, the first officer called for flaps and gear to be retracted. At 2002:31, the captain called positive rate and gear up. At 2002:32, the first officer selected the landing gear up and then selected the flap lever to the UP position. The captain re-selected the flap lever to the approach setting. During the go-around, the first officer observed the altimeter indicating 100 feet below the aerodrome elevation, perceived sensations of being pushed back in the seat and the aircraft pitching up, and believed the aircraft was climbing. However, the aircraft did not maintain a positive rate of climb during the go-around, and it collided with trees at 2002:43.
1.2 Injuries to Persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | 1 | - | - | 1 |
| Serious | - | 2 | - | 2 |
| Minor | 1 | - | - | 1 |
| Total Injuries | 2 | 2 | - | 4 |
1.3 Damage to Aircraft
The aircraft was substantially damaged by contact with the trees and the ground, and was eventually destroyed by a post-impact fire.
1.4 Other Damage
Property damage was limited to the forest in the immediate area around the crash site, with some minor environmental damage caused by the spillage of fuel and the post-impact fire.
1.5 Personnel Information
1.5.1 General
| Captain | First Officer | |
|---|---|---|
| Pilot Licence | Airline Transport | Commercial |
| Medical Certificate Expiry Date | 01 March 2007 | 01 April 2007 |
| Total Flying Hours | 8814 | 672 |
| Hours on Type | 449 | 439 |
| Hours Last 90 Days | 104 | 127 |
| Hours on Type Last 90 Days | 104 | 127 |
| Hours on Duty Prior to Occurrence | 1.5 | 1.5 |
| Hours Off Duty Prior to Work Period | 15 | 15 |
1.5.2 The Captain
The captain held an airline transport pilot licence (ATPL) last issued by Transport Canada (TC) on 04 April 2006, valid for multi-engine land aeroplanes. The licence included type ratings for AJ25, BA32, DA10, and HS25 aircraft, and a Group 1 instrument rating valid until 01 April 2008. The captain also held a United States Federal Aviation Administration (FAA) airline transport pilot certificate issued on 16 August 1998 with a type rating for HS-125 jet aircraft.
The captain applied for employment as a La Ronge-based Beech A100 King Air captain with TWA on 28 April 2006, and subsequently moved to La Ronge, beginning employment with the company on 08 May 2006.
The captain received three training flights with a designated company training pilot, in a company Beech A100 King Air aircraft, from 10 May to 16 May 2006, comprising a total of 5.4 hours of flight time. During this period, the captain practiced normal, abnormal, and emergency checklist procedures on the ground with the training pilot in a King Air aircraft that was available for use as a cockpit procedures training device. The focus of the ground and flight training was to prepare the captain for the pilot proficiency check (PPC).
The training included flight planning, weight and balance, crew coordination, use of take-off and landing data charts, use of checklists, rejected and missed approaches, and controlled flight into terrain (CFIT) avoidance. The training emphasized the need to conduct stabilized approaches. The captain's flying skill level was initially considered to be lower than expected for his experience level, but his performance during the training was consistently rated as satisfactory, including familiarity, knowledge, application of SOPs, and pilot decision making. At the completion of the training, the captain was scheduled for the PPC.
On 16 May 2006, the captain passed an initial Beech A100 King Air captain PPC conducted by a designated approved check pilot (DACP). Prerequisite ground and flight training and exams were checked off as complete.
On 18 May 2006, the captain completed 20 hours of Beech A100 King Air ground school provided by a TWA-designated training pilot, covering the material specified in the company's flight crew training manual (FCTM). The investigation did not determine why the 16 May 2006 flight test report showed that ground training was complete when the ground training was not completed until 18 May 2006.
The captain began company line indoctrination on 23 May 2006 and received a total of 128.0 hours of flight time. During the line indoctrination, the captain flew with training pilots or other line captains. Line indoctrination records showed that the captain initially experienced difficulty in several areas, including pre-flight planning and IFR operations, but made steady progress and completed the line indoctrination program on 28 June 2006. The captain was then released to line operations and began flying with first officers. The company did not conduct any line checks on the captain and was not required to do so.
The captain's work schedule met the requirements of the flight duty time limitations and rest periods specified in the TWA flight operations manual (FOM). He had flown from 1600 to 2000 on 04 January 2007, did not fly on 05 January 2007, flew from 2200 on 06 January 2007 until about 0330 on 07 January 2007, and had been off duty from 0330 until 1800 on 07 January 2007. The investigation was unable to gather any information regarding the captain's sleep pattern before the accident. Between 01 October 2006 and the day of the occurrence, the captain had flown into Sandy Bay nine times during daylight and four times at night.
The captain was issued a private pilot licence in 1979, a commercial pilot licence and an instructor rating in 1980, instrument and multi-engine ratings in 1981, and an ATPL in 1983. The captain was employed as a flight instructor from 1980 to 1987, as a multi-engine IFR air taxi pilot on both piston and turboprop aircraft from 1984 to 1988, and as a turboprop commuter pilot from 1988 to 1991. From 1991 to 1995, the captain worked outside the aviation industry in non-flying occupations. From 1995 to 2003, he was employed by a succession of three Toronto-based air operators and flew the business jet aircraft for which he was type-rated. In March 2000, the captain completed a TC crew resource management (CRM) course. From October 2003 until May 2006, the captain again worked outside the aviation industry in non-flying occupations. During this period, he reportedly practiced take-offs and landings at an airport near his home and also practiced with a desktop computer flight simulator program. His only recent experience flying in northern Canada was with TWA.
The captain failed written and flight tests before initial issuance of the commercial pilot licence, multi-engine rating, and ATPL. In 1985, he passed an instrument rating renewal flight test on his fourth attempt. TC sent the captain counselling letters in 1983 regarding regulatory non-compliance, in 1984 regarding low-flying, and in 1985 regarding deficiencies in instructional technique.
From 1996 to 1998, the captain's employer reprimanded him four times for non-compliance with company policies and TC flight time duty limit regulations, and employed him only as a first officer. This employer provided the captain a letter of recommendation acknowledging his two years of employment as a first officer and stating that the captain had performed well.
In 2000, a second employer initially upgraded him to captain and later downgraded him to first officer because of repeated SOP non-compliance.
Later in 2000, the captain moved to a third employer and was briefly employed as a captain. Although he had been hired because he held a captain's PPC on an aircraft type the company operated, the third employer downgraded the captain to first officer and cited weak systems knowledge, pre-flight planning shortcuts, fixation on minor problems, dwelling on errors, narrow attention span, and poor decision making as reasons. In December 2002, this employer paid the captain a performance bonus. This employer reprimanded the captain in 2003 for sub-standard performance. Later in 2003, this employer refused to renew the captain's PPC because the captain's performance was unsatisfactory in the areas of crew coordination, CRM, and SOP compliance. In January 2004, the third employer provided the captain with a letter of reference stating that he had been employed as a captain for three and one-half years, that he was extremely knowledgeable about the aircraft he flew, and that, at times, he operated the aircraft in accordance with the SOPs.
Based on concerns regarding privacy legislation and the potential for legal action, the previous employers all indicated that they would not have disclosed the negative information about the captain's performance to prospective employers calling for a reference check.
1.5.3 The First Officer
The first officer held a commercial pilot licence last issued by TC on 17 May 2006 valid for multi-engine land aeroplanes. The licence included a Group 1 instrument rating valid until 01 June 2008.
The first officer was issued a private pilot licence in 2000, and was issued a commercial pilot licence with night, multi-engine, and instrument ratings following successful completion of an aviation college training program in July 2003. From August 2003 to March 2005, the first officer was employed by another air operator in northern Saskatchewan as a non-flying customer service agent.
The first officer was hired by TWA on 05 April 2005 and was employed by the company in non-flying jobs as an office assistant and dock/ramp agent based in La Ronge until March 2006. On 18 March 2006, the first officer completed 20 hours of Beech A100 King Air ground school provided by a TWA-designated training pilot, covering the material specified in the FCTM.
The first officer received four training flights with a company-designated training pilot, in company King Air aircraft, from 18 to 30 April 2006, comprising a total of 5.2 hours of flight time. The training included flight planning, weight and balance, crew coordination, use of take-off and landing data charts, use of checklist, rejected and missed approaches, and CFIT avoidance. The training included emphasis on stabilized approaches. The training go-arounds were initiated from about 100 feet agl on short final approach with landing flaps and landing gear extended. The first officer's performance during the training was consistently rated as satisfactory, with one exception. On the third training flight, steep turns were rated as unsatisfactory because altitude deviations were excessive. On the fourth training flight, steep turns were rated satisfactory.
On 03 May 2006, the first officer passed a Group 1 instrument rating renewal flight test and PPC conducted by a company check pilot (CCP) in a company Beech A100 King Air. Prerequisite ground and flight training and exams were checked off as complete. On 04 May 2006, a company-designated training pilot certified the first officer as competent on Beech A100 King Air aircraft.
The company was not required to provide line indoctrination for first officers, and the first officer did not receive any line indoctrination before beginning operations with line captains in May 2006. The company did not conduct any line checks on the first officer and was not required to do so.
In June 2006, the first officer made a night landing at Sandy Bay while flying with a different captain. Between 01 October 2006 and the day of the occurrence, the first officer was PNF on flights into Sandy Bay five times during daylight and three times at night. During these flights, the captain made the landings.
The first officer's work schedule met the requirements of the flight duty time limitations and rest periods specified in the TWA FOM. The first officer had flown from 1600 to 2000 on 04 January 2007, did not fly on 05 January 2007, flew from 2200 on 06 January 2007 until about 0330 on 07 January 2007, and had been off duty from 0330 until 1800 on 07 January 2007. The investigation did not gather any information regarding the first officer's sleep pattern before the accident.
1.5.4 Captain and First Officer Interaction
The captain and first officer occasionally used a non-standard transfer of control practice. The captain sometimes took control from the first officer using verbal phrases to do so, and sometimes physically took the controls without any verbal direction. The captain's verbal directions sometimes differed from the phrase specified in the SOPs, "I have control." On occasions when the captain did not make any verbal statement while taking control, the first officer responded by releasing the controls upon sensing pressure on the controls from the captain's control inputs.
The captain and first officer both preferred to fly with other crew members rather than each other, and about half of the company's King Air crew members were aware of this preference. Footnote 4 Some of the pilots were aware of a concern that the captain had about the first officer's landings, and were also aware that the captain had taken control from the first officer during several approaches and landings. The assessment of the other pilots was that the first officer's landings were somewhat inconsistent but improving as the first officer gained experience with the aircraft and the company's area of operations. They viewed the situation as one of a junior pilot gradually becoming more proficient, not as a hazardous situation, and they perceived the captain's concerns to be of a similar nature. None of the other pilots could recall the captain taking control from them without verbally indicating his intent first. One other pilot reported that the captain provided coaching during an approach to Prince Albert, Saskatchewan, in instrument meteorological conditions (IMC).
The captain and first officer flew together into Sandy Bay twice in the week before the accident, once during twilight and once during daylight. They had flown together the night before the accident, sharing the flight time between them by alternating legs as PF.
1.6 Aircraft Information
| Manufacturer | Beech Aircraft Corporation |
| Type and Model | A100 |
| Year of Manufacture | 1974 |
| Serial Number | B190 |
| Certificate of Airworthiness | Issued 10 January 1996 |
| Total Airframe Time | 17 066 hours |
| Engine Type (number of) | PT6A-28 (2) |
| Maximum Allowable Take-off Weight | 11 500 pounds |
| Recommended Fuel Types | Jet A, Jet A1, Jet B |
| Fuel Type Used | Jet A1 |
1.6.1 General
An examination of the aircraft's maintenance records indicated that the aircraft was maintained in accordance with the approved procedures in the company's maintenance control manual. The aircraft's last inspection was a phase 4 scheduled inspection program completed on 07 November 2006. The aircraft's next inspection was due in 40 hours. The aircraft's company maintenance worksheet indicated that there were no outstanding unserviceabilities. The aircraft was certified for visual flight rules (VFR) and IFR, day and night, in known icing conditions. The aircraft was not equipped with a ground proximity warning system or a terrain avoidance warning system, and was not required to be so equipped.
1.6.2 Weight and Balance
The aircraft departed La Ronge with 2600 pounds of fuel, at a take-off weight of about 10 833 pounds; the centre of gravity was within specified limits. En route fuel consumption was about 300 pounds and the landing weight was about 10 533 pounds.
1.6.3 Global Positioning System
The aircraft was equipped with a Trimble TNL 3000 GPS certified for IFR operations. The TNL 3000 uses a Jeppesen database with information about airports, navigational aids, and intersections.
The data source was the same for the Sandy Bay aerodrome geometric centre coordinates in both the TNL 3000 database and the Canada Flight Supplement (CFS). The TNL 3000 is capable of displaying the following data on one page: active waypoint, track to active waypoint, distance to active waypoint in nautical miles and tenths, groundspeed, and time to active waypoint in hours and minutes.
The GPS was destroyed in the post-impact fire and no data were retrieved.
1.6.4 Aircraft Flight Manual
Investigators calculated the landing distance required to be 1600 feet, without propeller reversing, on a paved, level, dry surface. The calculations were based on aircraft landing weight of 10 533 pounds, aerodrome elevation 1001 feet, and assumed weather conditions of −17°C, calm wind, and altimeter setting of 29.63 in Hg.
The normal procedures section of the Beech A100 King Air aircraft flight manual(AFM) does not include a go-around procedure, but does include the following balked landing procedure:
- Power – TAKEOFF
- Airspeed – BALKED LANDING CLIMB SPEED (when clear of obstacles ESTABLISH 100 knots)
- Flaps – UP
- Landing Gear – UP
The balked landing climb chart indicates that the aircraft should have been capable of climbing at about 1250 feet per minute (fpm) during the go-around. This chart assumes that take-off power is set, flaps are fully extended, and landing gear is down. Section 1.17.1.18 of this report describes the TWA SOPs for a go-around.
1.7 Meteorological Information
There are no weather reports available for Sandy Bay. The closest locations with aviation weather reports are Flin Flon, 57 nm southeast, Lynn Lake, 88 nm northeast, La Ronge, 105 nm southwest, and The Pas, 105 nm southeast.
A graphic area forecast (GFA) was issued at 1741 with a valid time of 1800. The GFA clouds and weather chart forecast a ridge of high pressure from southern Manitoba into central and northern Saskatchewan. The area around Sandy Bay, including Flin Flon, Lynn Lake, La Ronge, and The Pas, was forecast to have scattered clouds based at 2000 to 3000 feet asl and topped at 6000 feet asl, patchy ceilings at 1200 feet agl affecting 25 to 50 per cent of the area, visibility greater than 6 statute miles (sm), and local visibility greater than 6 sm in light snow affecting less than 25 per cent of the area. There were no GFA amendments issued for the area discussed.
The 1800 aviation routine weather report (METAR) for Flin Flon was as follows: wind 050° true (T) at 2 knots, visibility 15 sm in light snow, broken cloud ceiling at 2500 feet agl, temperature −12°C, dew point −13°C, altimeter setting 29.67 in Hg, remarks clouds stratocumulus 7 oktas, Footnote 5 last observation, next observation January 8 at 0600. The Flin Flon altimeter setting was 29.69 in Hg at 1700 and 29.70 in Hg at 1600. Flin Flon does not provide weather observations between the hours of 1800 and 0600.
The 2000 METAR for The Pas was as follows: wind calm, visibility 15 sm, a few clouds at 1800 feet agl, temperature −17°C, dew point −18°C, altimeter setting 29.68 in Hg. The 2000 METAR for La Ronge was as follows: wind 060°T at 2 knots, visibility 15 sm, a few clouds at 24 000 feet, temperature −18°C, dew point −20°C, altimeter setting 29.62 in Hg. The 2000 METAR for Lynn Lake was as follows: wind 300°T at 5 knots, visibility 9 sm, overcast cloud ceiling at 700 feet agl, temperature −17°C, dew point −20°C, altimeter setting 29.63 in Hg. The altimeter setting at Lynn Lake had been constant at 29.63 in Hg since 1800.
About three hours after the accident, the ceiling at Sandy Bay was estimated to be 700 to 800 feet agl by flight crews arriving to evacuate the survivors.
On the day of the occurrence, the end of civil twilight at Sandy Bay was 1721 and the moonrise was at 2143.
1.8 Aids to Navigation
An NDB, identifier 1W, was the sole navigational facility at the Sandy Bay aerodrome. The beacon is located at coordinates 55°32.6' N, 102°16.6' W, south of the apron and near the threshold to Runway 05. The Sandy Bay aerodrome lies beneath the base of NAV CANADA radar coverage and radar services were not available.
The company equipped the aircraft with one copy of the Canada Air Pilot (CAP) and one copy of the Restricted Canada Air Pilot (RCAP). Area navigation (RNAV) instrument approach procedures to runways 05 and 23 were published in the CAP and an NDB instrument approach procedure to Runway 05 was published in the RCAP. The CAP RNAV (GNSS [global navigation satellite system]) Runway 05 approach used a missed approach waypoint (RW05) coinciding with the threshold of Runway 05.
The RCAP NDB 05 procedure included an operational restriction requiring operations specification (OPS SPEC) 099 or 410 for use of the procedure (see section 1.17.1.2 for a description of OPS SPEC 099). All three approach procedures provided information regarding aerodrome lighting, and each procedure included three cautionary notes to pilots: to use the Flin Flon altimeter setting, that the Flin Flon altimeter setting was available during limited hours, and to verify that the runway was unobstructed.
1.9 Communications
A review of communications between TW350 and NAV CANADA air traffic services (ATS) determined that TW350 had not reported any problems with aircraft equipment or systems and there were no communication problems noted with the control agency.
Sandy Bay aerodrome is uncontrolled, with 122.8 MHz designated as the aerodrome traffic frequency. There are no ground communication facilities serving the aerodrome.
1.10 Aerodrome Information
The Sandy Bay aerodrome (CJY4) is an uncontrolled registered aerodrome operated by the Saskatchewan Ministry of Highways and Infrastructure and is used by unscheduled commercial and private operators. The Sandy Bay aerodrome is normally unattended and runway surface condition inspections are neither required nor conducted. At about 2115, the gravel runway surface was covered with a layer of compacted snow and a thin layer of fresh and unmarked snow, with no tire marks from the aircraft.
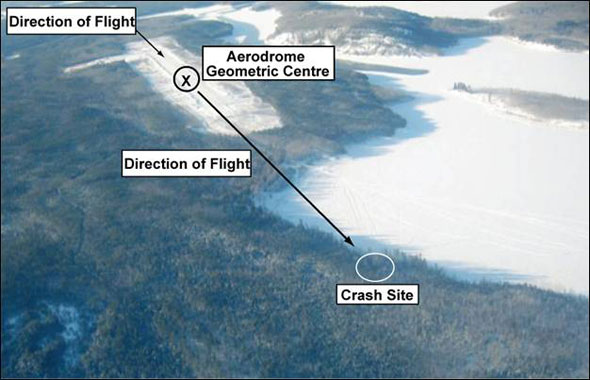
Runway 05/23 is at 1001 feet asl. Both the CFS and CAP show the runway as 2880 feet long and 75 feet wide with a treated gravel surface. The RCAP aerodrome chart shows the runway length as 2800 feet. This discrepancy has been brought to the attention of NAV CANADA. Beyond the departure end of Runway 05, the terrain descends to a bay on the Churchill River. The elevation of the river surface is 915 feet asl. The Sandy Bay aerodrome geometric centre coordinates published in the CFS correspond to a point on the centreline of the runway, 1440 feet or 0.237 nm from the thresholds of runways 05 and 23. The airspace from the surface to 2200 feet agl is Class G uncontrolled airspace. The overlying airspace associated with airway V357 is Class E controlled airspace from 2200 feet agl to 12 500 feet asl.
The aerodrome lighting was operated by Type J aircraft radio control of aerodrome lighting (ARCAL) and consisted of low-intensity runway edge lights, bi-directional threshold and runway end lights, and an aerodrome beacon. The aerodrome lighting was reported to be operating normally.
The Sandy Bay aerodrome is 1.2 nm northeast of the town of Sandy Bay and 2.3 nm northeast of a hydroelectric dam. There are no surface lights on the terrain surrounding the Sandy Bay aerodrome, with the exception of the hydro dam and town. Both the dam and town have extensive lighting systems that are clearly visible from the air at night when weather conditions permit.
The Sandy Bay aerodrome was not equipped with approach lighting, a visual approach slope indicator system (VASIS), or a precision approach path indicator (PAPI), and was not required to be so equipped. The aerodrome operator did not install a PAPI at runways less than 3800 feet long because the PAPI approach path ground point of interception (GPI) may be beyond a safe touchdown point for some aircraft using the runway.
The Sandy Bay aerodrome was constructed in 1981 for day VFR operations and was upgraded in 1990 with an aerodrome lighting system and an NDB to permit night and IFR operations.
1.11 Flight Recorders
The aircraft was equipped with a Universal Avionics Systems Corporation model CVR 30-B digital cockpit voice recorder (CVR), part number 1603-02-03, serial number 1242. The CVR was recovered from the empennage area and was partially melted and charred by the fire. The CVR was sent to the TSB Engineering Laboratory where the voice data stored in the recorder was recovered.
The aircraft was not equipped with a flight data recorder and was not required to be so equipped.
1.12 Wreckage and Impact Information
The wreckage was located in trees 2880 feet off the departure end of Runway 05 and approximately 50 feet right of the extended runway centreline. The aircraft track was 063° magnetic (M) when it struck trees near the river shore. The ground elevation at the initial tree strike was 1000 feet asl and the tree top had been cut off about 30 feet above the ground. The aircraft decelerated through the trees, striking the hillside at an elevation of 1040 feet asl and coming to rest approximately 365 feet from the initial tree impact. The swath through the trees indicates that the aircraft was in a nose-level attitude with 5 to 10° right-wing-low bank attitude at the point of initial tree impact.
The on-site examination found that all three blades on both propellers were damaged from contact with the trees and the ground. The damage was indicative of high rotational energy or engine power at impact. Both engines were destroyed by fire with only the heat-resistant components remaining. Continuity in the flight controls could not be established because of the severe destruction of the aircraft, although pieces of all the flight control surfaces were identified. The inboard flaps were still attached to the wing structure inboard of the engine nacelles; the flaps were partially extended. The right outboard flap actuator was measured and the dimensions were consistent with an approach flap setting. The horizontal stabilizer actuator was recovered and its dimensions were consistent with a stabilizer position of between 2° to 3° stabilizer up (nose down). All three landing gears were in the retracted position. The burnt remains of one of the aircraft's two radio magnetic indicators were recovered with two needles attached. The needles were pointing to approximately the 5 o'clock position, consistent with the approximate position of the Sandy Bay NDB in relation to the accident site and the aircraft orientation. The needle position is also consistent with aircraft electrical power being applied at the time of impact.
1.13 Medical and Pathological Information
1.13.1 The Captain
The captain held a Category 1 medical certificate issued by TC on 15 October 2004. The certificate showed that the captain had been declared medically fit by a civil aviation medical examiner on 25 August 2006, renewing the privileges of the captain's licence.
The TC Medical Division conducted a review of the captain's aviation medical records and determined that the captain had no medical conditions of relevance to the occurrence.
Autopsy results indicate that the captain received life-threatening injuries during the crash. The autopsy and toxicology tests did not reveal any pre-existing condition or substance that could have affected the captain's performance.
1.13.2 The First Officer
The first officer held a Category 1 medical certificate issued by TC on 06 December 2001. The certificate showed that the first officer had been declared medically fit by a civil aviation medical examiner on 17 March 2006.
The TC Medical Division conducted a review of the first officer's aviation medical records and determined that the first officer had no medical conditions of relevance to the occurrence.
1.14 Fire
The aircraft fuel tanks, located in rubber bladders in the wings, were torn open during the impact with the trees. A post-impact fire consumed approximately 80 per cent of the aircraft, leaving only the rear fuselage and empennage unburned.
1.15 Survival Aspects
The collision with the ground was survivable to most of the aircraft occupants because the aircraft decelerated gradually, with the flexing and shredding trees absorbing impact forces as the aircraft travelled through them. The fuselage did not strike any large trees, although both wings outboard of the engine nacelles were torn off by trees. The aircraft remained upright with the nose of the aircraft crumpling rearwards as it came to a stop.
All the occupants were conscious after the impact and were able to unfasten their restraint harnesses and seat belts. Fallen trees overlaid the fuselage and blocked the cabin entrance door on the left side of the aircraft. The first officer and one EMT pushed the door partially open with their feet, and the occupants evacuated the aircraft with difficulty, with only the clothing they had been wearing. The survival and first-aid kits on board were either inaccessible or could not pass through the limited opening of the door.
The forest at the crash site consisted of dense poplar and evergreen trees with heavy undergrowth and knee-to-hip-deep loose snow. The captain and one EMT were pulled away from the vicinity of the burning wreckage by the first officer and the other EMT. The first officer and the least seriously injured EMT left the crash site to go for help. They made their way through the forest and down the hillside to the frozen river surface before they realized that they would not be able to reach the aerodrome through the snow in the extreme darkness and cold temperature. They returned to the crash site, ending up on the opposite side of the burning wreckage from the captain and other EMT.
Sandy Bay Health Centre staff heard the aircraft fly overhead at about 2000. At about 2015, a staff member drove to the aerodrome to meet the aircraft. The aircraft was not on the apron and the aerodrome lighting was off. The staff member waited at the aerodrome for the flight until returning to the Health Centre at about 2045 and advising the head nurse, TWA, and the ambulance dispatch centre that the flight had not arrived.
A search party of Health Centre staff and police officers drove to the aerodrome and observed flames at the crash site from the departure end of Runway 05. The crash site was not accessible by foot or by road, and the search party returned to town for snowmobiles and additional help. The first rescuers arrived at the crash site at about 2200. Medical staff determined that the captain was deceased. The first officer and both EMTs were transported to the Sandy Bay Health Centre and subsequently flown to La Ronge and Saskatoon, Saskatchewan, by other medevac aircraft.
Search-and-rescue satellite systems did not detect any signals from the aircraft emergency locator transmitter (ELT). The absence of a usable ELT signal did not delay the search and rescue because local authorities initiated a search immediately after it was confirmed that the flight had not arrived.
1.16 Tests and Research
The ELT was recovered from its mounting bracket in the empennage area; it was partially charred and melted by the fire. The ELT was found in the armed position when recovered. An examination of the ELT found that the internal inertia switch had been tripped, indicating that the ELT had been activated. The ELT antenna mounted on the upper surface of the aft empennage was damaged and covered by fallen trees and foliage, which would have weakened the ELT signal, rendering it ineffective.
1.17 Organizational and Management Information
1.17.1 Transwest Air
1.17.1.1 General
TWA is a large regional airline operating from its main base in Prince Albert with sub-bases throughout Saskatchewan and Manitoba. The company operates a fleet of 14 aircraft types of both fixed-wing and rotary-wing aircraft under subparts 702, 703, 704, and 705 of the Canadian Aviation Regulations (CARs). At the time of the occurrence, the company operated 4 rotary-wing and 39 fixed-wing aircraft, including two Beech A100 King Air aircraft. The company had 232 employees, including 65 pilots and 12 flight attendants. During the summer float flying season, company size increases to about 280 employees.
The company was formed from the merger of Athabaska Airways and La Ronge Aviation in 2001. Following the merger, the company operated under subparts 702, 703, and 704 of the CARs. In June 2002, the company expanded into CARs subpart 705 airline operations with two SF340 turboprop aircraft. In 2005, TWA acquired some of the aircraft and pilots from another company, which had ceased operations.
The company is headed by two managing partners, with directors of functional areas reporting to the managing partners. The Director of Flight Operations (DFO) manages the Flight Operations Department and is designated as the operations manager for the purposes of the company's air operator certificate (AOC). Chief pilots, the flight attendant manager, the safety manager, and duty officers report to the DFO. Training pilots and line pilots report to the chief pilots.
1.17.1.2 Air Operator Certificate and Operations Specification 99
TWA holds an AOC issued by TC authorizing the types of services listed in the certificate, provided the company complies with the conditions and operations specifications of the AOC. Some of the conditions of the AOC are, in part: to conduct flight operations in accordance with the company operations manual, to employ managerial personnel who meet the Commercial Air Service Standards (CASS), and to conduct a safe operation.
The AOC includes OPS SPEC (Operations Specification) 99 authorizing the use, by a number of aircraft types including the Beech A100 King Air, of restricted instrument procedures (RIPs) published in the RCAP. The use of RIPs is subject to the following conditions: the pilot-in-command (PIC) shall ascertain by means of radio communication or by visual inspection the condition of the intended landing surface and the wind direction and speed; and the air operator shall not authorize its flight crews to use, nor shall any flight crew member conduct, a RIP published in the RCAP unless all the provisions attached to that RIP are complied with.
1.17.1.3 Flight Operations Manual
The TWA FOM has been compiled for the use and guidance of TWA operations personnel. All flight and ground operations personnel are required to follow FOM policies and procedures in the performance of their duties. The FOM specified the company management structure and the duties and responsibilities of all management team members.
The DFO is responsible for safe flight operations. Some specific responsibilities of the DFO listed in the FOM are: control of operations and operational standards of all aircraft operated; supervision, organization, staffing, and efficiency of flight operations; crew scheduling, training programs, and the safety management system (SMS); ensuring that operations are conducted in accordance with current regulations, standards, and company policy; and qualifications of flight crews.
The safety manager is responsible for providing guidance and direction for the operation of the company's SMS. Some specific responsibilities of the safety manager were to implement the company's SMS, and to identify hazards and carry out risk management analyses of those hazards.
The duties and responsibilities of the PIC are covered in depth in the FOM over 1½ pages, including:
- preparing and operating the flight safely and in compliance with the requirements of the CARs and all company directives, policies, bulletins, and notices;
- being solely responsible for aircraft dispatch and flight watch;
- flight planning and coordination of all pre-flight activities;
- completing and filing with the base duty officer pre-flight documentation as required;
- being knowledgeable and proficient in: SOPs, the use of aircraft performance charts and tables, normal, abnormal, and emergency procedures, and instrument flight procedures; and
- operating the aircraft in accordance with the appropriate company SOPs at all times.
The FOM describes the duties and responsibilities of the second-in-command (SIC) as follows: "The second-in-command is responsible to the pilot-in-command and shall carry out any assigned duties as specified by the PIC and outlined in the standard operating procedures for the aircraft, as applicable."
As required by CASS 723.105, the FOM included forms and instructions for use for operational flight plans, passenger manifests, and weight and balance.
One section of the FOM echoed the conditions in OPS SPEC 99, stating the following:
In all cases, instrument approach procedures shall not terminate in a landing unless, prior to landing, the PIC has determined by means of a radio communication or visual inspection:
- the condition of the intended landing surface; and
- the wind direction and speed.
1.17.1.4 Pilot Self-Dispatch
Although the DFO retains responsibility for the day-to-day conduct of flight operations, operational control of all TWA flights is delegated to the PIC. This system of operational control is known as pilot self-dispatch and delegates all responsibility for aircraft dispatch decision making to the PIC. Crews reported that company management accepted no-fly decisions and did not exert pressure on pilots to reverse their decisions.
The FOM specified a requirement for all flights to be authorized by the DFO or chief pilot, but did not specify any process for authorization. In La Ronge, the authorization was delegated through the base manager to the duty officer, whose only role in dispatching a flight was to confirm to the customer that an aircraft and crew were available, and then to alert the crew and maintenance of the flight being dispatched. All other decisions regarding dispatch were made by the PIC. The FOM did not include, and was not required to include, any pilot self-dispatch decision support tools such as pre-flight planning checklists, Footnote 6 or aerodrome hazard summaries.
Pilot self-dispatch systems are widely used by commercial air operators across Canada.
1.17.1.5 Pairing Policy
Section 705.108 of the CARs requires airline operations to have a crew pairing policy. This regulation does not apply to air taxi and commuter operations. The FOM included a pairing policy that applied to the company's airline operations, but not to commuter or air taxi operations. The policy set restrictions on crew pairing based on hours of experience and formal qualifications. The policy required, in part, "when, after completion of their individual line indoctrination, crew pairing restrictions apply to both the PIC and to the SIC, a training pilot shall occupy the jump seat."
Had it been applicable to air taxi operations, the pairing policy would not have prevented the first officer from being paired with the captain and would not have imposed any restrictions on the crew.
1.17.1.6 Unscheduled Service to Registered Aerodromes
Although TWA did not operate scheduled service to Sandy Bay and other registered aerodromes, unscheduled service occurred frequently. The two King Air aircraft that the company operated flew into Sandy Bay 12 times from 20 December 2006 to 07 January 2007, including the accident flight and one subsequent medevac flight.
TWA did not identify specific risks associated with frequent unscheduled flights to registered aerodromes, and was not required to do so by regulation.
1.17.1.7 Global Positioning System Approaches
TWA was working toward implementation of GPS approach capability within its fleet and had submitted a GPS pilot training program to TC for approval. The training program would require that pilots be provided knowledge regarding human factors applicable to the use of GPS and how errors might be reduced or eliminated.
TWA King Air pilots, including the captain and the first officer, were not yet trained or certified to conduct GPS approaches. They reported flying instrument approaches using traditional NDB and VOR (very high frequency omni-directional radio range) approach aids for primary track guidance, and also routinely using the GPS to provide distance to the aerodrome. They retrieved aerodrome information from the GPS database by entering the aerodrome identifier and selecting it as the active waypoint.
1.17.1.8 Flight Crew Training Manual
Although the company FCTM was issued as a separate manual, it formed part of the FOM and was approved by TC. The FCTM stated in part that the flight crew training programs were "designed to ensure that each person who receives training acquires and maintains the competence to perform assigned duties."
Line indoctrination was intended to assess a new captain's proficiency and decision making, and to ensure thorough familiarity with the company's bases, routes, and operations. CARs do not require line indoctrination for air taxi operations, and, although one section of the FCTM indicated that line indoctrination was required only for commuter and airline operations, another section of the FCTM also required a minimum of 20 hours of line indoctrination for multi-engine air taxi captains. The company's practice was to assess each pilot individually and, for pilots with little experience as PIC or who had been away from flying for lengthy periods, to increase the amount of line indoctrination to about 100 hours.
The FCTM required all CAR 705 airline flight crew members to complete initial and annual recurrent training in CRM. No CRM training was required for CAR 703 air taxi or CAR 704 commuter flight crew members.
Pilot line checks are a means of verifying crew compliance with standards, policies, and procedures. The FCTM included a line check form to record line and route checks. The description in the form indicated that it was to be filled out by the check pilot on completion of the flight, and the flight reviewed with the candidate to ensure full understanding of any debriefing items and rectification. The form was to be forwarded to the chief pilot for review and retention.
Line checks were not described anywhere else in the FOM or FCTM, and no guidance was provided for the frequency at which line checks were to be conducted or the criteria governing when they would be conducted. Line checks were rarely done at TWA.
Although the company emphasized the need for stable approaches during initial qualification training, neither the FCTM nor the SOPs included any flight crew guidance as to when an approach should be considered unstable or criteria under which an approach must be abandoned.
1.17.1.9 Director of Flight Operations/Safety Manager
On 10 August 2005, TWA notified its principal operations inspector (POI) at TC's Prairie and Northern Region (PNR) that the DFO would be on sick leave for 90 days and the company was instructed to nominate a replacement. TC's PNR subsequently issued an AOC notice of suspension to TWA to come into effect on 10 September 2005 providing a 30-day period to replace the DFO. The DFO returned to work on 09 September 2005 and the notice of suspension was rescinded.
The DFO was absent on sick leave again in May 2006 and, on 14 November 2006, went on extended sick leave. The company nominated the safety manager to replace the DFO.
The safety manager had worked closely with the previous DFO since being appointed in October 2005 and had been employed as acting DFO during periods when the previous DFO was absent on sick leave. On 08 December 2006, TC approved the safety manager as the new DFO. The company began the process of replacing the safety manager, and the new DFO retained the duties of the safety manager. The new DFO was still employed as the safety manager at the time of the accident.
The new DFO had 13 years of aviation experience as a flight instructor and commercial pilot, had completed the TC company aviation safety officer (CASO) course, and had supervisory experience as a chief flying instructor. The new DFO held an ATPL, was employed as a CAR 705 airline captain on the SF340, and was based in Saskatoon. The new DFO's flying workload decreased substantially from October 2005 to the time of the occurrence—flying about five days per month and averaging about 25 hours of flight time per month during the 12 months before the occurrence.
1.17.1.10 Southern Chief Pilot
The chief pilot's responsibilities grew as the company expanded and he became responsible for supervising 65 pilots dispersed at a number of bases and sub-bases throughout the company's area of operations. In April 2003, one of the company's training pilots proposed to the DFO that the chief pilot's job be split, with a chief pilot based in Saskatoon for the company's commuter and airline operations and a second chief pilot based in La Ronge for aerial work and air taxi operations. The training pilot indicated that he felt that the company's operations warranted two full-time chief pilots and offered himself as a candidate for the La Ronge-based job. The company did not take any immediate action on this proposal.
TC had expressed concern about the chief pilot's workload, so the company began work during 2005 and 2006 to put in place a second chief pilot, with the first chief pilot renamed the southern chief pilot (SCP). The SCP's flying workload was variable, with about 3 to 12 days per month spent flying, averaging about 20 hours of flight time per month during the 12 months before the occurrence. The SCP was based in Saskatoon and was employed as a CAR 705 airline captain on the SF340.
1.17.1.11 Northern Chief Pilot
The northern chief pilot (NCP) began employment with TWA in April 2006 and was based in Saskatoon. He held an ATPL and had over 20 years of experience in commercial aviation flight operations. The NCP had completed commercial business management courses and had experience as an air taxi operations manager supervising 10 pilots, and as a training pilot and senior base pilot supervising 4 pilots for a large Canadian Twin Otter aircraft operator.
The NCP received initial and line indoctrination training to qualify as a captain on the company's SF340 airline aircraft. He was also qualified on de Havilland DHC6 commuter aircraft and flew as captain on both aircraft during the summer of 2006, as well as working with the SCP doing managerial tasks. The NCP's flying workload was high during June and July 2006 during his initial qualification on the SF340, with 27 days flying and 135 hours of flight time. On average, the NCP flew about 7 days per month, averaging about 35 hours of flight time per month during the time he worked for TWA.
On 19 September 2006, TC approved the nomination of the NCP to be a chief pilot under subparts 702, 703, and 704 of the CARs. The SCP retained responsibility for supervising the company's 23 subpart 705 airline pilots. The NCP was responsible for the supervision of 42 air taxi and commuter pilots from Prince Albert and northward, including training pilots and the crews operating the company's two King Air aircraft from La Ronge.
The FOM describes the duties and responsibilities of the chief pilots. The NCP is responsible for the professional standards of the flight crews under his authority, including: developing SOPs; developing and implementing required flight crew training programs; operational suitability and requirements of all aerodromes served by the company; acting on and distribution of accident, incident, and other occurrence reports; supervision of flight crews; and processing and acting on any flight crew reports.
The NCP's approach to supervision was informal. He did not keep records of interactions with his subordinates and did not have a formal plan to monitor pilot performance. The NCP met or talked frequently with the training pilots. Before December 2006, the NCP's schedule was not published, but beginning in December 2006, his schedule was widely distributed to pilots and management. This approach allowed the NCP to meet the pilots he supervised while he was line flying, during stopovers at company bases at La Ronge, Stony Rapids, and Wollaston, or while pilots were at the Saskatoon base.
The NCP made base visits to one or more of these locations about once per month for several days and had an office established at the company's water base in La Ronge. He was also available to pilots by telephone or e-mail. Periodic pilot meetings would be held to discuss issues of operational or general interest.
Most of the pilots interviewed felt comfortable addressing any concern regarding proficiency of other pilots with the NCP, and several had done so. All the pilots interviewed were aware of the supervisory role of the NCP, and all but one pilot knew that the NCP was their immediate supervisor.
1.17.1.12 Pilot Hiring
The company had an established hiring process, requiring the use of a questionnaire checklist to be completed by the flight operations clerk during a telephone screening interview, and a more detailed interview checklist to be used by a manager during either a telephone or face-to-face interview. The hiring manager varied depending on availability and was one of the following: a managing partner, the DFO, the Director of Passenger and Ramp Services, the SCP, or the NCP.
Pilots with current qualifications and experience on King Air aircraft were in demand across Canada. During the 12-month period before the occurrence, TWA lost three King Air captains and one first officer to other companies.
Because of the competitive environment, the company hired pilots meeting its criteria for immediate employment as King Air captains. The captain's resume indicated that he met the company's Beech A100 King Air captain criteria and included information about previous employers, but did not include any information about employment from November 2003 to April 2006. The safety manager and SCP were on vacation while the company was hiring the captain; the NCP contacted the captain by telephone to obtain further information and passed the resume to the previous DFO.
Other than the resume, the company did not have any documents regarding pre-employment screening or interviews of the captain, and nobody at the company could recall doing such screening or interviews. The company did not have any documents regarding reference checks. No TWA personnel could recall calling a previous employer of the captain and none of the previous employers received any calls from TWA about the captain. The company also had no records documenting the hiring of the first officer.
In addition to the first officer of TW350, five other junior pilots employed by TWA were interviewed during this investigation. Two of the five had also completed aviation college training programs, and the other three had done their training at commercial flight schools with college affiliations. All five began their employment with TWA by doing a period of service of about one year in non-flying jobs, including hotel clerk, duty officer, fuel truck operator, and dock/ramp agent. Three of the five had begun their TWA flying as first officers on Beech turboprop aircraft. One had begun flying as a first officer on twin-piston aircraft and one was still doing ground duties and waiting for an initial flying position.
1.17.1.13 Company Response to Repeated Flight Crew Regulatory Infractions
In the fall of 2006, an experienced aviation consultant was hired to conduct an independent audit of TWA's operations. The consultant found, in part, that the company's management response to repeated flight crew regulatory infractions was insufficient and recommended that the company implement a disciplinary policy.
The disciplinary policy implemented by the company used unpaid suspension from duty as punishment. The first application of the policy, on 27 November 2006, was to the captain and first officer of TW350 following investigation of an incident at Fort McMurray, Alberta, on 24 November 2006 (see section 1.17.1.15 for further details on the investigation and suspension).
The disciplinary policy was subsequently revised to fines of 10 per cent of monthly salary for a first offence and 20 per cent of monthly salary for a second offence, with no suspension from duty. In addition to the disciplinary policy, pilot meetings concerning repeated flight crew regulatory infractions were planned for December 2006 but, because of scheduling difficulties, were held after the accident in January 2007.
Between 27 November 2006 and 08 February 2007, two other TWA crews were involved in CARs infractions, with all four pilots being fined by the company under the revised disciplinary policy. All the King Air pilots interviewed were aware of the disciplinary policy and clearly understood it.
1.17.1.14 Safety Management System Implementation
Although TWA was required to implement a SMS because it operated under CAR 705, the company had chosen to have the SMS apply to all of its operations (see Appendix C for more information on the SMS). One of the managing partners was the accountable executive, the DFO was responsible for supervision, organization, and staffing, and the safety manager was responsible for development, implementation, and operation of the SMS under the authority of the DFO. Implementation was occurring in four phases, with each phase having specific requirements. TWA was in phase 2 of SMS implementation at the time of the occurrence.
During phase 1 of SMS implementation, the company had completed a gap analysis, a SMS implementation project plan, and the submission of its SMS documentation to TC. Phase 2 entailed implementation of the company's safety management plan and safety oversight components: reactive processes, investigation and analysis, and risk management. Phase 2 also required the following: training for personnel involved in the SMS, documentation of relevant policies and procedures, a TC review of the company's documentation, and a TC on-site SMS assessment that was scheduled for 23 April 2007.
Phase 3 involved implementation of processes for the proactive identification of hazards. It was scheduled to be complete by 30 September 2007. Phase 4 involved implementing operational quality assurance and emergency preparedness and response, and documentation of relevant policies and procedures. Phase 4 was scheduled to be complete by 30 September 2008.
1.17.1.15 Supervision of TW350 Crew
The TSB investigation examined three events within TWA involving supervision of the occurrence captain and first officer by company flight operations managers during the months before the accident.
The first event occurred in the fall of 2006, when the captain discussed the first officer's performance with the NCP and a training pilot. The captain assessed the first officer's landings as being inconsistent and sometimes unsatisfactory, and asked for guidance on how to help improve the first officer's landings. The NCP perceived the captain's concerns as a senior pilot wanting to help a junior pilot improve proficiency, and not as expressions of a hazardous situation. The NCP determined that other captains occasionally coached the first officer, but did not share the captain's assessment of the first officer's landings as being unsatisfactory. A training pilot was directed to assess the first officer's landings during a training flight and determined that the first officer had some initial difficulty landing with a crosswind, but improved during the flight and demonstrated satisfactory landings. The NCP verbally counselled the captain to be more assertive and provided tips on how to work together with the first officer to improve landing techniques, including demonstrating landing techniques and coaching the first officer if necessary. The NCP investigated this report by himself and no records were made to document the investigation.
The second event occurred on 13 November 2006, when the captain and first officer were paired for an IFR flight to Meadow Lake. The captain was the PF and the first officer was the PNF. After the flight, the first officer advised the NCP of problems during the arrival at Meadow Lake. The NCP requested a written report and, on 17 November 2006, the first officer reported the following:
- the captain's disagreement with the first officer's advisories regarding the inbound approach track;
- the captain banking excessively during the procedure turn;
- the captain descending further below MDA after the first officer called descent below MDA;
- the captain again descending below MDA during the second approach;
- when the captain acquired visual reference to the surface, the aircraft was not positioned to land on Runway 09 and the captain indicated that he would circle the airport and land on Runway 09;
- during the circling, the captain decided to land on Runway 35 rather than Runway 09; and
- on landing, the aircraft touched down on Runway 35 before the flaps had fully extended.
This report was made directly to the NCP, who investigated this report by himself without using the company's SMS investigative processes.
The NCP subsequently interviewed the first officer and the captain. The NCP reviewed the report of the poorly flown approach and poor crew coordination with the captain, and was satisfied that the captain understood the deficiencies identified. The NCP concluded that it was not necessary to conduct a training flight to review SOPs or instrument procedures, or to assess the captain's flying proficiency and decision making with a line check. No training flights or line checks were conducted or required, and the captain continued line flying.
The NCP verbally counselled the first officer to be more assertive in the cockpit by identifying incorrect procedures or inaccurate flying. Other than the first officer's report to the NCP, no records were made of the information the investigation gathered or the decisions made.
The third event occurred on 24 November 2006. The occurrence captain and first officer had been paired as a crew for a scheduled flight from Saskatoon to Fort McMurray. Although the crew was required to initiate communication on the mandatory frequency (MF) five minutes before commencing the approach procedure and TWA aircraft were equipped with more than one radio to permit communication on more than one frequency, the crew members made their first transmission on the MF when they were two miles from landing at Fort McMurray. The crew was advised by the Fort McMurray flight service specialist that they had not made the required transmission, but the crew did not report the incident to their company.
TWA was using the TC Civil Aviation Daily Occurrence Reporting System (CADORS) as one of its SMS data sources for reactive incident investigation, and the TWA safety manager initiated an investigation immediately after learning of the event through a review of CADORS information. This event was investigated jointly under the company's SMS by the safety manager and the SCP and NCP.
The company's investigation made a finding as to cause of "lack of situational awareness" and determined that, although the crew members understood the regulatory requirement to communicate on the MF before commencing the approach, they were unsure when they were required to use a second radio if the first radio was in use with ATC. The safety manager recommended that the crew review MF procedures and the NCP added a recommendation for the crew to review IFR airport procedures.
As part of the SMS documentation of the incident, the safety manager completed a company audit finding form, identifying the incident as a non-conformance with subsection 602.104(2) of the CARs. The short-term corrective action plan specified that the NCP had immediately removed the crew from line flying until further notice. The long-term corrective action plan included two items: first, a safety directive (SD06-15) sent out to all flight crews regarding the numerous unnecessary CARs violations that TWA had incurred over the past year; second, pilot meetings were to be held at each base to discuss CARs violations. The finding form included follow-up action for a line check to be performed on the crew by the training pilot to ensure that regulations and SOPs are being followed, but did not propose a date for the line check. The finding completion was dated 27 November 2006.
TWA's SD06-15 regarding CARs violations was issued by both chief pilots to all pilots on 22 November 2006 (see section 1.17.1.17 for further information about SD06-15).
On 27 November 2006, the NCP advised the captain and first officer by telephone that they were suspended from flight duties and followed up with a suspension letter to each pilot. Although the captain acknowledged understanding the requirement to communicate on the MF before commencing the approach, he had insisted that ATC was responsible for the incident rather than the crew. Because he did not accept full responsibility for the incident, the captain was suspended for 15 days (26 November to 10 December 2006). The first officer did accept responsibility for the incident and was suspended for seven days (26 November to 02 December 2006).
The captain and first officer were scheduled to fly together only once in December 2006; consequently, the company planned to conduct a line check in January 2007. No line check was scheduled or conducted on the crew before they returned to flying duties following the suspensions.
1.17.1.16 TW350 Crew Pairing and Scheduling
Since the approval of his nomination, the NCP had met with all the company's King Air pilots. None of the other pilots had discussed with the NCP any concern regarding either the captain's or the first officer's flying proficiency. However, one pilot had advised the NCP verbally of his concern about pairing the captain and first officer, and also verbally advised the La Ronge base manager not to pair the captain and the first officer.
The NCP did not consider the Meadow Lake and Fort McMurray incidents as indications of any problem with the captain and first officer as a crew pair, and he did not have any concerns about the pairing of the captain and the first officer.
By mid-December 2006, the captain and first officer had returned to flying following their suspension. On 24 December 2006, the NCP distributed the January 2007 King Air flight crew schedule, pairing the captain and the first officer for the entire month.
1.17.1.17 Operations Directives and Safety Directives
The company disseminated information to pilots using operations directives (ODs) and safety directives (SDs), with sign-off sheets used by pilots to indicate that they had read the information. Some of the directives issued by the company in 2006 are described below.
On 12 June 2006, the safety manager issued SD06-04 to all crew members regarding the importance of incident reports. The directive discussed implementation of the company's SMS, including the incident/accident reporting system, provided guidance on when a report was needed, and encouraged crew members to submit reports in a timely manner.
On 30 August 2006, the safety manager issued SD06-11 to all flight crews regarding MF advisory calls. The directive indicated that the company had been advised by TC of several incidents where crews had not complied with MF communications requirements. The directive included quotes from applicable CARs regarding MF reporting procedures for both arrivals and departures. Both the captain and first officer of TW350 acknowledged reading this directive by initialling the sign-off sheets.
On 30 October 2006, the safety manager issued SD06-13 regarding the black hole effect. The directive reminded pilots that "black hole conditions occur when there are no surface lights between the aircraft and runway environment and the sky is overcast and/or moonless." The directive identified two hazards associated with black holes: false climb illusion after take-off, and a tendency for pilots to fly too low on approach and collide with terrain short of the runway. The directive included the following guidance to reduce the risk of these hazards: using distance measuring equipment (DME) to assist in maintaining a descent based on 300 feet per nm and considering over-flight of an unfamiliar airport before beginning the approach descent. The directive did not identify any specific runways affected by black hole conditions. All the King Air pilots had initialled the sign-off sheet for this safety directive, including the captain and first officer. All the pilots interviewed were aware of black hole hazards, although not all recalled reading the safety directive.
On 22 November 2006, the NCP and SCP issued SD06-15 regarding CARs violations. The directive indicated that company flights had been involved in several CARs violations during the past year, including altitude violations, airspace infractions, and MF violations. The directive indicated that TWA pilots held commercial or air transport pilot licences that certified an understanding of aviation regulations, and emphasized the need to comply with regulations to ensure the safety of passengers and crew members. The directive stated the company's responsibility "to ensure that all crew members are conducting themselves in a safe and knowledgeable fashion" and pointed out that, once a flight departs, the crew has "sole responsibility for the continuance of this professionalism." The directive indicated that the chief pilots and the safety manager were available to answer questions or to provide clarification regarding regulations.
1.17.1.18 Beech A100 King Air Standard Operating Procedures
The King Air SOPs were issued by TWA for guidance on the operation of the aircraft.
Section 3.3 of the SOPs required the first officer to complete all required performance calculations prior to flight and the captain to review the calculations. Also, section 3.18 of the SOPs required crews to always consult landing charts for contaminated runway operations.
Aircraft performance charts are contained in the AFM. This manual is kept on the aircraft for pilot reference. The company did not provide any means of easily recording or displaying aircraft performance calculations in the cockpit, nor were they required to.
The crew of TW350 did not make or review any pre-flight aircraft performance calculations. Additionally, none of the TWA King Air pilots interviewed made reference to aircraft landing performance charts during line operations, and only one pilot could provide an estimated landing distance, 1500 feet, when asked to do so by investigators. Although all had received training in the use of aircraft performance charts during initial or recurrent training, pilot expectations of aircraft performance on landing were based on experience gained during line operations.
The SOPs required that a copy of the OFP, weight and balance, and passenger manifest be left at the point of departure. The crew of TW350 did not leave behind copies of the OFP, weight and balance, and passenger manifest.
The SOPs required that a pre-flight crew briefing be conducted and that specified items be briefed, and also required the crew to conduct a pre-flight passenger briefing. The crew of TW350 did not conduct either of these briefings.
Section 5.7.3 of the SOPs permitted pilot role switching and indicated that take-offs, landings, and en route flying are normally shared on a 50/50 basis. This SOP also stated "the Captain may assume any flying task at his discretion."
The company had a widely known and unwritten policy requiring the captain to fly the first leg of the day. The intent of this unwritten policy was to ensure that the most experienced crew member would be PF in the event of aircraft mechanical problems that were thought to be more likely to occur on the first flight of the day. The practice of the crew of TW350 was that sometimes the captain would fly the first leg and sometimes the first officer would fly the first leg. Pilots interviewed were all aware that there was an unwritten company policy; however, some pilots thought that the practice was part of the SOPs, while some other pilots thought that the captain could decide who would fly the first leg. Pilots reported occasions when a first officer would fly the first leg. Pilot practice was to alternate legs when possible in order to provide both pilots with equal flight time at the controls.
TWA had a standard aircraft control transfer procedure used throughout its multi-crew fleet, including the King Air. Section 3.13 of the SOPs defined the procedure for transfer of aircraft control from one pilot to the other, stating "anytime that control of the aircraft is transferred from one pilot to the other, the following phraseology shall be used:"
PF ....................................................................... "You have control"
The PF shall not release controls until he hears:Pilot assuming control ............................................ "I have control"
Or, if the PNF is initiating the control transfer:Pilot assuming control ............................................ "I have control"
Pilot relinquishing control ....................................... "You have control"
Section 5.9 of the SOPs defined standard callouts for transfer of control from one pilot to the other, whereby the pilot assuming control would say "I have control" and the pilot relinquishing control would respond "you have control."
The investigation examined three instances of control transfer during the flight of TW350. In the first, at 1945:53, the first officer used the standard phrase and the captain used a non-standard phrase to indicate that he had control. In the second, at 1947:08, both crew members used the standard phrases required by the SOPs. In the third instance, during the go-around, neither crew member made any verbal statement regarding the transfer of control. The third instance is discussed in section 2.10.
TWA King Air pilots reported that the transfer of control procedure was well understood with mostly consistent compliance. Only one pilot reported any deviations from this procedure and, other than the first officer, no pilot had experienced the captain taking control without following the transfer of control procedure and verbally stating his intentions.
Section 6.10 of the SOPs required the PNF to check the engine instruments and verbally indicate that they had been checked during the cruise check. The captain did not verbalize checking the engine instruments and did not call the cruise check complete.
During the descent and approach check, the crew was required to conduct a passenger briefing, but did not do so.
Section 3.22 of the SOPs provided crew guidance for approaches and specified "straight-in approaches must not be done unless VASIS, PAPI, or glide slope information is available and used." The SOP did not identify specific locations where this policy would apply. Half the pilots interviewed were not aware of this prohibition of straight-in approaches, and even those pilots aware of it reported occasionally flying straight-in approaches under such conditions.
Section 3.25 of the SOPs stated that "the captain shall normally carry out all landings on runways under 3500 feet and any landings as conditions warrant (for example, low Canadian Runway Friction Index [CRFI], crosswinds, emergencies, etc.)." Although most of the pilots interviewed were aware of this requirement, some were unaware of any first officer landing limitations and thought that the captain could decide when a first officer could land. Some pilots did not know in which manual this directive was. One captain disagreed with the directive because he felt that the policy reduced opportunity for first officers to gain experience and improve their skills. Another captain was adamant about never permitting a first officer to land at Sandy Bay, and approached low over the threshold at Sandy Bay to touch down as close to the threshold as possible. Another first officer, other than the occurrence first officer, reported that the occurrence captain had permitted him to land at Sandy Bay.
The SOPs required the approach briefing to include specified elements, including the inbound track, airport elevation, and approach speed, and also recommended that corrections for below standard temperatures be made to procedure altitudes. The first officer's approach briefing for the straight-in NDB approach to Runway 05 did not include these elements.
Section 2.7.4 of the SOPs required that all flight crew members were to monitor other crew members in the performance of their duties. Any deviation or omission by a person was to be challenged by bringing it to the attention of that person as soon as practicable. However, during the occurrence flight, neither crew member challenged the other regarding deviations from the SOPs. Two examples of this are the captain's decision for the first officer to be PF, which was not challenged by the first officer, and the first officer's decision to conduct the approach straight-in, which was not challenged by the captain.
Section 2.6 of the SOPs required the PNF to call checklists complete. The captain was the PNF throughout the flight and did not call the completion of any checklists.
Section 4.2.4 of the SOPs provided a text description (below) of the missed approach or go-around procedure (two engines). This description was located in the emergency procedures section of the SOPs, rather than in the normal flight procedures section, and stated: "Two engine approaches will be conducted with Flaps Approach. The PF shall initiate the power for a go-around. For a missed approach over a runway the same procedure applies."
| PF | PNF |
|---|---|
| 1. Calls "GO AROUND, MAX POWER, FLAPS APPROACH" and simultaneously applies max. torque, raises nose to 10 to 15° up. | |
| 2. Ensures max. power is set and selects flaps to approach. Calls "MAX POWER SET, FLAPS APPROACH" | |
| 3. Calls "POSITIVE RATE" | |
| 4. Retracts and Calls "GEAR UP" | 5. Calls "400 feet" |
| 6. Calls "ACCELERATING" and accelerates to V2 +10 or greater | 7. Calls "V2 + 10" |
| 8. Calls "FLAPS UP" | |
| 9. Selects and Calls "FLAPS UP" and calls the missed approach procedure and monitors PF | |
| 10. Calls "1500 FEET" | |
| 11. Calls "CLIMB POWER AND AFTER TAKE-OFF CHECKLIST". | |
| 12. Advises ATC of intentions and requests appropriate clearance. Completes checklist. |
Section 5.9 of the SOPs specified standard callouts and required the PNF to call "go-around" to initiate a missed approach or go-around. The captain did not use the phrase "go-around" to communicate his decision to abandon the landing attempt and conduct a go-around. The phrase used by the captain was non-standard and did not clearly state his intent.
Sections 7.4 and 7.7 of the SOPs provided flight profile diagrams for precision and non-precision instrument approaches that included text descriptions of the go-around as follows:
- Go-Around
- Max Power
- Flaps Up
- Gear Up
- Climb 150K
Pilots interviewed had varying descriptions of the go-around procedure; some pilots described the initial flap selection as flaps to approach, and some as flaps up.
The new DFO and the NCP knew of the captain's concerns regarding the first officer's landings, as well as the Meadow Lake and Fort McMurray incidents. However, neither manager was aware of the extent of the deviations from company policies and procedures within the King Air operation that are listed in this section. Both managers considered compliance with policies and procedures to be satisfactory.
1.17.1.19 Medevac Operations
The purpose of the flight was to transport a patient who had a non-life-threatening condition to Flin Flon. The crew's decision making was not influenced by any perceived pressure to complete the medevac mission.
1.17.2 Transport Canada
Transport Canada Civil Aviation (TCCA) is organized into headquarters and regional functions. Headquarters provides strategic policy guidance and support to the regions, and retains some operational oversight of large aviation companies. TCCA is headed by the Director General, Civil Aviation (DGCA) in Ottawa, Ontario. Prairie and Northern Region (PNR) is headed by the Regional Director, Civil Aviation (RDCA), who reports to the PNR Director General rather than the DGCA. Various mechanisms have been developed to coordinate the national management of TCCA. Footnote 7
TCCA's Commercial and Business Aviation (CBA) Division in each region was responsible for the oversight of commercial air operations that fall under Part VII, Commercial Air Services, of the CARs. Footnote 8 The CBA Division handles applications for new operations and changes to existing operations, and monitors day-to-day operations to ensure that air operators meet the required standards in the CASS and conduct business in accordance with their AOC. At the time of the accident, oversight was conducted through formal audits, inspections, PPCs, ramp inspections, and in-flight inspections. Each air operator has an assigned POI that monitors the company's operations. The activities of the POI are governed by TC's publication Air Carrier Inspector Manual (ACIM) (TP 3783).
The POI for TWA was responsible for 17 companies; TWA was the largest of these. The POI's contact with TWA was through the DFO and much of it related to amendments to the company's operating manuals and implementation of the company's SMS. Most of the contact was by telephone and correspondence, with occasional meetings. Because the POI was not qualified on the SF340 aircraft operated by TWA, PNR designated a second inspector as the SF340 POI.
1.17.2.1 Strategic Planning
In its strategic plans published in December 1999 Footnote 9 and April 2006, Footnote 10 TCCA articulated its commitment to consistent risk management in decision making and to the implementation of SMSs within aviation organizations (see Appendix C for more information on these strategic planning documents).
1.17.2.2 Risk Management and Decision Making in Civil Aviation
In a video briefing Footnote 11 on risk-based approach principles, TCCA states that the Government of Canada has been moving the Public Service to a more performance, risk-based regulatory and management approach over the past five years, and TCCA has been actively adapting its entire program to reflect this shift in philosophy. The briefing emphasizes the importance of conducting risk analyses for all proposed changes to the safety framework, including granting exemptions, amending the Aeronautics Act, regulations or standards, and changing inspection and audit policies. It comments that "risk analyses are now a mandatory part of the civil aviation program."
Civil Aviation Directive (CAD) 30 Footnote 12 articulates the following policy: TCCA "applies risk management techniques and processes consistently in all its decision making, and documents these decisions, to ensure the greatest potential for enhancing safety and effectively managing the Civil Aviation Program." The directive requires that all risk management be consistent with the guidance material and that management decisions be documented. TC's publication Risk Management and Decision-Making in Civil Aviation (TP 13095) of April 2001 provides this guidance. Specifically, TP 13095:
- describes the basic concepts of risk and risk management,
- highlights typical decision situations in civil aviation, such as operational management decisions regarding allocation of limited resources and setting of priorities for regulatory oversight activities; and
- outlines a decision-making process for managing risk.
The TSB investigation examined two pertinent cases of the application of TCCA risk management policies and procedures. Both were prompted by increased TCCA workload associated with SMS implementation. In the first case, the risks associated with a PNR management proposal were evaluated to allocate resources and set priorities for regulatory oversight activities, but any policy guidance was not included. In the second case, the consequences of a resource allocation and oversight priority decision were examined, and the organization's risk management policy guidance was amplified. In accepting the second risk assessment, the DGCA directed that, during the transition to SMS, decisions by TC executives and managers regarding the extent and type of oversight were to be made based on case-by-case risk assessments (see Appendix D for a summary of both risk assessments).
1.17.2.3 Frequency of Inspection Policy and Frequency of Inspection Policy Document
CAD 20 laid out the responsibilities of personnel involved in the management and execution of oversight activities. To the extent that resources allowed, staff were required to comply with the Frequency of Inspection Policy Document (FOIPD). Footnote 13 Proposed adjustments to the inspection/audit cycle were to be evaluated using TC's risk management techniques and policies as per CAD 30. Any deviation from the frequency policy was to be documented and communicated to the relevant functional director. All audits and inspections were to be conducted in accordance with the Inspection and Audit Manual (IAM).
The FOIPD specified the frequency standards for a broad range of regulatory oversight activities. Rectification of non-conformances identified in an audit could be confirmed by follow-up on-site inspections. The FOIPD required 100 per cent completion of on-site audit follow-up tasks.
1.17.2.4 Inspection and Audit Manual
TCCA's Inspection and Audit Manual (IAM) (TP 8606E), revised 07/2005, provides policy and procedural guidance for planning, executing, and monitoring regulatory inspections and audits. The policy section of the manual indicates that routine audits are conducted for the purpose of determining an organization's level of regulatory conformance, and that "all applicable characteristics of the organization will be subject to review."
Audits are classified as "combined" or "specialty," with a combined audit targeting more than one functional area and a specialty audit focusing on specialties within a single functional area. Where an assessment of an organization's SMS is to be completed, the Safety Management Systems Assessment Guide (TP 14326) is used. The IAM specifies the requirements for audit follow-up. On-site follow-up is required except where audit findings are of a minor nature and pose no threat to aviation safety.
The progress of the air operator in completing audit-finding corrective actions is monitored. Progress is tracked on the follow-up sections of the corrective action form, the corrective action tracking form, or entered directly into the functional area database. Long-term corrective action plans are followed by the POI. Surveillance during audit follow-up is described as "the only means to ensure that organizations with non-conformances comply with regulatory requirements and respond satisfactorily to audit findings."
Audit follow-up is considered complete when the POI has accepted all the corrective actions, their status has been recorded in the audit file, the convening authority Footnote 14 has been advised, and a letter is forwarded to the air operator advising that the audit is closed.
1.17.2.5 Prairie and Northern Region Decisions Regarding Safety Management System Workload and the Regional Audit Program
The PNR audit program for 2006 comprised some 160 audits per year, including 7 large-scale regional combined audits requiring about 5 full-time equivalents (FTEs) and 153 smaller-scale audits requiring about 15 FTEs. Thirty-three companies were in the process of phasing-in a SMS.
PNR management was becoming concerned that, during implementation of SMS (and additional assessment activity associated with the introduction of new regulations), it might be difficult to maintain the audit schedule mandated by the FOIPD. Accordingly, the possibility of switching from divisional specialty audits to mandatory inspections during SMS implementation was considered in January 2006 (but subsequently rejected). It was recognized that a risk assessment would be required if this change were to be made.
By June 2006, PNR workload associated with validating the CAR 705 operators in phase 2 of SMS implementation had grown substantially. It was therefore decided that enhanced monitoring would replace the regional combined audit program for CAR 705 operators. Audits would still be conducted under enhanced monitoring if determined by risk factors derived through program validation (PV). PV is a focused review of one or more components of an organization (or a SMS). It assigns a score, which, if low, triggers enhanced monitoring techniques. Responsibility for tracking and scheduling of oversight, including assessing risk indicators to decide whether an audit of an operator would be warranted, was reassigned within PNR.
The PNR continued to conduct scheduled audits of CAR 703 and CAR 704 operators that were not yet implementing SMS. The PNR also continued to carry out other surveillance and monitoring activities mandated by the FOIPD, and retained the capability and intent to conduct audits based on safety intelligence and risk indicators.
PNR management considered that a regional level risk assessment regarding the replacement of the regional combined audit program was unnecessary; this was because responsibility for safety oversight and conducting risk assessments was simply being re-assigned within the PNR. However, a risk assessment was subsequently conducted in August 2007, which recommended an implementation plan to manage the risks associated with this decision.
1.17.2.6 Regulatory Inspections and Audits of Transwest Air
On 10 March 2005, PNR inspectors conducted an operational inspection of TWA. Footnote 15 The inspection was prompted by concern about reduced effectiveness of the company's operational control resulting from increased management workload associated with the addition of the SF340 aircraft. The inspection resulted in a finding that the company's flight time/duty rest period records did not conform to the company operations manual. TWA's corrective action plan was accepted by the POI and the inspection finding was closed on 13 June 2005.
As part of a pre-audit, the SF340 POI conducted an in-flight inspection of the company's CAR 705 airline operation on 21 December 2005. This inspection identified crew proficiency problems during an approach to Stony Rapids and the crew was subsequently removed from duty by the company. The company conducted training flights and line checks on the crew members before returning them to line service.
Between 16 and 27 January 2006, the PNR conducted a comprehensive regulatory audit to "analyze Transwest Air's policies and procedures to ensure that legislative requirements are met and an acceptable level of aviation safety is maintained." The audit was conducted in accordance with policy and procedures detailed in the IAM. The audit reviewed maintenance, flight operations, cabin safety, transportation of dangerous goods, and aviation occupational safety and health. Upon completion, an exit meeting was conducted at the company's main base in Prince Albert on 27 January 2006.
On 09 February 2006, the PNR audit coordinator forwarded two copies of the audit report to the TWA DFO. The audit made 34 maintenance and 11 operations findings identifying examples of non-conformance with the CARs, the CASS, or TWA company policies and procedures. The audit of flight operations revealed shortcomings with respect to flight crew requisite training and record keeping, and the abilities of the DFO and the chief pilot to exercise effective and meaningful operational control of the northern sub-bases, including La Ronge. The audit did not identify the widespread deviations from SOPs by the King Air pilots that were revealed by this TSB investigation.
Because the accident did not involve any maintenance or airworthiness issues, the TSB investigation examined only the flight operations audit findings and their follow-up. Two flight operations (FO) regulatory non-conformances, listed by audit finding number, will be discussed further in this report:
-
FO-05-01: The operations manager did not fulfill all responsibilities of the position as required by CASS 725.07(2)(a)(ii). For example, the company operations manual was out of date with respect to the CASS and CARs; and operational flight plans in La Ronge were found to be inconsistently completed; and
-
FO-06-01: PPC assessments were conducted on candidates who had not received all the training required, contrary to section 8.9.1 of the Approved Check Pilot Manual.
1.17.2.7 2006 Audit Corrective Action Plan
On 29 March 2006, the POI accepted part of the TWA proposed corrective action plan and advised that the company's proposed corrective action plans for other findings were rejected because the long-term corrective action proposed was inadequate.
On 26 May 2006, a PNR audit coordination officer forwarded to the POI the second TWA corrective action plan submission addressing those findings for which the first corrective action plan proposal had been rejected. The covering memorandum included explicit instructions for recording information on the corrective action forms provided as to whether the corrective action plan was accepted or rejected, and whether on-site follow-up would be required if the corrective action plan was accepted.
The corrective action form used was similar in layout and content to the corrective action form on page 49 of the IAM, but significant differences existed at the bottom of the forms (see Appendix E).
The bottom of the form used had, from left to right:
- one signature line for the audit follow-up office of primary interest (OPI),
- a line for the date of closure, and
- a second signature line to indicate that the person signing had closed the finding.
The bottom of the corrective action form in the IAM had, from left to right:
- a block for the date of closure,
- a block to indicate update of the National Aviation Company Information System (NACIS) database, and
- a signature block for the person closing the finding.
On both forms, the area for indicating whether on-site follow-up to the audit finding was required was ¾ of the way down the page.
Human factors principles of good form design require that a form should have a natural flow and conform to expected standards. Footnote 16 The normal use of a signature space is to attest to the accuracy of the data entered in the form.
The revised corrective action plans for FO-05-01 and FO-06-01 were accepted and the POI noted on the forms "satisfactory subject to confirmation" for FO-05-01 and "satisfactory" for FO-06-01, and recorded that on-site follow-up was required for both findings, with a proposed date of 01 September 2006. The POI signed both forms on the "Finding Closed by" line, with 12 June 2006 written on the "Date of Closure" line. There was no formal system available to assist inspectors in monitoring the due dates of follow-up action. The POI did not make any personal note or reminder regarding completing the FO-05-01 and FO-06-01 follow-up by 01 September 2006.
The NACIS database is used by TC for recording and monitoring regulatory oversight activities. On 15 June 2006, the audit coordination officer updated the NACIS database record for finding FO-05-01 to show that TC had accepted both the short-term and long-term corrective action plans and that the item was completed on 12 June 2006. The database record shows that administrative follow-up was required rather than on-site, and did not include a field for a proposed follow-up date. The TSB investigation did not receive any information regarding updates to NACIS records for finding FO-06-01.
On 02 August 2006, the PNR audit coordinator advised TWA that all corrective action and follow-up had been completed and that the audit was considered closed. The TSB investigation determined that TWA had implemented its corrective action plan for audit findings FO-05-01 and FO-06-01, but TC was actually unaware of this because the on-site follow-up proposed by the POI did not occur.
TWA executed its revised corrective action plan for FO-05-01 and FO-06-01, conducting 28 base and 28 ramp inspections in Saskatoon, Prince Albert, La Ronge, Stony Rapids, and Wollaston Lake from July to December 2006. Most inspections did not note any irregularities, although some inspections revealed regulatory non-compliance issues that were dealt with by management. The company also conducted 8 audits of over 40 pilot training records, including those of the captain and the first officer of TW350. A few audit forms had comments, mostly regarding currency dates.
The inspections and audits conducted by TWA focused on aspects of regulatory compliance that could be easily verified with documents. The corrective action plan did not require any in-flight inspections to verify compliance with the CARs and company procedures, and no in-flight inspections were conducted.
1.17.2.8 Audit Finding Tracking and Follow-up
The TSB investigation compared the hard copy audit-finding corrective action forms to a printout dated 16 April 2007 from the NACIS database for the TWA 2006 combined audit (see Appendix F). The forms showed 8 findings requiring administrative follow-up, 18 requiring on-site follow-up, 7 requiring both administrative and on-site follow-up, and 12 requiring no follow-up. The NACIS showed 24 findings requiring administrative follow-up, 20 requiring on-site follow-up, and 1 requiring no follow-up.
The comparison revealed that:
- The 12 findings that did not require follow-up were included in the 24 findings the NACIS showed as requiring administrative follow-up.
- Four findings that required on-site follow-up, including FO-05-01 and FO-06-01, were included in the 24 findings the NACIS showed as requiring administrative follow-up.
- Four findings that required on-site follow-up, including FO-05-01 and FO-06-01, were included in the 24 findings the NACIS showed as requiring administrative follow-up.
- Thirteen findings that required on-site follow-up according to the finding forms showed the same information in the NACIS.
- One finding that required on-site follow-up was listed in the NACIS as no follow-up required.
The NACIS finding tracking detail screen includes a data field for either administrative or on-site follow-up, allowing selection of only one type of follow-up. Consequently, the seven findings requiring both on-site and administrative follow-up were shown in the NACIS as requiring only on-site follow-up.
The comparison also examined the completion status of the findings. Although the NACIS showed all 45 findings as completed before the audit was closed in August 2006, the finding forms revealed that follow-up action had been completed and documented for only 31 of the 33 findings requiring follow-up. Findings FO-05-01 and FO-06-01 required follow-up action that was not recorded on the finding forms because no follow-up had been done.
1.17.2.9 Pilot Proficiency Checks
Regulations require that flight crews employed by air operators demonstrate their proficiency on each aircraft type. The sequences for these checks are outlined in the applicable CAR and associated standard. The candidate is given an oral examination by the check pilot with respect to aircraft systems and performance, is then briefed on how the check will be conducted, and completes the flight planning in accordance with the briefing. The check pilot observes the candidate in the aircraft or simulator conducting the normal and emergency procedures and assesses his or her proficiency against the limitations and procedures outlined in the AFM and the company's SOPs. After completion of the flight check, the check pilot debriefs the candidate on his or her assessment of the check and completes the required documentation.
TCCA's approved check pilot (ACP) program has transferred pilot checking responsibilities from TC inspectors to ACPs. TC Policy Letter 166, dated 08 July 2004, states "this initiative . . . is aimed at reducing the amount of time an inspector spends conducting pilot proficiency checks (PPCs) in favour of the more critical auditing and surveillance functions."
In Commercial and Business Aviation Advisory Circular (CBAAC) 0176R2 issued on 06 August 2004, TC indicated that too many inspector resources were being concentrated on conducting PPCs for those air operators without an ACP program. The CBAAC discussed a refocusing of inspector resources toward a more systematic approach to safety oversight, specifically a plan to "implement a reduction in the frequency with which TC inspectors conduct PPCs on pilots operating under subparts 703 and 704 of the CARs." The CBAAC implemented exemptions to the CARs allowing for a 24-month PPC frequency, and advised that "air operators can anticipate increased oversight activity in areas other than PPCs."
In CBAAC 0250 issued on 21 November 2005, TC published a plan to "eliminate the current provision of PPCs conducted by inspectors by December 31, 2007, with some exceptions." The exceptions encompassed annual monitor rides and PPCs for company executive and supervisory pilots, and a random number of PPC monitors to ensure that overall program expectations were being met.
The FOIPD specified two inspection frequencies for Activity Reporting and Standards System (ARASS) task 13D030, air taxi operations PPCs: 100 per cent of the PPCs for those pilots employed by organizations without ACPs, and 15 per cent of the PPCs for those pilots employed by organizations with ACPs.
The Approved Check Pilot Manual (TP 6533E), 8th edition, issued February 2006, was in effect at the time the captain and first officer of TW350 completed their PPCs. This edition stated that an ACP can be a company check pilot (CCP), a contract CCP, or a designated approved check pilot (DACP).
TWA employs ACPs. During the 12 months before an operational audit of TWA in September 2003, 55 PPCs had been conducted at TWA: 35 by TC inspectors, 15 by a CCP, and 5 by a contract CCP. During the period from 07 January 2006 to 07 January 2007, 90 PPCs were conducted at TWA: 17 by TC inspectors, 53 by CCPs, and 20 by DACPs. The PPC of the TW350 captain was performed by a DACP and the PPC of the TW350 first officer was performed by a CCP.
The investigation determined that both ACPs and TC inspectors considered that PPCs conducted by ACPs were likely more thorough evaluations of SOP knowledge and compliance than those conducted by TC inspectors because of the ACP familiarity with the aircraft and SOPs.
1.17.2.10 Aerodromes and Airports
TC defines an aerodrome as any area of land, water (including frozen surface thereof), or other supporting surface used or designed, prepared, equipped, or set apart for use either in whole or in part for the arrival and departure, movement or servicing of aircraft and includes any building, installations, and equipment in connection therewith. Footnote 17
An airport is an aerodrome for which, under Part III of the CARs, an airport certificate has been issued by the Minister. Airport operators are required to maintain and operate the site in accordance with applicable TC standards, and regular inspections are conducted by TC to confirm compliance. Standards for airports are more stringent than standards for aerodromes.
Where an aerodrome operator provides TC with information respecting the location, markings, lighting, use, and operation of the aerodrome, TC registers the aerodrome and publishes the information in the CFS or the Water Aerodrome Supplement, as applicable. Footnote 18 TC may refuse to register an aerodrome where the operator of the aerodrome does not meet the regulatory requirements for warning notices, wind direction indicators, lighting, prohibitions, and fire prevention, or where using the aerodrome is likely to be hazardous to aviation safety and, in such a case, does not publish information with respect to that aerodrome. Footnote 19 The operator of a registered aerodrome must notify TC immediately after any change is made to the location, marking, lighting, use, or operation of the aerodrome that affects the information published by TC.
The FOIPD specifies that TCCA regional aerodrome safety divisions must inspect 10 per cent of registered aerodromes annually, and describes this inspection task as a complete assessment of safety made by means of physical flight and ground inspections, review of the CFS entry, inspection briefings and debriefings, and preparation of the inspection report.
Registered aerodromes listed in the CFS are not certified as airports, and are not subject to regular inspections. Pilots intending to use registered aerodromes are expected to obtain current information from the owner/operator.
Sandy Bay is a registered aerodrome. It underwent eight inspections documented by TC aerodrome inspectors from 1982 to 1994. There were no documents of any inspections by TC after 1994.
The absence of inspections after 1994 was the result of a policy shift away from the requirements of the FOIPD, whereby inspection priority was given to certified airports with the objective to have them in full compliance with the applicable CARs and associated standards. Non-certified aerodromes would not be regularly inspected because of resource limitations.
The Sandy Bay aerodrome is not certified and as such is only required to meet the few basic regulations listed above. There are several hundred such aerodromes in the region, and, while the PNR continues to provide an oversight role for these facilities, inspectors are not able to attend them on a regular basis. The PNR conducts annual surveys to ensure that, for those aerodromes which are registered, the information published in the CFS is correct. TC also responds to any complaints or concerns raised about non-certified aerodromes.
1.17.2.11 Commercial Air Services at Uncertified Aerodromes
While unscheduled commercial air service is permitted at uncertified aerodromes, the CARs do not normally permit aerodrome operators to allow scheduled commercial air services to use an uncertified aerodrome. However, scheduled operations may occur between an airport and an aerodrome or between two aerodromes "if the air operator is authorized to do so in its air operator certificate." Footnote 20 Such authorization will "specify conditions in the authorization that will ensure a level of safety in respect of the use of the aerodrome that is equivalent to the level of safety" established by subpart 302 of the CARs.
In policy letter 121/AARM, dated 07 May 1998, TC provides a policy outlining procedures to be followed by inspectors when handling requests from air operators who wish to provide scheduled passenger service using an uncertified aerodrome. The procedures require, in part, that an on-site inspection of the aerodrome be conducted to determine the suitability of the aerodrome and to establish conditions that will ensure an "equivalent level of safety."
1.18 Additional Information
1.18.1 Crew Resource Management Training
The objective of crew resource management (CRM) is to reduce human error in aviation. CRM is widely accepted as the use of all human, hardware, and information resources available to the flight crew to ensure safe and efficient flight operations.
Measurements of the impact of CRM training show that, after initial indoctrination, significant improvement in attitudes occur regarding crew coordination and flight deck management. Footnote 21 In programs providing recurrent training and practice in CRM concepts, significant changes have been recorded in flight crew performance, with CRM-trained crews operating more effectively as teams and coping better with non-routine situations. Research also shows that, when there is no reinforcement of CRM concepts by way of recurrent training, improvement in attitudes observed after initial indoctrination tends to disappear.
Researchers have recommended that future CRM training should be based on the underlying premise that human error is inevitable and cannot be entirely eliminated, and see CRM "as a set of error countermeasures with three lines of defense." Footnote 22 The first defence is the avoidance of error, the second defence is trapping errors before they occur, and the third defence is mitigation of the consequences of errors that occurred but were not trapped.
In Canada, CASS 725.124(39) requires CAR 705 airline operators to provide all flight crew members with initial and annual recurrent CRM training. This requirement does not extend to CAR 704 commuter or CAR 703 air taxi operators. CASS 725.124(39) requires that, for CAR 705 operations, all crew members must receive initial CRM training covering subject categories that include attitudes and behaviours, communication skills, problem solving, human factors, conflict resolution, decision making, team building and maintenance, and workload management.
The human behaviour categories listed above have been described in detail in CRM research papers. One example regarding teamwork states that "good communications within the group, a high degree of situational awareness, and a comprehensive understanding of the decision-making process by all members of the group are all prerequisites for the creation of synergy and the effective performance of the team as a whole." Footnote 23
CAR 704 commuter and CAR 703 air taxi categories are assigned by TC based on number of seats and weight of aircraft, and do not take into account the complexity of an aircraft or the crew coordination required to operate it. CAR 703 air taxi operations range from single-pilot, single-engine aircraft with no requirement to coordinate crew activities, to multi-crew, multi-engine aircraft, with a requirement for levels of crew coordination comparable to that required for CAR 705 airline operations. The Canadian air taxi and commuter fleet includes a wide variety and large number of complex multi-engine aircraft operated by two pilots and using SOPs for operational crew coordination guidance. These aircraft are operated around the clock across Canada. CAR 705 airline operations typically operate with a dispatch system in place to support flight crew planning and decision making, whereas most CAR 703 and 704 operations operate under the pilot self-dispatch system discussed in sections 1.17.1.4 and 2.21. CAR 703 air taxi flight crews are employed at the industry entry level, often with little or no previous commercial aviation experience. Operations are commonly conducted in uncontrolled airspace with little assistance from air traffic services (ATS). Additionally, CAR 703 and 704 operations more frequently involve aerodromes with limited support infrastructure and services as compared to those aerodromes and airports used by CAR 705 airline operators.
As part of the investigation, six CAR 703 air taxi and CAR 704 commuter air operators were surveyed regarding their CRM training programs. It was discovered that five companies voluntarily provide initial and recurrent CRM training for their pilots. Three of those five companies provide recurrent CRM training annually, the fourth company every second year, and the fifth company every third year. Some of the training programs are combined with other training such as CFIT. The sixth company surveyed does not provide CRM training, but does include discussion of CRM concepts during other ground training.
TWA provided initial and annual recurrent CRM training to its CAR 705 airline crew members as required. Although no CRM training was required for TWA's CAR 703 air taxi or CAR 704 commuter flight crew members, the company's flight operations managers considered CRM training to be important and had voluntarily scheduled initial CRM training for air taxi and commuter pilots. However, the company's commuter and air taxi crews had not received CRM training before the accident occurred.
The captain of TW350 completed a TC CRM course in March 2000. The first officer of TW350 received 16 hours of human factors and pilot decision-making training between 2001 and 2003 as part of an aviation college training program. Neither the captain nor the first officer had received additional initial or recurrent CRM training after beginning employment with TWA, and no such training was required by the company or TC.
The TSB has investigated at least eight occurrences Footnote 24 in which crew members who had not received CRM training made errors that contributed to the occurrence. These occurrences span 15 years and occurred in widespread locations across Canada. Aircraft types were all two-engine turboprop aircraft with the exception of one four-engine jet transport aircraft. The eight occurrences involved 25 crew members and 149 passengers, and resulted in 7 fatalities and 1 minor injury. The potential for more serious consequences was high.
In its report on investigation A93P0131, the Board stated the following:
Notwithstanding the many pressures in the commercial flying environment that come to bear on operators and aircrew, the Board believes that, with the correct tools and skills, the likelihood of inappropriate decisions can be reduced. While some large air carriers can develop the necessary training on their own, other operators will require direction and assistance in setting up meaningful training programs. Therefore, to ensure that all operators and aircrew involved in commercial aviation have access to training for better coping with day-to-day operating decisions, the Board recommends that:
The Department of Transport establish guidelines for crew resource management (CRM) and decision-making training for all operators and aircrew involved in commercial aviation.
Transportation Safety Recommendation A95-11 (issued May 1995)
In response to Recommendation A95-11, TC indicated that CRM and pilot decision-making training would be mandated for all air operators who are required to adhere to the airline operations regulations. TC's response to Recommendation A95-11 addressed only CAR 705 airline operations and did not apply to CAR 703 air taxi and CAR 704 commuter operations. Consequently, the TSB assessment of TC's response was Satisfactory in Part.
The United States National Transportation Safety Board (NTSB) included improving CRM on its list of most wanted transportation safety improvements for years 2007 and 2008. The list stated that the FAA should act to require commuter and on-demand air taxi flight crews to receive CRM training.
On 01 May 2009, the FAA issued a notice of proposed rulemaking (NPRM) Footnote 25 regarding CRM training for crew members in Part 135 operations. The proposed rule would require all certificate holders conducting operations under Part 135 of the Federal Aviation Regulations (FARs) to include in their training programs CRM for crew members, including pilots and flight attendants. In considering this proposal, the FAA identified 268 accidents in Part 135 operations that may have been directly or indirectly related to ineffective CRM. After further review, the FAA found that 24 of these accidents were directly related to ineffective CRM and were responsible for 83 fatalities and 12 serious injuries. The FAA evaluated the risk of an accident caused by the absence of CRM training by reviewing accidents involving Part 121 operators during periods both before and after the 1997 implementation of CRM training requirements for those operators. The FAA concluded that, after implementation of the CRM training requirement, CRM training-related accident rates decreased by 11 per cent and fatal accident rates decreased by 25 per cent. In the NPRM, the FAA stated that effective CRM training for crew members is a critical element in the reduction of accidents and incidents.
1.18.2 Threat and Error Management
The International Civil Aviation Organization (ICAO) states that the fundamental purpose of CRM training is "to improve flight safety through the effective use of error management strategies in individual as well as systemic areas of influence" and proposes the integration of threat and error management (TEM) into CRM. Footnote 26
To better understand the role of the crew in managing risk during normal operations, the University of Texas Human Factors Crew Resource Project has developed the TEM model. TEM is a conceptual framework regarding aviation operations and human performance, and can be used in different contexts, including flight deck operations and occurrence investigation. Three basic components of TEM are threats, errors, and undesired aircraft states. Footnote 27 Threats and errors are part of every day operations to be managed by flight crews, and both are considered to have potential to cause undesired aircraft states. The TEM model has been effectively used to gather data during routine flight operations through line operations safety audits (LOSA).
The model is based on the premise that, in every flight, hazards that must be handled by the crew will be present. These hazards increase the risks during a flight and are termed threats in the TEM model. Threats include such things as unknown weather conditions, short runways, limited visual cues, altimeter errors, aircraft serviceability issues, unfamiliar airports, etc. Provided the crew members have an opportunity to handle the threat, effective management of the hazard leads to a positive outcome with no adverse consequences (that is, the crew members take action to mitigate the threat). However, mismanagement of the threat can lead to crew error, which the crew must also manage. Mismanagement of crew error may lead to an undesired aircraft state, which can lead to an accident. At any point, effective management of the situation by the crew can mitigate the risk and the situation may be inconsequential.
The TEM model identifies five types of errors: intentional non-compliance (violations of SOPs), procedural errors (slips and lapses in the application of procedures), communication errors (information is incorrectly transmitted or interpreted), proficiency errors (skill or knowledge is lacking to manage the aircraft), and operational decision errors (where a decision is taken that increases the risk of the flight). Crew responses to an error may be to trap the error by identifying and correcting it, to exacerbate the error by making a subsequent error, or to make no response to the error.
The most common crew behaviours cited for effective error management included vigilance and crew member advocacy and inquiry. Although threats and errors are present in the majority of flight segments, they rarely carry significant consequences because they are effectively managed by the crew. The effective management of risks on the flight deck is inextricably linked to effective CRM.
Flight crews must also manage undesired aircraft states, since they carry the potential for unsafe outcomes. Undesired state management is an essential component of the TEM model, as important as threat and error management. Undesired aircraft state management largely represents the last opportunity to avoid an unsafe outcome and thus maintain safety margins in flight operations. Footnote 28
1.18.3 Trans-Cockpit Authority Gradient
A steep authority gradient between crew members is a recognized potential barrier to good CRM. Footnote 29 The authority relationship between an aircraft captain and the first officer has been cited in many accidents and incidents. This trans-cockpit authority gradient can result from the actual differences in the age, experience levels, and rank of the crew members, as well as the way that the differences are emphasized by one or both of the crew members. In the case of the TW350 crew, the first officer was 28 years younger than the captain. The first officer had only eight months of commercial flying experience with less than 700 hours of total flight time, while the captain had been employed in the industry since 1980 and had over 8000 hours of total flight time.
Research has shown that there is an optimum trans-cockpit authority gradient to allow an effective interface between pilots on a flight deck. Footnote 30 The gradient may be too flat, such as with two equally qualified individuals, or too steep, as with a dominating chief pilot and a junior and unassertive first officer. In such cases, a degradation of performance may result with a chance of errors going undetected and uncorrected.
A study in the United Kingdom of 249 airline pilots confirmed the importance of this aspect of flight deck communication. Footnote 31 Nearly 40 per cent of the first officers surveyed said that they had on several occasions failed to communicate to the captain their proper doubts about the operation of the aircraft. Reasons for this appeared to be deference to the experience and authority of the captain and a desire to avoid conflict.
1.18.4 Development of Adaptations and Reduced Safety Margins
Time and resource pressures can result in individuals making adaptations to get the job done. While SOPs are prescribed in order to set boundaries for safe operations, individuals may experiment with the boundaries in order to become more productive. This leads to adaptations of procedures and a shift beyond the prescribed boundaries described in the SOPs toward unsafe practices. Footnote 32
One reason for this is that humans rarely perform work with strict adherence to prescribed rules or instructions. Procedures are often developed for a particular task in isolation from the work context. Performance requirements impose constraints on operators beyond what was considered (and available) when the task instructions were written. To get the job done, people work outside the defined rules. This is why studies of humans, even those working in high-risk, complex systems, have found that operators modify instructions and violate rules in ways that are quite rational given the actual workload and timing constraints (Dekker, 2006). Footnote 33
Without regular supervision, education, and enforcement of the expected boundaries, individuals are likely to continue to adapt procedures and cut corners until the actual unsafe boundary is found through the occurrence of a minor or major accident. Additionally, the communication of successful adaptations between crew members, such as the usefulness of GPS to provide distance to go or a straight-in approach to save time, will tend to lead to the spread of these adaptations throughout an organization unless adequate supervision is applied.
1.18.5 Previous Safety Action Regarding Crew Pairing Issues
Crew pairing issues have been documented as a risk to safety Footnote 34 and have been identified in previous TSB investigations, although these have focused on issues related to crew inexperience rather than crew incompatibility. TSB recommendation A93-03 addressed the need for crew pairing following occurrence A90H0002 at Moosonee, Ontario, on 30 April 1990:
The Department of Transport provide guidance for air carriers to assist in the effective pairing of flight crews.
Transportation Safety Recommendation A93-03 (issued May 1993)
In response to Recommendation A93-03, TC indicated that the issue of crew pairing was being addressed as a result of the recommendations contained in the Commission of Inquiry into the Air Ontario Crash at Dryden, Ontario, and that the issue was under active review. In addition, TC indicated that the FAA issued a NPRM for a regulation that would prevent the pairing of pilots if both have 75 hours or less of operating time on the type of aircraft being flown, and that TC expects to implement legislation similar to that of the FAA. Subsequently, CAR 705.108 came into force, which required Canadian airline category operators to apply the crew pairing standards published in CASS 725.108. The CASS 725.108 standards establish minimum experience requirements for flight crews and impose crew pairing restrictions for specific situations. These standards do not apply to CAR 703 air taxi and CAR 704 commuter operations. Section 1.17.1.5 discusses implementation of this regulation within TWA.
The TSB assessment of TC's response to TSB Recommendation A93-03 was Satisfactory in Part because the action by TC was limited to addressing crew experience on aircraft type. The TSB assessment concluded that TC's response would probably have little effect in preventing accidents attributable to poor crew pairing where pilots, although experienced on type, were unsuitably paired with respect to other aspects of the total operating environment.
1.18.6 Limited Visual Cues for Approach and Landing
Black holes are described in TC's Instrument Procedures Manual (TP 2076) as follows: "During night visual approaches to runways in dark, featureless areas such as unlighted woods or over water, the lack of ambient clues to orientation interferes with depth perception. Such areas are known as black holes." TP 2076 also identifies two hazards associated with black holes: disorientation after take-off and a tendency for pilots to fly too low on approach and collide with terrain short of the runway.
A greater number of visual cues, in particular any cues in the foreground and background relative to the runway, enables pilots to more accurately assess aircraft orientation relative to the runway. The absence of visual cues increases pilot workload and decreases the likelihood of a safe landing, such as in the case where a black hole effect can lead to a CFIT just short of the threshold. Footnote 35
The TSB has previously investigated occurrences where black hole hazards were found to be causal or contributory (see TSB reports A05O0225, A01C0236, A00A0051, A99A0131, A96O0034, A95C0197, A93C0169, and A90H0002). The occurrences investigated range from private operations at registered aerodromes to airline operations at certified airports, and include both approach and departure problems. Consequences of the occurrences ranged from minor aircraft damage with no injuries to aircraft destruction with fatal injuries. In one of the fatal accidents (TSB report A93C0169, which also occurred at Sandy Bay), the aircraft was operated by one of the pre-merger TWA companies. Considerable numbers of registered aerodromes with few visual cues for night operations exist in all 10 provinces and all three territories. Some certified airports are also affected by this phenomenon.
TC and the aviation industry have taken action to implement defences against the risks posed by black holes. Approach lighting systems, PAPI, and high-intensity runway lighting are used to provide more visual cues and help pilots better manage black hole hazards. However, many Canadian aerodromes are not certified, do not receive scheduled traffic, and are not required to have such lighting systems. Many of these aerodrome operators are unable to justify the costs associated with the installation and maintenance of improved aerodrome lighting and navigation aids.
Information about aerodrome lighting systems is available in flight information publications, including the lighting installed at Sandy Bay. However, this information does not currently include any cautionary notes explicitly identifying hazards associated with limited visual cues for approach and landing.
Education of pilots has been extensive. TC used TSB investigation A90H0002 as a case study for a human factors handbook, Footnote 36 including information on black hole effect hazards and suggested means to reduce the associated risks. TC has also published a number of articles in its newsletter Aviation Safety Letter, which is sent to every valid Canadian licensed pilot, on night flying and the hazards of black holes.
As part of a night VFR awareness campaign, TC produced a night VFR awareness briefing package for use by regional system safety offices during safety awareness presentations.
In the airmanship section (AIR) of the Aeronautical Information Manual (AIM), TC provides information and advice on various topics that help to increase knowledge. Detailed information, including suggested means to defend against hazards, is provided on topics including altimeter errors resulting from non-standard temperatures, winter flight operations, and whiteout conditions. Flight operations at night are discussed briefly in section AIR 2.16, but no information is provided regarding specific hazards or means to defend against hazards.
1.18.7 False Climb or Somatogravic Illusion
The somatogravic illusion occurs in conditions of poor visibility or in darkness when there is an absence of visual cues. Instrument-rated and experienced pilots are not immune to this illusion, which is a subtle and dangerous form of disorientation.
The illusion occurs because the body relies on sensory organs in the inner ear to maintain balance and, in the absence of visual cues, signals from these organs can produce a very powerful disorientation. In the case of an aircraft that is accelerating during a go-around, the sense organs of the inner ear of the pilot send a signal to the pilot's brain that is interpreted as tilting backwards instead of accelerating forward.
According to text in the Fundamentals of Aerospace Medicine, "A relatively slow aircraft, accelerating from 100 to 130 knots over a 10-second period just after take-off, generates +0.16 Gx on the pilot. Although the resultant gravitoinertial force is only 1.01 G, barely more than the perceptible force of gravity, it is directed 9° aft signifying to the unwary pilot a 9° nose-up pitch attitude." Footnote 37
If the aircraft nose is simultaneously raised, which is usually the case in a go-around, the pilot has a very strong sensation of climbing. The illusion of false climb tends to lead the pilot to lower the nose and descend. The aircraft then accelerates and the illusion can intensify. If the aircraft is being flown in proximity to the ground, ground contact can occur before the pilot can assimilate information from the aircraft's instruments, overcome the powerful illusion, and take corrective action.
1.18.8 Threshold Crossing Height and Ground Point of Interception
Aircraft final approaches typically use a 3° glide slope, which is about 300 feet descent per nm traveled. Threshold crossing height (TCH) is the height of the glide slope above the runway threshold and, for a 3° glide slope, the TCH is about 50 feet. Ground point of interception (GPI) is the point at which the glide slope intercepts the runway surface. For a 3° glide slope with a TCH of about 50 feet, the GPI is about 1000 feet from the runway threshold. These parameters coincide with most typical PAPI and instrument landing system (ILS) installations.
The CJY4 GPS waypoint, 1440 feet past the threshold of Runway 05, was the targeted GPI of TW350's descent profile of 300 feet per nm. Investigators calculated that this combination would result in a TCH of 71 feet or 40 per cent greater than the TCH for a typical PAPI or ILS.
1.18.9 Minimum Obstacle Clearance
Minimum obstacle clearance varies significantly between instrument approach procedure segments and also between instrument approach procedures depending on the type of navigational aid used. Information regarding minimum obstacle clearance is contained in TC's Criteria for the Development of Instrument Procedures (TP 308), July 1996, but is not included in the instrument approach procedures used by pilots and is not readily available to pilots in flight.
1.18.10 Altimeter Setting Procedures
The pressure altimeter used in aircraft is a relatively accurate instrument, but the altitude information indicated by an altimeter may differ greatly from the actual height of the aircraft above mean sea level or above ground. In instances of aircraft operating close to the ground or above the highest obstacle en route, especially when not flying in visual conditions, knowledge of actual ground separation or of "error" in the altimeter indication is of prime importance if such separation is less than what would be assumed from the indicated altitude.
CAR 602.127(2) specifies that "no pilot-in-command of an IFR aircraft shall commence an instrument approach procedure unless the aircraft altimeter is set to an altimeter setting that is usable at the aerodrome where the approach is to be conducted."
TC provides operational guidance regarding altimeter setting procedures in section 9.17 of the AIM. Minimum altitudes in instrument approach procedures meet obstacle clearance requirements when International Standard Atmosphere (ISA) conditions exist and the aircraft altimeter is set to the current altimeter setting for that aerodrome. Altimeter settings are considered current up to 90 minutes from the time of observation. Care should be exercised when using altimeter settings older than 60 minutes or when pressure has been falling rapidly.
Under conditions of extreme cold, aircraft true altitude will be lower than indicated altitude, reducing obstacle clearance to less than the minimum required. Consequently, corrections to published altitudes should be applied to ensure adequate obstacle clearance. The CAP indicates that "in conditions of extreme cold weather pilots should add the values derived from the altitude correction chart to the published procedure altitudes." Section RAC 9.17.1 of the AIM indicates that "for practical operational use, it is appropriate to apply a temperature correction when the value exceeds 20 per cent of the associated minimum obstacle clearance."
The minimum obstacle clearance for the Sandy Bay RCAP NDB 05 final approach segment is 350 feet, Footnote 38 20 per cent of which is 70 feet. Based on the published height above touchdown zone elevation (HAT) of 799 feet and an assumed temperature of −17°C at Sandy Bay, the cold temperature altitude correction that should have been applied to the RCAP NDB 05 minimum descent altitude was 108 feet (1780 + 108 = 1888 corrected MDA).
TWA Beech A100 King Air pilots interviewed did not use any standard practice in applying cold temperature altitude corrections. One pilot had never used such corrections and others began applying the correction at temperatures ranging from −10° to −20°C. The crew of TW350 did not discuss this issue and did not apply any temperature corrections to the minimum altitudes for the Sandy Bay RCAP NDB 05 instrument approach procedure.
Instrument approach procedures designed for use with altimeter setting sources more than 5 nm from the aerodrome reference point (ARP) include adjustments to procedure altitudes corresponding to the horizontal distance and elevation difference between the ARP and the altimeter source. A remote altimeter setting source is not authorized when the altimeter setting source is more than 75 nm from the ARP.
TWA King Air pilots had all flown to Sandy Bay and were all aware of the cautionary notes to use the Flin Flon altimeter setting and that it was only available for limited hours. The pilots did not use any standard practice when the Flin Flon altimeter setting was not available and were unsure whether there was a standard practice. Pilots proposed practices such as using the nearest available altimeter setting and adding 200 feet to minimum procedure altitudes, using the point of departure altimeter setting, or diverting if unable to operate under VFR.
1.18.11 Instrument Flight Rules Procedures at an Uncontrolled Aerodrome in Uncontrolled Airspace
In the AIM, section 9.13, TC provides operational guidance to pilots regarding landings at uncontrolled aerodromes as follows:
A straight-in landing from an IFR approach should not be used at an uncontrolled aerodrome where air-ground advisory is not available to provide the wind direction and speed and runway condition reports required to conduct a safe landing. The pilot should determine the wind and verify that the runway is unobstructed before landing. Where pilots lack any necessary information, they are expected to ensure that a visual inspection of the runway is completed prior to landing. In some cases, this can only be accomplished by conducting a circling approach using the appropriate circling MDA.
1.18.12 Non-Punitive Reporting Systems
An integral component of a SMS is a non-punitive reporting system. With a non-punitive reporting system, employees of an organization are given qualified immunity from punitive actions to encourage them to report occurrences and hazards. This qualified immunity has been demonstrated to significantly increase the number of hazard and occurrence reports made by employees, enabling an organization to gain a better understanding of risks present in its operations. Footnote 39
A decrease in reporting reduces the availability of critical information about the state of an organization that is needed to assess whether risk is being managed to an acceptable level. Inappropriate use of punitive actions reduces the number of occurrences and hazards reported by operating employees of an organization because of fear of punishment. Such a decrease in reporting has been demonstrated in the Netherlands following criminal conviction of air traffic controllers involved in occurrences. Footnote 40 Potential punitive action is also widely viewed as a significant factor affecting reporting of medical errors. Some theorists have raised concerns regarding the definition of human behaviour warranting punitive action and regarding who makes a judgement as to whether someone's behaviour warrants punitive action. Footnote 41
TC requires air operators implementing SMSs to have a non-punitive reporting policy in place by the completion of implementation of phase 2. TWA's non-punitive reporting policy provided immunity from disciplinary action for employees who reported safety deficiencies, hazards, or occurrences, and was published in the company's Safety Management Plan. The policy did not include information as to circumstances where punitive measures would apply.
1.18.13 Decision Support Tools
Self-dispatch systems are common throughout Canada and applied to all TWA flights, including TW350. Decision support systems can be used to assist in these circumstances.
A decision support system "is a system under the control of one or more decision makers that assists in the activity of decision making by providing an organized set of tools intended to impart structure to portions of the decision-making situation and to improve the ultimate effectiveness of the decision outcome." Footnote 42
1.19 Investigation Techniques
As part of the investigation, extensive interviews were conducted with line and management staff at both TWA and TC's PNR. TWA made all its King Air pilots available for interviews, enabling investigators to embed an 18-question flight crew survey within the interviews. The survey gathered information about the pilots' knowledge of and compliance with the CARs, company FOM, company King Air SOPs, and instrument approach procedures. The survey was informal in design.
2.0 Analysis
There were no records of any outstanding aircraft unserviceabilities and the investigation determined that the aircraft operated normally throughout the flight. Aircraft performance calculations show that the aircraft was capable of safely landing at Sandy Bay and that it was also capable of climbing during the go-around.
Therefore, the analysis focuses on human performance, management of safety by Transwest Air (TWA), and the provision of regulatory safety oversight by Transport Canada (TC).
2.1 Pilot Hiring
TWA had an established pilot hiring process that included a checklist of questions for interviewing a candidate and a check of references provided by the candidate. The process provided the company with an opportunity to verify that candidates met minimum screening criteria.
In the case of the captain and first officer, the absence of records documenting their hiring indicates that the company did not follow its established process. The captain's resume and a brief telephone inquiry to the captain indicated that he held appropriate licences and ratings issued by TC and that he met the company's King Air captaincy requirements. The company made an offer of employment to the captain (although the investigation could not determine which manager made the offer) and the captain accepted the offer.
The investigation revealed that the captain's previous employers had restricted his employment because of repeated non-compliance with regulations and standard operating procedures (SOPs) and had strong concerns about his flying proficiency and decision making. The employers did not readily provide information to the investigation about the captain's flying history and it is extremely unlikely that they would have responded to a reference check from TWA or any other prospective employer with anything other than an acknowledgment that they had employed the captain. In fact, the letters of reference the companies provided portrayed a substantially different perspective of the captain than did their training records.
The company could not have learned of potential weaknesses in the captain's past performance that would require close supervisory monitoring because of systemic constraints on free passage of objective factual information about employment candidates. Some of these constraints are federal and provincial privacy legislation as well as the potential for legal action by former employees.
These constraints are societal; consequently, they affect the entire aviation industry. Therefore, it is likely that many air operators experience difficulty obtaining standardized information on the quality of pilot performance because of systemic constraints on the free passage of objective factual information about employment candidates.
Similar conclusions have been made by the United States National Transportation Safety Board (NTSB). Refer to Appendix H regarding action taken in the United States by the NTSB and the Federal Aviation Administration (FAA) regarding standardized information on the quality of pilot performance.
2.2 TW350 Crew Pairing
As discussed in sections 1.5.4, 1.17.1.15, and 1.17.1.16, some pairing issues within the TW350 crew were identified by the northern chief pilot (NCP) and other King Air pilots. On two separate occasions, the NCP took some action to correct crew resource management (CRM) issues between the TW350 crew members.
The NCP was approached by the TW350 captain regarding the first officer's landings. After investigating, the NCP concluded that the first officer's performance was satisfactory and provided guidance to the captain to demonstrate landings, to coach the first officer, and to be more assertive.
The captain had opportunities to demonstrate landings on the occasions he was the pilot flying (PF). The captain coached the first officer during the final approach to Sandy Bay and he also used assertiveness when rejecting the first officer's suggestion to go around as well as when advancing the power levers during the go-around. Therefore, the NCP's intervention likely contributed to the captain adopting the recommended behaviours and applying them in operations. However, the underlying issue—the captain's concern about the first officer's ability to land the aircraft—was not fully resolved.
The NCP was approached by the TW350 first officer regarding the captain's performance at Meadow Lake. The NCP investigated and was satisfied that the captain understood the deficiencies represented by the poorly flown approach and poor crew coordination. The NCP concluded that it was not necessary to conduct a training flight to review SOPs or instrument procedures, or to assess the captain's flying proficiency and decision making with a line check. The NCP verbally counselled the first officer to be more assertive in the cockpit by identifying incorrect procedures or inaccurate flying.
Because the captain was the pilot not flying (PNF) of TW350, no determination can be made about the effectiveness of the counselling the NCP provided the captain regarding flying performance. However, many examples of absent or ineffective crew coordination occurred during TW350. Some of these examples are: the missed opportunity of the pre-flight crew briefing, the decision for the first officer to be PF, the decision to conduct the approach straight-in, and the execution of the go-around. The crew coordination issue the NCP had identified was not resolved by the NCP's counselling of the captain.
The first officer's suggestion to conduct a go-around is an example of ineffective assertiveness during TW350. Therefore, the assertiveness issue the NCP had identified was not resolved by the NCP's counselling of the first officer.
Additionally, there were other pairing issues within the TW350 crew that were not identified by the NCP or other flight operations managers, including: trans-cockpit authority gradient, communications, problem solving and decision making, conflict resolution, and operating practices that were substantial deviations from SOPs. All of these issues are targeted by the CRM training requirement for Canadian Aviation Regulations (CARs) subpart 705 airline crew members discussed in section 1.18.1.
There was a substantial age difference between the TW350 crew members, and the captain had significantly more experience in a broad variety of commercial aviation aircraft and operations than did the first officer. Two examples of ineffective CRM resulting from a steep trans-cockpit authority gradient are: the captain's disagreement with the first officer's advisories regarding the inbound approach track during the Meadow Lake incident and, during TW350, the first officer's unassertive suggestion to go around and the captain's rejection of the first officer's suggestion. Therefore, a steep trans-cockpit authority gradient existed between the TW350 crew members. This crew pairing issue existed on other flights involving this crew pair and was not identified by TWA company management. This issue fits into the CRM categories of attitudes/behaviours, human factors, and team building/maintenance. The investigation did not determine the influence of authority gradient between the captain and other pilots.
Examples of ineffective communications between the TW350 crew members are: the missed opportunity of the pre-flight crew briefing, the missed opportunities of challenges to deviations or omissions, the incomplete approach briefing, the first officer's unassertive suggestion to go around, and the captain's non-standard and ambiguous go-around call. This crew pairing issue existed on other flights involving this crew pair and was not identified by TWA management.
Examples of ineffective problem solving and decision making during TW350 are: the absence of any pre-flight aircraft performance calculations, the absence of the pre-flight crew briefing, the decision for the first officer to be PF, the decision to conduct the approach straight-in, the absence of altimeter corrections for below standard temperatures, the late decision to conduct the go-around, and the execution of the go-around. This crew pairing issue existed during previous flights involving this crew pair and also affected other King Air crews. This issue was not identified by TWA management.
Examples of ineffective conflict resolution between the TW350 crew members are: the captain's rejection of the first officer's unassertive suggestion to go around and the non-standard transfer of control practice used by the crew. These events very likely resulted from ineffective resolution of the captain's concerns about the first officer's ability to fly an approach and land the aircraft. This crew pairing issue existed during previous flights involving this crew pair and was only partially identified by TWA management.
Section 1.17.1.18 includes many examples of practices that were substantial deviations from SOPs both during the flight of TW350 as well as during other flights operated by other TWA King Air pilots. This crew pairing issue existed during previous flights involving the TW350 crew pair; TWA flight operations managers were unaware that these deviations were occurring and were unaware of the extent of the deviations. This issue fits into the CRM categories of attitudes and behaviours, problem solving, human factors, decision making, and workload management.
Refer to section 2.14.1 regarding the issues identified and the action taken by the TWA safety management system (SMS) investigation of the Fort McMurray incident.
Regulatory and TWA requirements regarding crew pairing are discussed in sections 1.17.1.5 and 1.18.5. All this guidance was issued subsequent to TSB Recommendation A93-03. The TSB assessed TC's response to Recommendation A93-03 as Satisfactory in Part because the proposed action at the time "would probably have little effect in preventing accidents attributable to poor crew pairing where pilots, although experienced on type, were unsuitably paired with respect to other aspects of the total operating environment." This assessment is applicable to the TW350 crew, where pairing issues adversely affected CRM.
TC crew pairing regulations to date have focused on crew experience and skill levels, which are concrete issues that are straightforward to assess. However, as this occurrence demonstrates, there are other aspects of the pairing that can have an impact on the crew's ability to effectively work together. Regulations and TC guidance material do not currently address the breadth of issues that can have an impact on the effectiveness of a crew pair, and that should be considered before making crew pairing selections.
Additionally, current crew pairing regulations apply only to airline operations, where there are relatively large numbers of pilots who can be scheduled to prevent ineffective crew pairings. There are no requirements for air taxi and commuter operations to have a crew pairing policy, and implementing a crew pairing policy by excluding permutations of pilots may be impractical in small commercial aviation operations where there are a limited number of pilot combinations. However, alternative strategies exist to mitigate the risk, including making operational hazards explicit to the crew members to enable them to apply CRM skills to mitigate the hazard, or providing specific CRM or flight management coaching before a flight is conducted.
While some crew pairing issues were identified and addressed, others were not, and TWA managers were unaware of the degree to which these factors could impair effective crew coordination. As a result, crew coordination was inadequate to safely manage the risks associated with TW350.
2.3 Absence of Recent Crew Resource Management Training
CRM training has developed over the years as an effective tool. Modern, well-designed CRM training now includes such things as threat and error management (TEM). CRM training is specifically designed to address much of the behaviour identified in this report regarding the interaction between flight crew members. Research has proven that CRM-trained crews operate more effectively as teams and cope more effectively with non-routine situations than do crews without CRM training. Additionally, when there is no effective reinforcement of CRM concepts by way of recurrent training, improvement in attitudes observed after initial indoctrination tends to disappear.
Although some commuter and air taxi operators have voluntarily provided CRM training to their pilots, some companies do not. Additionally, those companies voluntarily providing recurrent training do not necessarily do so on an annual frequency.
The captain of TW350 had received initial CRM training in 2000 and the first officer, in the period from 2001 to 2003, but neither pilot had received further CRM training before starting flying duties with TWA. The company had voluntarily planned CRM training for TWA's King Air operation in December 2006, but this training had been postponed and the accident occurred before any of the company's King Air pilots received CRM training.
The CRM training the TW350 crew members had received occurred well in the past and likely did not have any significant lasting effect on their behaviour in the absence of reinforcement in the form of additional initial or recurrent CRM training.
The counselling provided to each crew member by the NCP is an example of the company attempting to address CRM issues between the crew members. As discussed in section 2.2, while the TW350 crew members responded to corrective feedback, the individual counselling provided to the TW350 crew members by the NCP had limited effectiveness overall.
The TW350 crew members made an ineffective and dysfunctional team, despite individual counselling. The counselling had some positive effect; therefore, it is likely that formal CRM training could also have positively influenced the crew members' behaviour. Consequently, it is likely that recent CRM training would have assisted the crew of TW350 in better managing risks during the flight. The crew members' inability to work effectively as a team to avoid, trap, or mitigate crew errors encountered during the flight is likely, in part, because they had not received recent CRM training.
As described in section 1.17.1.18, the non-compliance was not confined solely to the TW350 crew pairing and extended to other King Air pilots. These TWA King Air pilot actions are examples of ineffective CRM in the categories of attitudes and behaviours, problem solving, decision making, and workload management.
Non-compliance was a widespread problem within TWA's King Air operation. None of the company's King Air pilots had received recent CRM training. Therefore, as with the TW350 captain and first officer, it is likely that recent CRM training would have assisted TWA's other King Air pilots in better managing risks during flight.
Some CAR 703 air taxi and CAR 704 commuter operators are unlikely to provide initial or recurrent CRM training to pilots in the absence of a regulatory requirement to do so. Therefore, some CAR 703 air taxi and CAR 704 commuter pilots may be unprepared to avoid, trap, or mitigate crew errors encountered during flight.
2.4 Decision for the First Officer to be Pilot Flying
TWA had two defences in place to ensure the most experienced crew member was flying when higher risks were anticipated. Captains were expected to fly the first leg of the day, and captains were expected to perform landings on runways less than 3500 feet long. Both of these defences were negated by the decision for the first officer to be the PF for the flight from La Ronge to Sandy Bay.
The SOPs required crew members to monitor other crew members and to identify any deviation or omission and bring it to their attention as soon as practicable. However, this third defence was negated because the first officer did not point out to the captain that the decision for the first officer to be PF deviated from company policies requiring the captain to be the PF. Although the investigation could not determine why the captain decided that the first officer would be PF that night, this decision was not an isolated incident, given that at least one other captain had also permitted first officers to land at Sandy Bay. The selection of the first officer to be PF to Sandy Bay resulted in the approach being flown by the less experienced crew member.
2.5 Use of Global Positioning System Distance to Aerodrome
The Canada Air Pilot (CAP) included an RNAV (GNSS) instrument approach procedure to Runway 05 at Sandy Bay and this approach used a missed approach waypoint coinciding with the threshold of Runway 05. If the crew members of TW350 had used this approach procedure, the global positioning system (GPS) would have provided distance-to-go to the threshold of the runway and it is likely that they would have calculated their descent profile using the distance from the threshold.
However, because the crew members were not trained to conduct GPS approaches, they were using the Restricted Canada Air Pilot (RCAP) non-directional beacon (NDB) approach to Runway 05, with primary track guidance from the automatic direction finding equipment. Sandy Bay did not have distance measuring equipment (DME), and the crew had the GPS programmed direct to the CJY4 waypoint to provide distance-to-go to the aerodrome.
Using the GPS distance-to-go improved the crew's awareness of the aircraft position in relation to the aerodrome. GPS distance-to-go also enabled the crew members to more accurately predict the aircraft's projected flight path than if they did not know their distance-to-go. Availability of GPS distance-to-go information enabled both crew members to use a descent profile of 300 feet per nm for their descent planning, as specified in TWA safety directive SD06-13 regarding approaches and the black hole effect.
However, the distance-to-go information depicted the distance between the aircraft and the CJY4 geometric centre waypoint, 1440 feet past the threshold of Runway 05. The crew members were likely unaware that their actual distance-to-go to the runway threshold was about ¼ nm less than what the GPS depicted.
The targeted ground point of interception (GPI) for the descent profile was the CJY4 active GPS waypoint, 1440 feet past the threshold of Runway 05. This descent profile would have had a threshold crossing height (TCH) of approximately 71 feet, about 40 per cent greater than the TCH for a typical precision approach path indicator (PAPI) or instrument landing system (ILS). However, because the temperature was colder than standard, the true aircraft altitude would have been lower than the indicated altitude. This would have reduced, by an unknown amount, the 71-foot TCH of the descent profile used by the crew.
The crew members were likely unaware of their ¼ nm error in the aircraft position in relation to the runway threshold. Although this spatial awareness error could have contributed to the aircraft being high on final approach when the crew acquired visual reference with the aerodrome, the investigation could not determine whether this was the case.
TWA aircraft were equipped with GPS, and although King Air crews had not yet received training, the GPS was routinely being used for distance-to-go during instrument approaches. Informal or unauthorized use of GPS by untrained crews during instrument flight rules (IFR) approaches can introduce risk, rather than mitigate it.
2.6 Limited Visual Cues for Approach and Landing
While the crew was aware of the black hole effect, there was no discussion in this context during the pre-flight preparation or the approach briefing. Once the flight crew members acquired visual reference with the aerodrome, they needed to make a transition from instrument flight to visual flight in order to continue the approach to landing.
During darkness, the Sandy Bay aerodrome and surrounding terrain provide limited visual cues to pilots for assessing the orientation of the aircraft relative to the runway. This limited visual environment increases the difficulty of transitioning from instrument to visual flight and requires continued reliance on aircraft instruments during the short visual portion of the flight.
The crew of TW350 successfully made the transition to visual flight, with the first officer controlling the aircraft and the captain monitoring airspeed and altitude. However, it was not until about one minute after acquiring visual reference that the captain identified that the aircraft was high on the descent profile. In TEM terms, the aircraft being high on approach was an undesirable aircraft state that the crew needed to manage. During the approach and attempted go-around, pilot workload increased and decision making became more complicated because of the limited visual cues available for assessment of aircraft orientation relative to the runway and surrounding terrain.
The aerodrome operator had not installed a PAPI at the aerodrome because of limited financial resources and concern about runway overruns. The company SOPs prohibited straight-in approaches at locations where VASIS, PAPI, or glide slope information was not available to pilots, but did not explicitly identify aerodromes where they were likely to encounter such conditions, such as Sandy Bay. Additionally, the instrument approach procedures for Sandy Bay did not include any cautionary notes identifying the limited visual cues present at the aerodrome.
Aerodromes with limited visual cues and navigational aids are not explicitly identified in flight information publications as hazardous for night/IFR approaches. Passengers and crews will continue to be exposed to this hazard unless aircraft and aerodrome operators carry out risk assessments to identify hazards and take mitigating action.
2.7 Short Runway
The SOPs required the first officer to complete performance calculations before the flight and the captain to review the calculations, but neither pilot did so. Pilot practice across the company's King Air operations was to base expectations of aircraft performance on past experience and pilots did not normally make performance calculations. Both of the occurrence pilots had previously flown into Sandy Bay without incident and they likely expected this flight to be little different from previous flights.
The Sandy Bay runway length was 2880 feet and the landing distance as calculated from the aircraft flight manual (AFM) was 1600 feet using a bare level paved surface. Subtracting landing distance from runway length results in an available touchdown zone length of 1280 feet from the threshold of the runway to the point at which runway remaining would be insufficient to stop the aircraft. Because the runway was snow-covered gravel rather than bare pavement, the aircraft landing distance would have been greater than 1600 feet, thereby reducing the length of the safe touchdown zone and requiring the flight to touch down closer to the threshold. However, the crew was using a descent profile with a GPI 1440 feet past the runway threshold and at least 160 feet beyond the end of the safe touchdown zone.
The crew members did not assess the aircraft performance and did not identify runway length as a threat. Consequently, they did not discuss and agree on a point at which a safe landing was no longer possible and were unprepared to make an informed and timely go-around decision as a crew.
2.8 Rejection of Go-Around Suggestion
The crew acquired visual reference with the runway lighting approximately four miles or two minutes before the threshold, while the aircraft was still descending toward minimum descent altitude (MDA). Because the crew was using GPS distance-to-go, the aircraft was higher than the crew expected, resulting in an undesired aircraft state. The captain identified that the aircraft was high on the approach and he managed this undesired aircraft state by continuing the approach and coaching the first officer.
The first officer subsequently suggested a go-around, without identifying the threat or recommending a change of plan in a more assertive form of communication. Such behaviour is typical of this type of crew pairing where barriers to effective CRM have not been addressed. This is an example of ineffective CRM components of communication skills, problem solving, and conflict resolution. The situation was worsened because the captain had prior concerns with the first officer's landings and was likely predisposed to discount or disregard the first officer's suggestion, and the crew pairing was also affected by a steep trans-cockpit authority gradient. These are examples of ineffective CRM component of conflict resolution.
The captain's instruction to continue the approach occurred only one second after the first officer's suggestion to go around, indicating that the captain had likely already decided that a landing could be made and a go-around was not necessary. That the captain held this mental model and did not share it with the first officer is an example of ineffective CRM components of crew communication and problem solving. The captain continued to coach the first officer rather than taking control of the aircraft himself.
Coaching the first officer introduced a time lag into the control of the aircraft because of the additional time required for the captain to formulate a verbal command, communicate it to the first officer, and for the first officer to perceive and interpret the verbal command. Given the short time period between crossing the runway threshold and reaching the point where a landing could no longer be made safely, this control time lag decreased the likelihood that descent profile and airspeed corrections would be made before touchdown. This is an example of ineffective CRM components of problem solving and communication skills.
The crew was focusing on landing the aircraft and had not discussed and agreed on a point at which a safe landing was no longer possible. This is an example of ineffective CRM component of problem solving.
The first officer suggested a go-around at an appropriate time. However, ineffective CRM coupled with inadequate preparation by the crew resulted in the captain rejecting this suggestion.
2.9 Go-Around Decision and Execution
The crew continued the approach past the point where the aircraft could be safely stopped on the runway. This was another undesired aircraft state that the crew needed to manage by doing a go-around from the landing flare.
The captain's communication to the first officer of his decision to abandon the landing attempt and conduct a go-around was non-standard and ambiguous. Consequently, the first officer did not immediately increase the engine power to initiate the go-around.
During the go-around, the first officer, who was the designated PF, made calls and actions both the PF and PNF were responsible for, and the captain, who was the designated PNF, made calls and actions both the PNF and PF were responsible for. The crew's actions were uncoordinated and did not follow the go-around sequence in the SOPs. Consequently, crew coordination was ineffective during a critical phase of flight.
The captain decided to initiate a go-around, but his communication of this decision to the first officer was non-standard and did not have the desired effect of triggering the standard sequence of go-around actions required.
2.10 Transfer of Control
Procedures for clear and consistent verbal communications prevent confusion between the pilots as to who has control of the aircraft, and TWA had such an aircraft control transfer procedure that was standard throughout its fleet. However, because the captain had concerns about the first officer's ability to land the aircraft, during previous flights, he had taken control of the aircraft from the first officer on numerous occasions, sometimes doing so using the phrase in the SOPs, "I have control," sometimes using phrases that differed from the SOPs, and sometimes without making any verbal statement. It is possible that the captain occasionally felt that he did not have sufficient time to make a verbal statement when taking control. In instances when the captain took control without making any verbal statement, the first officer's practice was to release the controls upon sensing pressure on the controls from the captain's control inputs.
As the PF during the approach, the first officer was responsible for advancing the power levers when a go-around was initiated and the captain, who was the PNF, was responsible for ensuring that maximum power was set. However, because the captain's communication to the first officer of his decision to abandon the landing attempt and conduct a go-around was non-standard and ambiguous, the first officer was unsure of the captain's intentions and consequently did not immediately advance the power levers to initiate the go-around. Four seconds after communicating his intent to initiate a go-around, the captain advanced the power levers to a high-power setting, thus ensuring maximum power was set, an action specified in the SOPs for the PNF. The captain almost certainly took this action because it was clear to him that they could not land safely on the remaining runway and the first officer had not responded to the captain's communication of his intent to initiate a go-around.
The investigation examined several possible scenarios of aircraft control during the go-around:
- The first officer was in control.
- Both pilots were attempting to control the aircraft.
- The captain was in control.
- Neither pilot was in control.
Immediately after the captain had advanced the power levers, the first officer perceived pressure on the control column and observed the captain's hand on the control column. Believing the captain was taking control without making any verbal statement, the first officer released the control column, also without making any verbal statement, using the non-standard practice they had employed on previous flights. Therefore, the first two scenarios listed above did not occur because the first officer released the control column.
On previous flights, the captain had taken control from the first officer both on approach and during landing. Given the captain's mistrust of the first officer's ability to land the aircraft, the lack of response from the first officer to the captain's ambiguous go-around communication, and the fact that the remaining runway was insufficient to land safely, it is very likely that the captain took control of the aircraft from the first officer using the non-standard transfer of control practice the crew had developed, and became the PF for the remaining 20 seconds of the flight.
The scenario in which neither pilot was controlling the aircraft is considered very unlikely.
2.11 Standard Operating Procedures Discrepancy – Flaps
The SOPs text description of the go-around procedure called for flaps to be initially set to approach, while the flight profile diagrams called for flaps to be selected up. Likely because of this difference, pilots interviewed had varying descriptions of the go-around procedure, with some pilots describing the initial flap selection as flaps to approach, and some as flaps up.
The discrepancy in the SOPs describing the selection of flaps during go-around likely led to both pilots independently operating the flap control lever, distracting them from monitoring the climb performance during the go-around.
2.12 Somatogravic Illusion
At 2002:23, when the power levers were advanced to a high-power setting, the aircraft would have been about halfway along Runway 05, between the threshold and departure end. Assuming the aircraft was about 10 feet above the runway at the time, the aircraft altitude at the beginning of the go-around would have been about 1011 feet above sea level (asl).
At 2002:31, when the captain called positive rate and gear up, the aircraft would have been flying past the departure end of the runway into an area with no external visual references available to the crew. It would have been necessary for the crew to transition from visual references to instruments in order to control the aircraft.
At 2002:32, the first officer selected the landing gear UP and then selected the flap lever to UP. Immediately afterward, the captain re-selected the flaps to the approach setting, an action that could have diverted his attention from monitoring the instruments and controlling the aircraft.
During the go-around, the first officer observed the altimeter indicating 100 feet below the aerodrome elevation and perceived sensations of being pushed back in the seat and the aircraft pitching up, and believed the aircraft was climbing. However, the aircraft collided with trees at 2002:43, at an altitude of about 1030 feet asl.
Although the aircraft vertical flight path and performance during the go-around could not be determined with certainty because the aircraft was not equipped with a flight data recorder (FDR), the TSB calculated that the aircraft was capable of climbing at 1250 feet per minute (fpm) during the go-around. Twenty seconds elapsed from power lever advancement to collision with the trees, during which time the aircraft was capable of climbing from 1011 feet asl to about 1400 feet asl.
Because the aircraft altimeters were set to an invalid altimeter setting, and because the below standard temperature would have caused the altimeters to indicate a higher altitude than the aircraft true altitude, the investigation could not determine whether the aircraft did descend during the go-around, as indicated by the first officer's observation of the altimeter. However, the terrain from the departure end of Runway 05 descends gradually from 1001 feet asl at the runway to 915 feet asl at the river surface, and it is certainly possible that the aircraft could have descended.
Aircraft performance during the go-around would have been similar to the example cited in section 1.18.7, resulting in a linear acceleration that was sufficient to have caused a false sensation of excessive aircraft pitch angle. It is possible that the aircraft did have a positive rate of climb at the time the captain called positive rate. However, it is likely that a somatogravic illusion caused the PF to lower the nose of the aircraft. Consequently, the aircraft did not maintain a positive rate of climb and collided with the trees.
2.13 TW350 Crew Training and Competency
The crew of TW350 held valid licences and ratings issued by TC, and met the experience and qualification requirements of the TWA Flight Operations Manual (FOM) for CAR 703 air taxi operations. The initial flight training provided by the company met the requirements of CAR 703. On completion of the training of both crew members, their technical competency was assessed as satisfactory by approved check pilots (ACPs). The first officer immediately entered line service, while the captain received extensive line indoctrination training before entering unrestricted line service.
The first officer and captain met competency standards on the completion of their initial flight training before they began employment as line pilots. However, this performance check was done eight months before the accident. Section 2.15 will discuss the erosion of competency standards during line employment of the crew.
2.14 Supervisory Deficiencies and Deviations from Required Procedures
2.14.1 Supervisory Deficiencies
The high supervisory workload and wide span of control of the chief pilot had been a known problem for several years. The company was aware of the workload issue and hired a second chief pilot to better distribute the managerial responsibilities. Although the northern chief pilot (NCP) was hired in April 2006, supervision of all company pilots, including both the captain and the first officer of TW350, remained the responsibility of the overloaded southern chief pilot (SCP) until September 2006, when TC approved the NCP's nomination.
The NCP's previous aviation supervisory experience was in smaller, less geographically dispersed operations with far fewer pilots to supervise and he needed to adapt his supervisory practices to his new circumstances at TWA. Because the NCP did not fly as a King Air crew member, his contact with King Air pilots was limited to meetings on the ground. Consequently, the NCP had little or no direct opportunity to observe the proficiency of the King Air pilots or their compliance with standards, policies, and procedures.
As discussed in sections 1.17.1.3 and 1.17.1.18, the company provided extensive guidance to flight crews in its FOM and SOPs on how the company expected them to manage threats that existed in its operation. However, the crew of TW350 and other King Air pilots commonly deviated from required procedures and policies, and the company's flight operations managers were unaware of the existence or extent of these deviations that affected the pilots' competency.
The NCP investigated both the captain's report of the first officer's unsatisfactory landings and the first officer's report of the captain's unsatisfactory proficiency and decision making at Meadow Lake. The NCP did not record his process, findings, or corrective action. In response to the captain's report related to landings, a supervisory intervention was made by having the first officer's landings assessed by a training pilot. However, the first officer's report, which provided detailed information about significant deviations from SOPs and expected proficiency norms by the captain, did not elicit any assessment of the captain's proficiency by training flights or line checks.
The actions taken by the NCP varied substantially from the actions taken one year earlier by the SCP when a TC in-flight inspection of the company's CAR 705 airline operation identified crew proficiency problems during an approach to Stony Rapids in December 2005. In this case, the SCP removed the crew from duty and subsequently verified the crew's competence by conducting training flights and line checks on the crew members before returning them to line service.
The responsibilities of a chief pilot specified in the TWA FOM were general in nature (for example "the supervision of flight crew") and the FOM did not provide specific guidance on how the supervision was to be conducted. Consequently, supervisory practices varied from one manager to another and from one situation to another.
Although the company was in an early phase of SMS implementation and was still developing related processes for investigating incidents and hazards, the Fort McMurray incident investigation was done under the SMS, was well documented, and included well-defined corrective action. The SMS investigation found that the incident was the result of lack of situational awareness, and immediate corrective action was punitive in the form of unpaid suspensions for both crew members. Long-term corrective action included a safety directive to all pilots regarding CARs infractions, and a plan for pilot meetings to discuss the issue. Follow-up action included a line check of the crew.
While the Fort McMurray SMS investigation was better documented and included better defined corrective action than the Meadow Lake investigation done by the NCP, the Fort McMurray investigation did not fully identify the cause of the incident and did not include corrective action for that cause. Poor situational awareness is not an underlying factor but rather a symptom of a deeper problem. The investigations of initial occurrences involving the crew of TW350 did not result in effective corrective action because the company's investigative practices did not detect or address the underlying proficiency, compliance, and supervisory problems that had resulted in the incidents being investigated.
Although TWA had provisions in its flight crew training manual (FCTM) to document line checks, no criteria were established governing when line checks would be conducted. Additionally, the company did not identify the TW350 captain's or first officer's proficiency or general compliance as deficiencies. Consequently, no line checks were conducted individually or as a crew before the Fort McMurray incident. Following the Fort McMurray incident, the NCP did not schedule the line check proposed during the SMS investigation. No verification of the crew's competency was made before the crew members were returned to service following the suspension, no line check was scheduled for January 2007, and no line check was conducted before the accident.
Crew practices during the occurrence flight deviated from required procedures, and these types of deviations were common across the company's King Air operation. Although the company was aware of repeated CARs deviations by its flight crews, deficiencies in supervisory activities permitted the undetected development and persistence of substantial and widespread deviations from SOPs within the King Air operation, especially with the crew pairing of the captain and first officer of TW350.
2.14.2 Altimeter Errors Resulting from Lower-than-Standard Temperatures
Flight crews were provided guidance in the TC Aeronautical Information Manual (AIM), the TWA SOPs, and the CAP regarding temperature corrections to published altitudes to ensure adequate obstacle clearance. The CAP and TWA SOPs both indicated that pilots should add the values derived from the altitude correction chart to the published procedure altitudes in conditions of extreme cold weather, but did not specify when to begin doing so. The only clear guidance as to when to apply altitude temperature corrections is in the AIM, section 9.17.1, which indicates that it is appropriate to apply a temperature correction when the correction exceeds 20 per cent of the associated minimum obstacle clearance.
TWA Beech A100 King Air pilots interviewed did not use any standard practice in applying cold temperature altitude corrections. The crew of TW350 did not discuss this issue and did not apply any temperature corrections to the minimum altitudes for the Sandy Bay RCAP NDB 05 instrument approach procedure.
The cold temperature altitude correction for the Sandy Bay RCAP NDB 05 minimum descent altitude was 108 feet, and exceeded 20 per cent of the minimum obstacle clearance for the final approach segment. Consequently, a correction of 108 feet should have been added to the MDA for the approach. Because the temperature correction was not applied to the MDA, the obstacle clearance on the approach would have been about 108 feet less than the minimum required.
This issue did not contribute to the accident because weather conditions were such that the crew acquired visual contact with the aerodrome before reaching the MDA. However, because of the variation in minimum obstacle clearance and the absence of in-flight information about it, flight crews are unlikely to follow the guidance provided in the AIM regarding when it is appropriate to apply altitude temperature corrections.
Inconsistent application of temperature corrections by flight crews can result in reduction of obstacle clearance to less than the minimum required and reduced safety margins.
2.14.3 Unknown Weather and Runway Conditions at Destination
Pilots require ceiling and visibility information to determine whether an instrument approach is likely to be successful. Wind information is required to decide which runway will enable landing into the wind. Information regarding runway surface conditions and occupancy status is required to decide whether a safe landing is possible. Wind and runway information is often provided by ground communication facilities or through distribution of weather reports and NOTAMs (notice to airmen).
However, where no information is available, pilots must make visual observations of wind direction indicators, runway surface conditions, and occupancy status. Operations specification (OPS SPEC) 99, the TWA FOM, and the TC AIM all provided guidance to flight crews regarding these requirements. The RCAP NDB 05 instrument approach procedure also included a cautionary note to verify that the runway was unobstructed. If necessary, this could require a circling approach to enable a visual inspection of the runway.
Additionally, the TWA King Air SOPs prohibited straight-in approaches at aerodromes where VASIS, PAPIs, or glide slopes were not available. Half of the TWA King Air pilots interviewed were not aware of the company's prohibition of straight-in approaches. Even those pilots aware of the prohibition reported occasionally flying straight-in approaches to avoid manoeuvring with limited visual cues.
No pre-flight information was available for the Sandy Bay weather or runway conditions, and no ground communications facility existed to provide this information to the crew before landing. The absence of ceiling and visibility information posed little threat to TW350 because the flight could return to La Ronge if the crew members did not acquire visual reference with the aerodrome during the approach. However, because they did not visually inspect the aerodrome before attempting to land, the crew members were unaware of the wind direction, runway surface condition, or occupancy status before landing.
The plan to fly the approach straight in was proposed by the first officer, and the captain concurred with this plan. The captain was required to point out to the first officer that the plan deviated from the FOM and SOP requirements, but did not do so. Consequently, the defences in the FOM and SOPs were negated.
The approach briefing was another opportunity for the crew to identify and manage the threats posed by the unknown weather and runway conditions. However, the briefing did not include all the elements required by the SOPs nor additional information about threats.
The TW350 crew's attempt at landing without first visually inspecting the aerodrome was common throughout the TWA King Air operation. This practice presents a risk to all flights because not knowing the wind direction introduces a risk of a downwind landing with increased landing distance, and not knowing runway condition before touchdown leaves the crew unprepared for potential post-touchdown problems such as runway obstructions or unsafe runway surface conditions.
The practice of not visually verifying wind/runway conditions at aerodromes where this information is otherwise unavailable increases the risk of post-touchdown problems.
2.14.4 Current Altimeter Setting not Available
TWA did not have any policies regarding dispatch of aircraft to destinations where the altimeter setting would not be current on arrival, and did not provide flight crews any guidance on this situation. Although all the company's King Air pilots were aware that the Flin Flon, Manitoba, altimeter setting was sometimes not available, pilot practices regarding how to deal with this situation varied widely.
The instrument approach procedures for Sandy Bay included corrections for and required the use of the Flin Flon altimeter setting because no on-site altimeter setting was available at Sandy Bay. The Flin Flon altimeter setting was not available between 1800 and 0600, and altimeter settings from other locations reporting continuously were not designated for use with the approach procedures because they exceeded the 75 nm limit for a remote altimeter setting source.
The crew members of TW350 did not identify that the Flin Flon altimeter setting would not be current for their arrival. Consequently, they did not have any plan for how to conduct the approach without a usable altimeter setting. Based on CAR 602.127(2), the Sandy Bay instrument approach procedures were not usable during the period the Flin Flon altimeter setting was not current (1930-0600). Approaches during this period should have been conducted under VFR. This issue did not contribute to the accident because the weather conditions were such that the crew of TW350 acquired visual contact with the aerodrome before reaching the MDA.
The company dispatched flights to Sandy Bay without a standard means for crews to deal with non-current altimeter settings. Use of non-current or inappropriate altimeter settings can reduce minimum obstacle clearance and safety margins.
2.15 Tranwest Air's Disciplinary Policy
As part of its SMS implementation, TWA had published its non-punitive reporting policy, which provided immunity from disciplinary action for employees who reported safety deficiencies, hazards, or occurrences. However, at the time of the occurrence, the company's SMS was still in phase 2 of implementation and the non-punitive reporting system was not yet operating.
After repeated flight crew regulatory infractions, TWA implemented a punitive regulatory enforcement policy. The first use of the policy occurred on 27 November 2006, when it was applied to the occurrence crew. Meetings with pilots to discuss repeated violations did not occur until after the accident.
The investigation identified many instances where both the TW350 crew and many of the other TWA King Air pilots were unaware of what the correct procedures were and did not apply them either correctly or at all during operations. These included not completing performance calculations or reviewing them before flight (SOP 3.3), first officers flying the first leg of the day (TWA unwritten policy), conducting straight-in approaches when prohibited (SOP 3.25), use of GPS for distance-to-go when not trained in GPS approaches, operating with invalid altimeter settings under IFR, and not correcting altimeter settings for cold temperatures. Each of these issues extended beyond the crew of TW350 and also applied to other TWA King Air pilots.
The captain's history of non-compliance indicates that he had a predisposition toward deviations from required procedures, but does not in itself support a conclusion that the non-compliance was deliberate. The crew of TW350 and most of the other TWA King Air pilots were likely unaware that the many policy and procedural deviations identified by this investigation were actually deviations. Some of the SOP deviations were adaptations. As described in section 1.18.4, adaptations occur when humans adapt their behaviour to their work. Examples of these adaptations are the use of GPS enabling straight-in approaches and the TW350 crew's transfer-of-control practice. The deviations within the TWA King Air operation almost certainly developed into routine practices for the flight crews and were not deliberate digressions.
Without increased supervisory surveillance to identify routine deviations, crews were unlikely to identify practices that were no longer conforming to established procedure or policy. The new disciplinary policy, designed to stop conscious deviations, was unlikely to have the rapid, broad impact that was intended because it was not accompanied by proactive identification of routine deviations. For example, the company's corrective action plan following the Fort McMurray incident primarily focused on dealing with the crew and did not actively seek signs of systemic problems within the company's operations.
The disciplinary policy had been implemented only six weeks before the occurrence flight, and there had been very little time for the new policy to have an impact on the performance of the company's flight crews. The company's disciplinary policy, designed to prevent deliberate violations, did not stop some deviations seen in the occurrence flight where the crew did not perceive the degree to which their practices varied from the required procedures.
While punitive discipline may be appropriate in some cases, in a SMS environment, inappropriate use can result in a decrease in the number of hazards and occurrences reported. This reduces the effectiveness of a SMS.
2.16 Transwest Air Management Workload and Effectiveness
The effectiveness of operational management personnel is dependent not only on their knowledge and skill, but also on the way the team is organized to handle the workload and to work with each other. TWA had all the policies and procedures required by TC to establish its operational control system in the FOM, FCTM, and SOPs. The company's operations had expanded as a result of amalgamation, company growth, and acquisitions, with only minor changes in the management team size and structure.
In recognition of the high workload associated with company growth and more pilots, the company hired the NCP. The NCP was trained on the SF340 and was subsequently approved by TC as an additional flight operations manager about four months before the accident.
A significant challenge the team faced was the repeated absences of the previous Director of Flight Operations (DFO) on sick leave, shifting workload onto other team members who were already busy with their own duties. This was a serious issue, as indicated by the notice of suspension issued by TC when it occurred in 2005. When the previous DFO went on extended sick leave in November 2006, the company quickly nominated the safety manager to become the DFO, and this was approved by TC on 08 December 2006.
The DFO, SCP, and NCP were based in Saskatoon, Saskatchewan, and fulfilled their line flying obligations on CAR 705 airline aircraft rather than the company's air taxi fleet. The need to travel to supervise subordinates, plus the need for managers to work as line captains imposed additional time pressures on an already busy team. Because they did not routinely fly with air taxi pilots, company management pilots had limited opportunity to directly supervise air taxi pilots and monitor their conformance with company policies and regulatory requirements.
The company management structure and workload, combined with the location of managers away from the remote bases of operations, reduced the effectiveness of operational control.
2.17 Prairie and Northern Region Resource Reallocation and Risk Management
Risk management is one of the fundamental concepts articulated in Transport Canada Civil Aviation (TCCA) strategic planning documents, and this philosophy is established as policy in Civil Aviation Directive (CAD) 30. The CAD 30 policy statement indicates that TCCA will consistently apply risk management techniques and processes in all its decision making. CAD 30 requires the use of risk management techniques when allocating resources. The publication entitled Risk Management and Decision-Making in Civil Aviation (TP 13095) provides examples of typical decision situations where use of risk management processes are appropriate, including operational management decisions regarding allocation of resources and setting of priorities for regulatory oversight activities. Additionally, the TCCA video briefing on risk-based approach principles indicates that risk analyses are a mandatory part of the civil aviation program. In March 2006, the Director General, Civil Aviation (DGCA) directed that decisions by TC executives and managers regarding the extent and type of oversight during the transition to SMS were to be made based on case-by-case risk assessments.
The decision was made to replace the PNR scheduled regional combined audit program with other oversight activities—focused inspections, program validation, SMS validations, enhanced monitoring and (if necessary) audits. This is an example of both regulatory oversight activity prioritization and allocation of resources. These decision types are identified in TP 13095 as appropriate for the application of risk management processes.
However, at the time of the decision in June 2006, no risk assessment was conducted regarding the replacement of the regional combined audit program by other oversight activities. A PNR risk assessment of this decision was subsequently conducted in August 2007 and recommended an implementation plan to control the risks associated with the decision.
PNR management practices at the time of the June 2006 replacement of the regional combined audit program, in order to manage SMS workload, did not conform to the TCCA risk management decision-making policies. This issue did not contribute to the accident, but was identified during the TSB investigation's examination of regulatory oversight of TWA. Reallocation of resources without assessment of associated risk could result in undetected regulatory non-compliance.
2.18 Transport Canada Oversight
TCCA's PNR regulatory monitoring and oversight of TWA was conducted using inspection and audit procedures specified in the Inspection and Audit Manual. In the December 2005 risk assessment, TCCA acknowledged that current audit procedures did not always capture safety issues, did not identify complex organizational issues affecting safety, were too focused on administrative aspects, and do not help assess proper management of certificate holders.
As early as the March 2005 operational inspection, PNR managers and inspectors were aware of deficiencies in TWA's management of its flight operations. Additionally, the January 2006 regulatory conformance audit made findings formally identifying deficiencies in the company's operational control of its flight operations.
However, the audit findings were based on aspects of regulatory compliance that could be easily verified with documents. The TSB investigation identified supervisory deficiencies within TWA that included repeated absence of the DFO, management workload, span of control, location of managers, absence of in-flight compliance monitoring, inability to effectively investigate, and dispatch of flights under IFR to aerodromes with no valid altimeter setting.
All or most of these deficiencies likely existed at the time of the 2006 audit. Because none of these deficiencies were identified during the audit, the extent of the flight operations management deficiencies at TWA was not fully appreciated by PNR management. Reasons why the audit did not detect these deficiencies likely include the limitations of the prevailing audit/inspection oversight system as defined by TCCA in the December 2005 national audit program (NAP) risk assessment.
Although TC safety oversight processes identified the existence of supervisory deficiencies within TWA, the extent of the deficiencies was not fully appreciated by PNR managers because of the limitations of the prevailing inspection/audit oversight system.
2.19 Audit Follow-up and Tracking
The normal use of a signature space on a form is to attest to the accuracy of the data entered. However, in the case of the audit finding corrective action form, the signature line was specifically intended to indicate that the audit finding was being closed rather than attesting to the accuracy of the information. The fact that a memorandum was sent with the corrective action forms with instructions for completing the forms is indicative of previous problems with the forms.
The principal operations inspector (POI) indicated that on-site follow-up was required on the corrective action forms for findings FO-05-01 and FO-06-01. Contradicting this information, the POI also signed the forms, indicating that the findings were closed.
It is likely that the POI signed the form out of habit, following the convention applied in most forms, to attest to the accuracy of the data provided. It is likely that the design of the form, specifically the meaning of the signature, led the POI to make this error.
The data from the form was then entered into the National Aviation Company Information System (NACIS) database, with the signature indicating that the finding was closed taking precedence over the requirement for on-site follow-up. As a consequence, the audit was closed when follow-up action was not yet complete.
There is a usability problem with the audit corrective action form that led to inaccurate information in the NACIS regarding finding follow-up for the 2006 TWA audit. Because this form is widely used, similar data entry errors are likely to exist within the database, undermining the effectiveness of the NACIS as a management tool.
Many data errors existed in the NACIS information regarding the audit findings for the January 2006 TWA combined audit, with accurate information recorded for only 21 of the 45 findings. Database records for the other 24 findings contained incorrect information regarding either the requirement for follow-up or the type of follow-up required. Two of these, FO-05-01 and FO-06-01, identified follow-up as complete when it was not. It is likely that NACIS information for other audits includes inaccurate information regarding whether follow-up is required or the type of follow-up required, reducing the effectiveness of the NACIS as TCCA's primary management audit tracking system.
2.20 Pilot Proficiency Checks
Regulations require air taxi pilots to successfully complete a pilot proficiency or competency check for the type of aircraft to be flown before acting as a flight crew member. Both pilots involved in this occurrence passed their respective flight tests, and both held current proficiency or competency certifications.
Because TWA employed approved check pilots (ACPs), TCCA was required to conduct 15 per cent of the required pilot proficiency checks (PPCs) for the company's pilots. During the 12-month periods from September 2002 to September 2003 and from 07 January 2006 to 07 January 2007, the required proportion of PPCs was carried out by TC inspectors.
The TCCA policy of transferring pilot checking responsibilities from TC inspectors to ACPs was intended to reduce the amount of time TC inspectors spent conducting PPCs in favour of more critical auditing and surveillance functions, and Commercial and Business Aviation Advisory Circular (CBAAC) 0176R2 indicated that "air operators can anticipate increased oversight activity in areas other than PPCs." It is possible that TC inspector resources were reallocated to oversight of other companies. However, the investigation revealed no information indicating that surveillance of TWA by TC had increased as a result of the decreased number of PPCs conducted by TC inspectors.
2.21 Pilot Self-Dispatch Systems and Decision Support Tools
Registered aerodromes are not certified as airports and are not built, maintained, or operated to the same standards as certified airports. Many registered aerodromes present threats that must be managed effectively to reduce risk to acceptable levels. In the case of Sandy Bay, the threats for the occurrence flight were a short runway, limited visual cues for approach and landing at night, and unknown weather and runway conditions. Because of such threats, the CARs do not permit scheduled commercial passenger air service at uncertified aerodromes unless a hazard identification and risk mitigation process is conducted.
Although TWA did not operate scheduled service to Sandy Bay or other uncertified aerodromes, unscheduled service occurred frequently. TW350 was one of many unscheduled flights the company's King Air crews made to Sandy Bay and other uncertified aerodromes. Such repetitive unscheduled service does not require hazard identification or risk mitigation before the use of uncertified aerodromes. Consequently, the probability of an unscheduled flight encountering undefended risks is higher than that for scheduled flights.
Pilot self-dispatch is commonly used in commercial air operations, as is the case with TWA. This places greater responsibility for decision making with the pilot-in-command (PIC).
TWA provided risk management in the form of extensive operational guidance in the FOM and SOPs regarding the decisions captains were expected to make, and required crew members to monitor each other's performance and to identify any deviation or omission. However, the company's pilot self-dispatch system relied totally on pilots' knowledge of and compliance with regulatory and company requirements.
Company policy guidance on how to cope with threats was general in nature and not linked with specific aerodromes. Additionally, the company did not provide, and was not required to provide, pilot self-dispatch decision support tools such as pre-flight planning checklists to assist pilots in verifying that they had complied with regulatory or company requirements.
Decision support tools were widely available. Although they were not used in hiring the captain, TWA had checklists for interviewing prospective pilots. TC auditors used audit finding forms. The POI used corrective action forms. PNR managers used the NACIS to support decision making. Senior TCCA managers used the July 2005 and December 2005 risk assessments in support of decisions to adjust regulatory oversight workload and activities.
However, when it came to pre-flight risk management, the crew of TW350 and other TWA King Air pilots did not have an easily usable tool, such as the example in Appendix B, to assist them in their decision making. Instead, they were expected to comply with a myriad of regulatory and operational requirements put in place to manage risk to an acceptable level and contained in documents such as the CARs, the FOM, and the SOPs that are better suited to reference in an office rather than an aircraft cockpit.
The availability of adequate decision support tools may not have made a difference in the flight of TW350. However, such tools could have improved pilot self-dispatch risk management in other flights operated by TWA that were crewed by other pilots who also deviated from regulatory and company risk management requirements.
Under the self-dispatch system, as part of being responsible for all decision making, flight crews were also responsible for all hazard identification and risk management. In the case of TW350, the pilot self-dispatch system failed because the crew did not comply with the company and regulatory risk management requirements and company operational control did not ensure crew compliance.
Self-dispatch systems rely on correct assessment of operational hazards by pilots, particularly in the case of unscheduled commercial service into uncertified aerodromes. Unless pilots are provided with adequate decision support tools, flights may be dispatched with defences that are less than adequate.
2.22 Company Safety Management System Implementation
TWA's existing management system already incorporated roles and responsibilities, documentation, and processes for managing safety. The company was implementing a formally documented SMS as required for its CAR 705 airline operations. The investigation examined SMS implementation at TWA; however, the scope of the investigation did not include SMS certification oversight activities conducted by TCCA.
At the time of the occurrence, the company was in phase 2 of SMS implementation, which meant that it was putting in place reactive processes. The company did not have a fully functioning SMS and was not required to have one until 30 September 2008.
The NCP was aware of previous problems with the captain and first officer and had conducted two informal investigations following a report from each pilot. However, the company's SMS did not yet have a functioning reporting system, did not receive either of these reports, and was not used in either of these investigations in any manner.
Additionally, the crew pairing was only one of many underlying factors that the TSB investigation identified as contributing to the accident. Other factors also contributed to this accident and were not detected either by the company's immature SMS or the company's traditional management processes. Some of these factors are as follows: ineffective operational control by company management (section 2.16), deficiencies in supervisory activities that permitted the undetected development and persistence of substantial and widespread deviations from SOPs (section 2.14.1), no assessment of aircraft performance was conducted by the crew or by any other King Air crew employed by the company (section 2.7), non-standard phraseology employed by the crew members (section 2.9), and a discrepancy in the SOPs regarding flap selection during go-around (section 2.11).
As discussed in section 1.17.1.15, TWA's SMS investigation of the Fort McMurray incident identified the incident as a non-conformance with CAR 602.104(2) and concluded that the cause of the incident was lack of situational awareness. However, as discussed in section 2.14.1, poor situational awareness is not an underlying factor, but rather a symptom of deeper problems. In this case, the deeper problem was deficiencies in supervisory activities that permitted the undetected development and persistence of substantial and widespread deviations from SOPs. The SMS analysis did not identify this serious issue.
Additionally, the company had identified other hazards that either presented risk or contributed to this occurrence, but the analysis of these hazards was general in nature, resulting in mitigating action that did not effectively reduce the risk associated with the hazards. Some of these hazards are black hole aerodromes existing in the company's area of operations (TWA SD06-13 discussed in section 1.17.1.17), and altimeter errors resulting from below standard temperatures (section 2.14.2).
TWA's SMS did not detect earlier reports to the NCP by the TW350 captain and first officer. However, it did detect the Fort McMurray incident, enabling the use of SMS to investigate, analyze, and initiate corrective action. Therefore, at the time of the occurrence, the SMS was working at a basic level.
The requirement for line checks was part of the corrective action plan recommended by the SMS investigation of the Fort McMurray incident. Execution of this portion of the corrective action plan required scheduling and conducting the line checks. However, as discussed in section 2.14.1, the line check was not immediately conducted after the suspensions and was not scheduled for January 2007. The execution of the plan was not conducted in a timely manner. One reason is that, as stated in section 1.17.1.8, company managers had no formal guidance in the FOM or FCTM as to the frequency at which line checks were to be conducted or the criteria governing when they would be conducted. Consequently, line checks were rarely done at TWA.
The TWA SMS investigation finding was that the Fort McMurray incident was a non-conformance with CAR 602.104(2). TSB investigators conducted a review of TCCA Civil Aviation Daily Occurrence Reporting System (CADORS) information and determined that, during the 740-day period before the Fort McMurray incident, from 04 November 2004 to 23 November 2006, TWA had 13 occurrences recorded in CADORS for alleged CAR infractions.
During the 740-day period after the Fort McMurray incident, from 25 November 2006 to 04 December 2008, TWA had 17 occurrences recorded in CADORS for alleged CAR infractions. The corrective action taken as a result of the TWA SMS investigation of the Fort McMurray incident did not reduce the number of regulatory non-compliance occurrences involving TWA. To the contrary, the number of regulatory non-compliance occurrences actually increased.
Additionally, as discussed in section 2.15, the part of the corrective action plan that was implemented—disciplinary action—was not effective and did not, by itself, mitigate the hazard posed by the crew's non-compliance with regulations.
The investigation reviewed publication TP 14235B, Civil Aviation Implementation Plan, Safety Management Systems (Revised 04/2005), regarding TCCA expectations for progressive SMS development as a certificate holder. This plan indicates that, at the completion of phase 2 of SMS implementation, certificate holders must demonstrate that their system includes a process for occurrence reporting with a risk management process. The plan indicates that, at the completion of phase 3 of SMS implementation, a certificate holder must demonstrate the addition of a process for the proactive identification of hazards and a risk management process. At the time of the occurrence, TWA's SMS had not yet completed phase 2 of implementation.
Therefore, TWA's SMS was not yet capable or expected to be capable of detecting, analyzing, and mitigating the risks presented by the hazards underlying this occurrence.
3.0 Conclusions
3.1 Findings as to Causes and Contributing Factors
-
The crew was unable to work effectively as a team to avoid, trap, or mitigate errors and safely manage the risks associated with flight TW350.
-
Transwest Air (TWA) managers had identified and addressed some crew pairing issues with respect to this crew, but were unaware of the degree to which these factors could impair their effective crew coordination.
-
The crew's lack of coordination was, in part, because they had not received recent crew resource management (CRM) training.
-
Contrary to company policy, the approach to Sandy Bay, Saskatchewan, was flown by the less experienced crew member.
-
The crew members did not assess the aircraft performance and did not identify runway length as a threat. Consequently, they did not discuss and agree on a point at which a safe landing was no longer possible and were unprepared to make and execute a timely go-around decision.
-
The first officer suggested a go-around at an appropriate time. However, inadequate preparation and coordination by the crew members resulted in the captain rejecting this suggestion and they continued the approach past the point at which the aircraft could be safely stopped on the runway.
-
The captain decided to initiate a go-around, but his communication of this decision to the first officer was non-standard and did not have the desired effect of triggering the correct sequence of go-around actions required.
-
The captain very likely took control of the aircraft from the first officer using the non-standard transfer of control practice the crew had developed, thereby causing confusion, which further eroded the limited opportunity to achieve a positive climb.
-
The discrepancy in the standard operating procedures (SOPs) describing the selection of flaps during go-around likely led to both pilots independently operating the flap control lever, distracting them from monitoring the climb performance during the go-around.
-
It is likely that a somatogravic illusion caused the pilot flying (PF) to lower the nose of the aircraft. Consequently, the aircraft did not maintain a positive rate of climb and collided with the trees.
-
Deficiencies in TWA's supervisory activities permitted the undetected development and persistence of substantial and widespread deviations from SOPs within the King Air operation.
-
The company management structure and workload, combined with the location of managers away from the remote bases of operations, reduced the effectiveness of operational control.
3.2 Findings as to Risk
-
Some Canadian Air Regulations (CARs) subpart 703 air taxi and subpart 704 commuter operators are unlikely to provide initial or recurrent CRM training to pilots in the absence of a regulatory requirement to do so. Consequently, these commercial pilots may be unprepared to avoid, trap, or mitigate crew errors encountered during flight.
-
Transport Canada (TC) Prairie and Northern Region (PNR) management practices regarding the June 2006 replacement of the regional combined audit program, in order to manage safety management system (SMS) workload, did not conform to TC's risk management decision-making policies. Reallocation of resources without assessment of risk could result in undetected regulatory non-compliance.
-
Although TC safety oversight processes identified the existence of supervisory deficiencies within TWA, the extent of the deficiencies was not fully appreciated by the PNR managers because of the limitations of the oversight system in place at that time.
-
It is likely that the National Aviation Company Information System (NACIS) records for other audits include inaccurate information resulting from data entry errors and wide use of the problematic audit tracking form, reducing the effectiveness of the NACIS as a management tracking system.
-
Self-dispatch systems rely on correct assessment of operational hazards by pilots, particularly in the case of unscheduled commercial service into uncertified aerodromes. Unless pilots are provided with adequate decision support tools, flights may be dispatched with defences that are less than adequate.
-
TWA King Air crews did not use any standard practice in applying cold temperature altitude corrections. Inconsistent application of temperature corrections by flight crews can result in reduction of obstacle clearance to less than the minimum required and reduced safety margins.
-
The practice of not visually verifying wind/runway conditions at aerodromes where this information is otherwise unavailable increases the risk of post-touchdown problems.
-
The company dispatched flights to Sandy Bay without a standard means for crews to deal with non-current altimeter settings. Use of non-current or inappropriate altimeter settings can reduce minimum obstacle clearance and safety margins.
-
The crew was likely unaware of their ¼ nautical mile (nm) error in the aircraft position in relation to the runway threshold resulting from use of the global positioning system (GPS). Unauthorized and informal use of the GPS by untrained crews during instrument flight rules (IFR) approaches can introduce rather than mitigate risk.
-
Widespread adaptations by the King Air pilots resulted in significant deviations from the company's SOPs, notwithstanding the company's disciplinary policy.
-
In a SMS environment, inappropriate use of punitive actions can result in a decrease in the number of hazards and occurrences reported, thereby reducing effectiveness of the SMS.
-
Aerodromes with limited visual cues and navigational aids are not explicitly identified in flight information publications as hazardous for night/IFR approaches. Passengers and crews will continue to be exposed to this hazard unless aircraft and aerodrome operators carry out risk assessments to identify them and take mitigating action.
-
Aerodromes with limited visual cues and navigational aids are not explicitly identified in flight information publications as hazardous for night/IFR approaches. Passengers and crews will continue to be exposed to this hazard unless aircraft and aerodrome operators carry out risk assessments to identify them and take mitigating action.
-
To properly assess applicants for pilot positions, operators need access to information on experience and performance that is factual, objective, and (preferably) standardized. Because some employers are unprepared to provide this information—fearing legal action—this may lead to the appointment of pilots to positions for which they are unsuited, thereby compromising safety.
3.3 Other Findings
-
TWA's safety management system was not yet capable or expected to be capable of detecting, analyzing, and mitigating the risks presented by the hazards underlying this occurrence.
-
The first officer and captain met competency standards on the completion of their initial flight training before they began employment as line pilots.
-
It is very likely that the captain became the pilot flying for the remaining 20 seconds of the flight. The scenario that neither pilot was controlling the aircraft at that time is considered very unlikely.
4.0 Safety Action
4.1 Action Taken
4.1.1 Transwest Air
On 18 January 2007, the Director of Flight Operations (DFO) of Transwest Air (TWA) issued operations directive OD07-01 entitled First Officer Take-off and Landing Limitations. The directive was addressed to all company pilots and disseminated company policy that "the captain will fly the first leg of the flight for a crew pairing—no exceptions." The directive also provided specific criteria governing when captains were required to fly take-offs or landings, including landing when the landing distance available is less than 3500 feet.
All pilots of multi-engine aircraft have received initial crew resource management (CRM) and pilot decision-making training. Recurrent training will take place on a yearly basis.
All pilots of multi-engine aircraft have completed a line check and will continue to undergo yearly line checks in the future.
Since the accident on 07 January 2007, any safety concerns brought forward are processed using the safety management system (SMS) and are assessed for risk and a corrective action plan is implemented. The accountable executive is kept informed of any non-standard situations.
In the spring of 2007, Transport Canada (TC) conducted an on-site validation that the components and elements required for phase 2 implementation of TWA's SMS were in place and functioning as indicated in the company documentation. An acceptance letter was sent to TWA on 06 July 2007.
Early in 2008, TC conducted an on-site validation that the components and elements required for phase 3 implementation of TWA's SMS were in place and functioning as indicated in the company documentation. An acceptance letter was sent to TWA on 06 March 2008.
TWA is currently undergoing phase 4 of SMS implementation. The phase 4 completion milestone is now 30 November 2009, when a SMS assessment is to confirm whether the certificate holders have the required elements in place to demonstrate compliance with the Canadian Aviation Regulations (CARs).
Standard operating procedures (SOPs) have been amended and standardized for all aircraft types to include, among other things, first officer take-off and landing limitations, the black hole effect, stabilized approaches, and pilot-monitored approaches.
Additionally, the Beech A100 King Air SOPs have been amended to reconcile the text description of the missed approach procedure with the procedure specified in the flight profile diagrams.
Copies of operational flight plans (OFPs) left behind at main base departure aerodromes are added to the paperwork to be filed at the end of each day. Base dispatchers are responsible for filing and auditing these OFPs on a daily basis. Completed OFPs from northern bases are faxed to the northern chief pilot (NCP) and the DFO at the end of every day for quality assurance purposes. Flight operations management is located in Saskatoon, Saskatchewan, and is able to audit the OFPs at that base at its discretion.
Cold temperature altitude corrections are discussed at pilot meetings held each fall. TWA has incorporated the cold temperature altitude correction procedures into its SOPs for all aircraft.
4.1.2 Saskatchewan Government Department of Highways and Transportation
The obstacle limitation surface (OLS) is a standard that applies to certified airports and is not applicable at Sandy Bay, Saskatchewan. However, the Department (now the Ministry of Highways and Infrastructure) has generally followed certification standards at Sandy Bay in regard to the OLS, lighting, and other physical characteristics.
The Manager of Airport and Marine Operations conducted an inspection of the Sandy Bay aerodrome on 25 July 2007 to identify short- and long-term capital improvement projects. The inspection resulted in the removal of trees penetrating the OLS on approach to Runway 05. This work was completed on 25 January 2008. The Ministry removed considerably more trees than required to meet OLS requirements.
A capital project to lengthen the runway to 3900 feet has been initiated. The first stage includes cost estimates and prioritization with other capital projects. Completion will depend on approval, funding, and priorities.
In 2008, the Ministry researched the possibility of installing a precision approach path indicator (PAPI) system at Sandy Bay. The Ministry had never installed PAPI systems on runways shorter than 3800 feet due to the ground point of interception (GPI) possibly being too far down the runway to allow for safe landings. It was determined, however, that there are a number of Canadian airports shorter than Sandy Bay that have PAPI systems. In 2008, Ministry consultations with operators and TC indicated that a PAPI system at Sandy Bay would be beneficial.
The Ministry purchased and installed a PAPI system at Sandy Bay aerodrome in 2008, with the system put into service on 03 October 2008.
4.1.3 NAV CANADA
After the accident, NAV CANADA conducted a review of flight information publications. The review determined that the minimum descent altitude (MDA) height above touchdown zone elevation (HAT) published in the Restricted Canada Air Pilot (RCAP) non-directional beacon (NDB) 05 instrument approach procedure for Sandy Bay was incorrectly depicted as 799 feet, while the correct HAT was 779 feet. NAV CANADA immediately distributed the correct information by a NOTAM (notice to airmen) and published the correct HAT in the next edition of the RCAP instrument approach procedure.
4.1.4 Transport Canada
TC forecasts that draft regulations will be published in Part I of the Canada Gazette in December 2009 requiring CAR 703 and 704 operators to implement safety management systems (SMS) in accordance with a phased schedule. Adoption of an effective SMS by these operators should significantly mitigate the types of management and operational issues identified in this report.
4.2 Action Required
4.2.1 Crew Resource Management Training
Following TC's response to TSB Recommendation A95-11 issued in 1995, CRM training is now required for CAR 705 airline operations. However, it is not required for CAR 704 commuter and CAR 703 air taxi operations and, for this reason, TC's response to TSB Recommendation A95-11 was assessed by the TSB as Satisfactory in Part. CAR 703 air taxi and CAR 704 commuter categories are assigned by TC based on number of seats and weight of aircraft, and do not take into account the complexity of an aircraft or the crew coordination required to operate it.
Ineffective CRM contributed to this accident and presented risk on other King Air flights operated by TWA. It is likely that recent CRM training would have assisted the crew of TW350 and TWA's other King Air pilots in managing risks present during flight to an acceptable level. As discussed in section 1.18.1, ineffective CRM also contributed to other occurrences investigated by the TSB (see Appendix G).
Many Canadians depend on air taxi and commuter operators for transportation, especially in isolated and less-developed areas of the country where surface transportation is difficult or impossible. The Canadian air taxi and commuter fleet includes a wide variety and a large number of complex multi-engine aircraft operated by two pilots using SOPs for operational crew coordination guidance and with a requirement for levels of crew coordination comparable to that required for the CAR 705 airline category aircraft. These aircraft are operated around the clock across Canada. Such aircraft require pilots with effective CRM skills to operate the aircraft safely and efficiently.
CAR 705 airline operations typically operate with a dispatch system in place to support flight crew planning and decision making, whereas most CAR 703 and 704 operations operate under the pilot self-dispatch system discussed in sections 1.17.1.4 and 2.21. CAR 703 air taxi flight crews are employed at the industry entry level, often with little or no previous commercial aviation experience. Operations are commonly conducted in uncontrolled airspace with little assistance from air traffic services (ATS). Additionally, CAR 703 and 704 operations more frequently involve aerodromes with limited support infrastructure and services as compared to those aerodromes and airports used by CAR 705 airline operators.
Many air taxi and commuter operators provide their pilots with CRM training voluntarily, although there is currently no regulatory requirement for them do so. However, some CAR 703 air taxi and CAR 704 commuter operators do not provide their pilots with any initial or recurrent CRM training, and others do not provide recurrent CRM training on an annual basis.
The investigation concludes that some operators are unlikely to provide training in the absence of a regulatory requirement to do so. Therefore, some commercial pilots may be unprepared to avoid, trap, or mitigate crew errors encountered during flight.
CRM training has developed over the years as an effective tool. Modern, well-designed CRM training now includes such things as the concept of threat and error management (TEM). This accident has demonstrated that current defences are less than adequate. In light of the risks associated with the absence of recent CRM training for air taxi and commuter crew members, the Board recommends that:
The Department of Transport require commercial air operators to provide contemporary crew resource management (CRM) training for Canadian Aviation Regulations (CARs) subpart 703 air taxi and CARs subpart 704 commuter pilots.
Transportation Safety Recommendation A09-02
4.3 Safety Concerns
4.3.1 Absence of Adequate Visual Cues
The absence of adequate visual clues leads to the black hole effect and contributes to somatogravic illusions.
The TSB determined that the black hole effect was a causal or contributing factor in occurrences A05O0225 (Piper PA-31), A00A0051 (Astra SPX), A99A0131 (Airbus A320-211), and A90H0002 (Beechcraft 99 Airliner). The TSB has made findings that somatogravic illusion resulting from the absence of adequate visual cues was a contributing factor in occurrences A05O0225 (PA-31), A01C0236 (SA226TC), A00O0111 (Falcon 20E), A99O0126 (MU-2B), A97C0236 (EMB-110P1), A96C0002 (Cessna T210M), A93C0169 (Cessna 310R at Sandy Bay), and A89H0007 (SA 227). These hazards will continue to contribute to future occurrences in the absence of additional mitigating action.
In addition to Sandy Bay, black hole hazards exist at many aerodromes and airports across Canada. Proactive identification and publication of information about aerodromes and airports affected by black hole hazards could substantially mitigate the risk associated with limited visual cues, and is consistent with current risk management and SMS philosophy. Therefore, the Board encourages aircraft and aerodrome operators, flight information providers, and TC to take action to mitigate the hazards of black holes.
Education regarding the hazards presented by the absence of adequate visual cues has been extensive. The Board is concerned, however, that little action has been taken to explicitly identify locations where these hazards exist. Some sectors of the industry will not take action, because they view mitigation of this hazard as the responsibility of others. Leadership by the regulator is required in order to address this issue effectively.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices
Appendix A – Sandy Bay Restricted Canada Air Pilot NDB RWY 05

Appendix B – Pre-Flight Risk Assessment Decision Support Tool Used by a Canadian CAR 703 Commercial Air Operator
Appendix C – Transport Canada Civil Aviation Transition to Safety Management System-based Oversight System
Strategic Planning
In December 1999, Flight 2005 established new safety goals and plans for the next five years. One operating principle identified in Flight 2005 was using risk management techniques and policies in decision making and applying them consistently.
Flight 2005 identified six directions that would evolve and become fully integrated into the Transport Canada Civil Aviation (TCCA) program over the next five years. Three of these directions were described as follows:
-
Resource Allocation – Using a risk-based approach to resource allocation for regulatory activities, emphasis will be placed on developing efficient ways of deploying civil aviation resources to those activities with the greatest safety benefit.
-
Safety Management – Implementing safety management systems (SMS) in aviation organizations to improve safety through proactive management rather than reactive compliance with regulatory requirements. Transport Canada's (TC) role is to provide these organizations with information on the safety management concept and to facilitate its implementation.
-
Human and Organizational Factors – Taking account of human and organizational factors in safety management practices, based on "a growing realization that organizational factors can also create unsafe conditions."
In April 2006, TCCA published an updated strategic plan, Flight 2010. In the foreword, the TCCA Director General, Civil Aviation (DGCA) stated that "aviation has become a business of managing risks" and managing risks would be the main focus of the strategic plan.
Flight 2010 states TCCA's mission as follows: "To develop and administer policies and regulations for the safest civil aviation system for Canada and Canadians using a systems approach to managing risks," and identifies goals and objectives as priorities over the next five years, including:
-
Implement SMSs as the cornerstone of the aviation community's business operations.
-
Assist the aviation community's transition to SMSs.
-
Re-align all interrelated activities necessary to manage and conduct the civil aviation program within the context of SMS.
-
Strengthen risk-based approach for all decision making, including resource allocation/reallocation for program activities to achieve responsible spending and results – This objective is presented "under the assumption that no additional resources will be available for the civil aviation program, it has to adjust activities by ceasing or reducing lower-priority items to fund higher-priority safety issues and Government of Canada agenda items."
Flight 2010 closes with a brief discussion of the period following 2010:
The aviation industry will have implemented robust safety management systems (SMS) in which the public and regulator have confidence. As companies evolve from compliance to safety risk management thinking, regulators will transform from regulatory compliance auditors into system evaluators, as the underlying philosophy shifts the onus for proving or disproving adequate safety performance from the regulator to the organization. Well designed and executed risk management systems and risk-based oversight programs will have laid the groundwork for this to happen, while achieving safer skies.
Safety Management Systems
The fundamental aim of SMS is to improve safety through proactive management rather than reactive compliance with regulatory requirements. A SMS is a systematic approach for managing risk that integrates operations and technical systems with the management of financial and human resources to ensure aviation safety or the safety of the public. In Canada, a SMS is expected to include:
-
a safety policy on which the system is based;
-
a document containing all SMS processes and a process for making personnel aware of their responsibilities with respect to them;
-
a process for setting goals for the improvement of aviation safety and for measuring the attainment of those goals;
-
a process for identifying hazards to aviation safety and for evaluating and managing the associated risks;
-
a process for ensuring that personnel are trained and competent to perform their duties;
-
a process for the internal reporting and analyzing of hazards, incidents, and accidents and for taking corrective actions to prevent their recurrence; and
-
a process for conducting periodic reviews or audits of the SMS and reviews or audits for cause of the SMS.
A SMS is intended to become integrated into the functioning of an organization such that the SMS processes become part of the organizational culture and the way people do their jobs. SMS implementation is intended to promote development of a safety culture within an organization, eventually helping it reach a mature state as a generative safety culture. Footnote 43
Under the SMS concept, operators will learn to act proactively by considering factors that might be hazards that could lead to incidents, selecting appropriate mitigation strategies, and putting them in place before an incident occurs. It is expected that, if a SMS is properly implemented, the risk of accidents with contributing organizational and human performance issues will be reduced.
Although SMS is relatively new to the Canadian aviation industry, there are already examples of established SMS programs with documented improvements in safety performance and cost reductions due to reduced incident rates to show that SMS can result in safety as well as financial benefits.
Implementation of Safety Management System-based Oversight System
TCCA policy regarding the implementation of SMS was articulated in Civil Aviation Directive 31 (CAD 31). TCCA is one of the first civil aviation regulators in the world to move to a SMS-based approach to oversight.
This policy applies to all areas of the national civil aviation program and outlines TCCA's approach to the implementation of SMS in aviation organizations. CAD 31 describes the approach as involving "progressive development" with implementation comprising four phases extending over 3 years and 120 days. CAD 31 briefly describes the roles and responsibilities of managers and committees involved in SMS implementation and states that "Civil Aviation is committed to and supports the implementation of safety management systems in aviation organizations."
As of July 2009, TCCA is forecasting that regulations requiring implementation of SMS within CAR 703 air taxi and CAR 704 commuter operators will be published in the Canada Gazette in December 2009 Footnote 44 and are planned to come into force in February 2010. These commercial operators would then develop their SMS over the following three years using the four-phase implementation program described in section 1.17.1.14.
Transwest Air (TWA) was in the midst of implementing its SMS and TC had previously been conducting its regulatory oversight of the company using an inspection/audit approach. TC was making a transition to SMS-based oversight of the company and TWA was scheduled for a phase 2 SMS implementation assessment by the Prairie and Northern Region (PNR) in April 2007. Because of this shift in oversight methodology, the TSB investigation examined, in general, TCCA implementation of CAD 31, "Safety Management Systems," and the transition from inspection/audit oversight to SMS-based oversight.
A considerable amount of change is required of both TCCA and industry in the transition from traditional audit/inspection oversight to SMS-based oversight. TCCA has adopted an iterative, phased implementation approach to allow both TCCA and industry to adapt and develop appropriate policies, procedures, and practices. For example, the learning obtained from the CAR 705 airline SMS implementation iteration currently underway is intended to be used to further develop the SMS program for implementation in a future iteration in CAR 703 air taxi and CAR 704 commuter operations.
A steering committee comprised of all TCCA Headquarters directors manages the development of processes, procedures, and practices related to SMS rulemaking and regulatory oversight. This involves the establishment of committees to obtain regular feedback from TCCA regions on the progress of SMS implementation, adapting procedures and practices based on this feedback, as well as implementation of quality assurance controls and a functional learning committee.
TC Headquarters provided classroom training to front-line TCCA managers and inspectors on SMS and on the transition from traditional audit/inspection oversight to SMS assessment. Online refresher training was also provided. Senior managers were provided with change management training.
SMS implementation guidance material developed by TCCA included a guide with detailed procedures to be followed by certificate holder organizations to assist with the implementation of their SMS using a phased approach. Staff instructions provided policy and procedural guidance for front-line TCCA managers and inspectors directly responsible for overseeing implementation of SMS by certificate holders.
TCCA used its experience in working on implementation activities with multiple stakeholders to determine the appropriate length of time for implementation. This experience highlighted that a SMS cannot be implemented instantaneously; time and continuous improvement is required to build an effective SMS.
TCCA uses a systematic approach to communication and has had a communication strategy for SMS in place since 2004. The strategy is a high-level document that continues to guide SMS communications efforts internally and with industry stakeholders.
Each region conducts its own risk assessment in relation to SMS and non-SMS organizations and the transition of oversight activities from audits to program validations.
In taking an iterative phased approach to implementation, risks associated with the program can be mitigated by applying the lessons learned from the relatively small number of CAR 705 airline operators who moved to SMS in the first phase to the much larger number of CAR 703 air taxi and CAR 704 commuter operators that will implement SMS in the later stages of the program. The iterative phased approach provides opportunities for skill and process development within TCCA, as well as opportunities to modify timelines and regulatory requirements as the program develops. Additionally, functional activities such as quality assurance and the functional learning committee are in place to gather feedback about implementation.
Appendix D – Two Examples of Transport Canada Civil Aviation Risk Assessments
As discussed in section 1.17.2.2, the investigation examined two examples of the application of Transport Canada Civil Aviation (TCCA) risk management policies and procedures.
July 2005 – Prairie and Northern Regional Risk Assessment of Proposed Audit Deferral
The first example of risk management application occurred in July 2005. A risk assessment was conducted by Transport Canada (TC) Prairie and Northern Region (PNR) to assess the risk of deferring the four air operator certificate (AOC) holders remaining on the regional combined audit schedule, as of June 2005, including Transwest Air (TWA). The risk assessment was conducted by a team of operations and maintenance inspectors responsible for oversight of the four companies. The team was responsible for conducting the risk assessment and recommending a risk control option, but did not have authority to assign resources to risk control activities.
The risk assessment summary included a hazard statement that states "Reallocation of combined audit resources may result in undetected non-compliance, which in turn erodes the regulatory compliance defence barrier for the prevention of aviation loss." The risk assessment produced a recommended risk control option that proposed, in part, to reduce the scope of the TWA audit from a combined audit to a maintenance specialty audit and to defer it until 01 February 2006, to defer the combined audits of the second and third companies, and to conduct the combined audit of the fourth company as scheduled. Other recommended action pertaining to TWA was to conduct inspections and specialty audits focused on technical dispatch, to conduct a detailed Civil Aviation Daily Occurrence Reporting System (CADORS) review, and to establish alert levels. Section 5.1 of the risk assessment described an implementation plan for TWA risk control activities, including enhanced surveillance of the company by the primary inspectors and a briefing for company management.
The recommended risk control option was accepted by the Regional Director, Civil Aviation (RDCA) on 09 August 2005, with an instruction to perform the risk assessment again in January 2006. Subsequently, the principal operations inspector (POI) for TWA was advised that the TWA Director of Flight Operations (DFO) would be on sick leave for 90 days (see section 1.17.1.9). The POI immediately advised the risk assessment team leader of the DFO's absence and a possible effect on the risk assessment factors and the decision to reduce the size of the audit. The risk assessment and risk control option were reviewed by PNR management staff at a meeting in early September 2005. Staff decided that the TWA audit would not be deferred and that executing the risk control plan for TWA was not necessary because the audit would not be deferred. On 16 September 2005, the PNR regional audit coordinator advised PNR managers of Commercial and Business Aviation (CBA) and Maintenance and Manufacturing that the TWA audit would occur as originally scheduled from 12 to 27 January 2006, that the audits of the second and third companies would be deferred, and that the audit of the fourth company would not be deferred.
December 2005 – Transport Canada Civil Aviation Headquarters Risk Assessment of Proposed Reduction of Regulatory Audits
The second example of risk management application occurred in December 2005. TCCA Headquarters conducted a risk assessment to consider what risks are involved in a reduction of regulatory audit activity during the implementation of safety management systems (SMS) over the next five years (2005 to 2010). The risk assessment was conducted by a team representing civil aviation branches and was facilitated by the Manager, Safety Evaluations and Standards. The risk assessment noted that "during SMS implementation, it may be difficult to maintain the audit schedule mandated by the Frequency of Inspection Policy Document and our international agreements." The risk assessment reviewed the possible costs and benefits to TC and concluded that reduction of the national audit program (NAP) during SMS implementation could have the benefits of freeing up to 25 staff and reducing audit related overtime and travel costs by up to $1.5 million.
In a discussion of audit procedures, the risk assessment identified the following problems with current audit procedures: current procedures are too focused on administrative aspects and do not help assess the proper management of certificate holders, current procedures do not always capture safety issues, current audits are very wide, but in some situations are not as deep as necessary, and the underlying issues that have direct effects on the safety of complex organizations are not being identified during these audits.
The risk assessment included a recommended risk control option that proposed, in part, to establish a focused inspection program to conduct risk-based inspections of NAP certificate holders. Also included was a recommendation to extend the focused inspection program to include all certificate holders implementing SMS.
The recommended risk control option was conditionally accepted by the Director General, Civil Aviation (DGCA) on 06 March 2006. The DGCA indicated that changes to technical or bilateral agreements must be successfully negotiated before any changes to the current oversight regime occur. A second condition imposed was that "The additional mitigation requiring the extension of the focused inspection program to include all certificate holders implementing SMS is not accepted. The extent and type of oversight during transition is the purview of the accountable TC manager/executive who will make these decisions based on a case-by-case risk assessment." On 09 March 2006, the DGCA advised National Civil Aviation Management Executive (NCAMX) members of the conditional acceptance of the risk assessment and instructed the Director of Standards to conduct an orderly shut down of the NAP and implementation of mitigations accepted in the risk assessment.
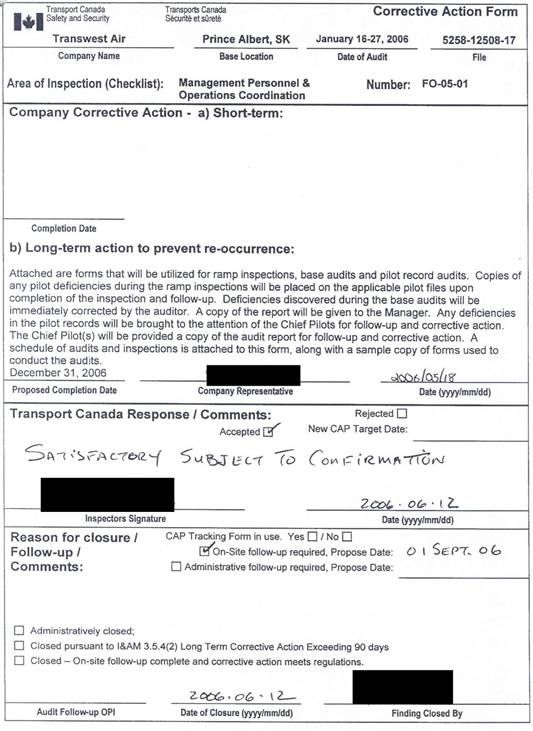
Appendix F – Comparison of Audit Follow-up Information
| Finding # | Correction Action Form | NACIS | ||||||
|---|---|---|---|---|---|---|---|---|
| Follow-Up Required |
Follow-Up Type |
Proposed Follow-Up Date |
Follow-Up Completed |
Date of Closure |
Follow-Up Required |
Follow-Up Type |
Date Completed |
|
| AMO-02-01 | Yes | Admin | 30-May-06 | Yes | 30-May-06 | Yes | Admin | 30-May-06 |
| AMO-05-01 | No | 26-Apr-06 | Yes | Admin | 26-Apr-06 | |||
| AMO-06-01 | Yes | Admin | 30-May-06 | Yes | 30-May-06 | Yes | Admin | 30-May-06 |
| AMO-06-02 | Yes | Admin | 30-May-06 | Yes | 30-May-06 | Yes | Admin | 30-May-06 |
| AMO-06-03 | Yes | Admin | 30-May-06 | Yes | 30-May-06 | Yes | Admin | 30-May-06 |
| AMO-08-01 | Yes | On-Site | 31-May-06 | Yes | 31-May-06 | Yes | Admin | 31-May-06 |
| AMO-08-02 | No | 26-Apr-06 | Yes | Admin | 26-Apr-06 | |||
| AMO-08-03 | Yes | On-Site | 31-May-06 | Yes | 01-Jun-06 | Yes | Admin | 01-Jun-06 |
| AMO-08-04 | Yes | On-Site | 31-May-06 | Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AMO-08-05 | Yes | Admin | 30-May-06 | Yes | 30-May-06 | Yes | Admin | 30-May-06 |
| AMO-10-01 | Yes | Admin & On-Site |
30-May-06 and 31-May-06 |
Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AMO-10-02 | Yes | On-Site | 31-May-06 | Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AMO-10-03 | No | 26-Apr-06 | Yes | Admin | 26-Apr-06 | |||
| AMO-11-01 | Yes | Admin & On-Site |
30-May-06 and 31-May-06 |
Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AMO-13-01 | Yes | Admin & On-Site |
30-May-06 and 31-May-06 |
Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AMO-13-02 | Yes | Admin & On-Site |
30-May-06 and 31-May-06 |
Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AMO-13-03 | Yes | Admin & On-Site |
30-May-06 and 31-May-06 |
Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AMO-14-01 | Yes | Admin & On-Site |
30-May-06 and 31-May-06 |
Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AMO-15-01 | Yes | On-Site | 31-May-06 | Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AMO-20-01 | Yes | On-Site | 31-May-06 | Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AOC-02-01 | Yes | Admin | 30-May-06 | Yes | 29-May-06 | Yes | Admin | 29-May-06 |
| AOC-04-01 | Yes | On-Site | 31-May-06 | Yes | 31-May-06 | Yes | On-Site | 31-May-06 |
| AOC-04-02 | Yes | On-Site | 31-May-06 | Yes | 31-May-06 | Yes | On-Site | 31-May-06 |
| AOC-07-01 | Yes | Admin & On-Site |
30-May-06 and 31-May-06 |
Yes | 31-May-06 | Yes | On-Site | 31-May-06 |
| AOC-07-02 | Yes | On-Site | 31-May-06 | Yes | 31-May-06 | Yes | On-Site | 31-May-06 |
| AOC-10-01 | Yes | On-Site | 31-May-06 | Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AOC-10-02 | Yes | On-Site | 31-May-06 | Yes | 01-Jun-06 | Yes | On-Site | 01-Jun-06 |
| AOC-10-03 | Yes | Admin | 30-May-06 | Yes | 30-May-06 | Yes | Admin | 30-May-06 |
| AOC-10-04 | Yes | On-Site | 31-May-06 | Yes | 31-May-06 | Yes | On-Site | 31-May-06 |
| AOC-11-01 | No | 26-Apr-06 | Yes | Admin | 26-Apr-06 | |||
| AOC-12-01 | Yes | On-Site | 31-May-06 | Yes | 31-May-06 | Yes | On-Site | 31-May-06 |
| AOC-13-01 | Yes | On-Site | 31-May-06 | Yes | 31-May-06 | No | 31-May-06 | |
| AOC-15-01 | No | 26-Apr-06 | Yes | Admin | 26-Apr-06 | |||
| AOC-23-01 | Yes | Admin | 30-May-06 | Yes | 30-May-06 | Yes | Admin | 30-May-06 |
| DG-04-01 | Yes | On-Site | Not designated |
Yes | 01-Aug-06 | Yes | On-Site | 14-Jul-06 |
| DG-04-02 | Yes | On-Site | Not designated |
Yes | 01-Aug-06 | Yes | On-Site | 14-Jul-06 |
| FO-03-01 | No | 12-Jun-06 | Yes | Admin | 12-Jun-06 | |||
| FO-03-02 | No | 29-Mar-06 | Yes | Admin | 29-Mar-06 | |||
| FO-05-01 | Yes | On-Site | 01-Sep-06 | No | 12-Jun-06 | Yes | Admin | 12-Jun-06 |
| FO-05-02 | No | 12-Jun-06 | Yes | Admin | 12-Jun-06 | |||
| FO-06-01 | Yes | On-Site | 01-Sep-06 | No | 12-Jun-06 | Yes | Admin | 12-Jun-06 |
| FO-08-01 | No | 12-Jun-06 | Yes | Admin | 12-Jun-06 | |||
| CS-01-01 | No | 06-Apr-06 | Yes | Admin | 06-Apr-06 | |||
| AOHS-B-02-01 | No | 06-Apr-06 | Yes | Admin | 06-Apr-06 | |||
| AOHS-B-02-02 | No | 06-Apr-06 | Yes | Admin | 06-Apr-06 | |||
Appendix G – Other Occurrences with Absence of Crew Resource Management Training
| A04Q0188 | On 01 December 2004, a Beech B300 Super King Air aircraft departed the runway during landing at Saint-Georges, Quebec. There were two crew members and one passenger on board. There were no injuries and the aircraft sustained substantial damage. The TSB investigation concluded that crew errors contributed to this accident. Neither the captain nor the first officer had received any crew resource management (CRM) training. CRM training was not required for this CAR subpart 604 corporate flight. |
| A04O0103 | On 22 April 2004, a Raytheon B300 Super King Air aircraft stalled during an instrument landing system (ILS) approach to Timmins, Ontario, in icing conditions. The crew recovered from the stall, flew a missed approach, and conducted a second approach to a successful landing. There were three crew members and no passengers on board. There were no injuries and the aircraft was not damaged. The TSB investigation concluded that the flight crew did not practice effective CRM during the approach, and that crew errors contributed to this incident. Although the captain and first officer had each received initial CRM training, neither pilot had received any recent CRM training. CRM training was not required for this CAR subpart 604 corporate flight. |
| A99Q0005 | On 04 January 1999, a Beech 1900C flew into the frozen surface of a river while conducting an instrument approach to Saint-Augustin, Quebec. There were two crew members and 10 passengers on board. There were no injuries and the aircraft sustained substantial damage. The TSB investigation concluded that crew errors contributed to this accident. Neither the captain nor the first officer had received any pilot decision-making or CRM training. CRM training was not required for this CAR subpart 704 commuter flight. |
| A96Q0176 | On 23 October 1996, a Swearingen SA226-TC aircraft departed the runway during landing at Puvirnituq, Quebec. There were 2 crew members and 11 passengers on board. One passenger sustained minor injuries and the aircraft sustained substantial damage. The TSB investigation concluded that a lack of communication in the cockpit contributed to this accident. Neither pilot had received any CRM training. CRM training was not required for this CAR subpart 704 commuter flight. |
| A94A0078 | On 14 April 1994, a Swearingen SA226-AT aircraft nearly collided with a building while on final approach at Sydney, Nova Scotia. There were two crew members and no passengers on board. There were no injuries and the aircraft was not damaged. The TSB investigation concluded that crew errors contributed to this incident. Neither pilot had received any CRM training. CRM training was not required for this commuter category flight. |
| A94W0026 | On 08 March 1994, a McDonnell Douglas DC-8-62F aircraft took off from Calgary, Alberta, with two failed tires on the left main landing gear. After take-off, air traffic control (ATC) advised the flight that rubber had been found on the runway, and the flight returned to Calgary for a successful emergency landing. There were 8 crew members and 75 passengers on board. There were no injuries and the aircraft sustained minor damage. The TSB investigation concluded that ineffective crew communications resulting from the lack of CRM training contributed to this incident. CRM training was not required for this airline category flight. |
| A93P0131 | On 21 July 1993, a Convair 580 aircraft ran off the end of the runway while landing at Tofino, British Columbia. There were 4 crew members and 47 passengers on board. There were no injuries and the aircraft sustained substantial damage. The TSB investigation concluded that crew errors and ineffective crew communications contributed to this accident. Neither pilot had received CRM training. CRM training was not required for this airline category flight. To ensure that all operators and aircrew involved in commercial aviation have access to training for better coping with day-to-day operating decisions, the Board recommended that:
|
| A89H0007 | On 26 September 1989, a Fairchild SA227 aircraft crashed at Terrace, British Columbia, while conducting a missed approach. There were two crew members and five passengers on board. All seven occupants were fatally injured and the aircraft was destroyed. The TSB investigation concluded that crew errors contributed to this accident. Neither pilot had received any CRM training. CRM training was not required for this commuter category flight. |
Appendix H – Action Taken in the United States Regarding Standardized Information on the Quality of Pilot Performance
The United States National Transportation Safety Board (NTSB) has been advocating for over 20 years for improvements in the ability of air operators to conduct background checks of pilot applicants.
On 03 November 1988, the NTSB issued a safety recommendation asking the Federal Aviation Administration (FAA) to require commercial operators to conduct substantive background checks of pilot applicants including, in part, examination of training, performance, and other records of previous employers (A-88-141). In responding to this recommendation, the FAA indicated that the agency agreed with the intent of the recommendation. However, such background checks were left to be performed on a voluntary basis because the FAA believed that the costs of promulgating and enforcing such a regulatory change would outweigh the benefits. The NTSB considered the FAA response to be unacceptable and classified Recommendation A-88-141 as "Closed – Unacceptable Action/Superseded."
On 21 November 1990, following a subsequent investigation, the NTSB issued a safety recommendation asking the FAA to require commercial operators to conduct substantive background checks of pilot applicants including, in part, examination of training, performance, and other records of previous employers (A-90-141). The FAA responded in February 1991, stating that the agency did not believe that a requirement for pilot screening was necessary, and that air carriers had been encouraged to make voluntary use of FAA databases to verify the validity of an applicant's history. The NTSB considered the FAA response to be unacceptable and classified Recommendation A-90-141 as "Closed – Unacceptable Action."
On 19 February 1993, following a subsequent investigation, the NTSB issued a safety recommendation asking the FAA to require commercial operators to conduct substantive background checks of pilot applicants, including, in part, examination of training, performance, and other records of previous employers (A-93-14). The FAA response disagreed with the recommendation, and the NTSB classified Recommendation A-93-14 as "Closed – Unacceptable Action."
On 15 November 1995, the NTSB issued four safety recommendations asking the FAA to:
-
Require specified airlines and training establishments to maintain pertinent standardized information on the quality of pilot performance in activities that assess skills, abilities, knowledge, and judgment during training, check flights, initial operating experience, and line checks and to use this information in quality assurance of individual performance and of the training programs (A-95-116)
-
Require specified airlines and training establishments to provide such information to the FAA for incorporation into a storage and retrieval system (A-95-117)
-
Maintain an FAA storage and retrieval system that contained pertinent standardized information on the quality of specified airline pilot performance during training (A-95-118)
-
Require specified airlines to obtain information from the FAA's storage and retrieval system that contains pertinent standardized pilot training and performance information for the purpose of evaluating applicants for pilot positions during the pilot selection and hiring process. The system should have appropriate privacy protections, should require the permission of the applicant before release of the information, and should provide for sufficient access to the records by an applicant to ensure accuracy of the records (A-95-119)
In response to these recommendations, the FAA worked with the United States Congress, resulting in the Pilot Records Improvement Act of 1996 (PRIA), which required that any company hiring a pilot for air transportation request and receive records from any aviation carrier, company, organization, or person that had employed a pilot applicant during the previous five years.
The PRIA required specified air carriers to obtain specified records from previous employers of pilot applicants before allowing an applicant to begin service as a pilot. The PRIA also required all air carriers to obtain from the FAA a pilot applicant's current medical certification and airman certification and any record of closed enforcement actions. On 02 June 1997, the NTSB classified Recommendations A-95-117 through A-95-119 as "Closed—Acceptable Alternate Action."
The PRIA addressed many of the NTSB's concerns that had led to Recommendation A-95-116. In response to the recommendation, the FAA asserted that much of the information desired in the recommendation is already available to prospective employers through applicant scores on certain written tests and failed manoeuvres noted in the FAA forms used to record pilot performance in commercial and airline transport pilot flight checks. The FAA also argued that inclusion of subjective evaluations in the permanent record may have the effect of making the training event a punitive experience rather than one where individuals can learn from mistakes. On 01 March 2000, the NTSB classified Recommendation A-95-116 as "Closed – Reconsidered."
After investigating a fatal accident on 13 July 2003 involving a Cessna 402C, the NTSB determined that the probable cause of this accident was the in-flight failure of the right engine and the pilot's failure to adequately manage the airplane's performance after the engine failed. The investigation determined that, from April 1983 to February 1998, the accident pilot had failed nine flight checks. The NTSB identified that employers have no means to verify the information provided by applicants regarding previous flight test failures, because the PRIA did not require that airlines obtain FAA records documenting failed flight checks.
The NTSB concluded that a record of multiple flight check failures may be an indication of a pilot applicant's unsatisfactory flight proficiency, and that a review of information regarding previous flight test failures would allow prospective employers to assess a pilot applicant's experience and determine whether an applicant has a history of unsatisfactory performance. On 27 January 2005, the NTSB issued safety recommendations A-05-01 and A-05-02 to the FAA to:
-
Require all Part 121 and 135 air carriers to obtain any notices of disapproval for flight checks for certificates and ratings for all pilot applicants and evaluate this information before making a hiring decision. (A-05-01)
-
Conduct a study to determine whether the number of flight checks a pilot can fail should be limited and whether the existing system of providing additional training after a notice of disapproval is adequate for pilots who have failed multiple flight checks. On the basis of the findings of the study, establish a flight check failure limit and modify the recheck training requirements, if necessary. (A-05-02)
To address the safety concern outlined in Recommendation A-05-1, the FAA indicated that it would amend Advisory Circular (AC) 120-68, Pilot Records Improvement Act of 1996, to add the following note after subparagraph 8(a)(4)(a): "Additional information. A letter of consent signed by a pilot job applicant may be used to authorize the FAA to release records of Notices of Disapproval for flight checks for certificates and ratings to an air carrier making such a request." Air carrier representatives involved in screening pilot job applicants may find this additional information helpful in evaluating an applicant.
The NTSB concluded that the FAA's proposal to amend AC 120-68 may be an acceptable alternative that could meet the intent of the recommendation in a timely manner. Pending the revision of AC 120-68 as proposed, and results of a survey of carriers demonstrating that they require the consent form as a condition of employment by a pilot applicant, the NTSB classified Recommendation A-05-1 as "Open-Acceptable Alternate Response." The NTSB expressed concern that the FAA-proposed action was an interim solution and urged the FAA to pursue rulemaking changes or changes to the statute itself in order to more adequately satisfy this recommendation.
In response to Recommendation A-05-02, the FAA conducted a study in 2004 to determine if there is a correlation between flight test failures and the airman being cited in an FAA enforcement action. A review of a total of 15 024 disapprovals against the FAA Enforcement Information System showed a very low correlation—less than one per cent. The FAA indicated that, while any single case of involvement in an FAA enforcement action may have little significance, taken collectively, involvement in enforcement can be an indicator of lack of qualities that make up a safe pilot, including required skills, knowledge, or compliance disposition.
The FAA stated that there were systems in place to enable specified operators to take additional steps to screen applicants and that the amendment to AC 120-68 would strengthen the use of letters of consent to authorize the FAA to release records of Notices of Disapproval for flight checks to prospective employers.
The NTSB concluded that the study conducted by the FAA was responsive to Recommendation A-05-02 and classified the recommendation as "Open-Acceptable Response" pending receipt of a report describing the study, a statement from the FAA on the conclusions drawn from the study results, and appropriate action in response to those findings.
Appendix I – Glossary
- AC
- Advisory Circular
- ACIM
- Air Carrier Inspector Manual
- ACP
- approved check pilot
- AFM
- aircraft flight manual
- agl
- above ground level
- AIM
- Aeronautical Information Manual (Transport Canada)
- AOC
- air operator certificate
- ARASS
- Activity Reporting and Standards System
- ARCAL
- aircraft radio control of aerodrome lighting
- ARP
- aerodrome reference point
- asl
- above sea level
- ATC
- air traffic control
- ATPL
- airline transport pilot licence
- ATS
- air traffic services
- CAD
- Civil Aviation Directive (Transport Canada)
- CADORS
- Civil Aviation Daily Occurrence Reporting System
- CAP
- Canada Air Pilot
- CARs
- Canadian Aviation Regulations
- CASO
- company aviation safety officer
- CASS
- Commercial Air Service Standards
- CBA
- Commercial and Business Aviation
- CBAAC
- Commercial and Business Aviation Advisory Circular
- CCP
- company check pilot
- CFIT
- controlled flight into terrain
- CFS
- Canada Flight Supplement
- CJY4
- Sandy Bay aerodrome
- CRFI
- Canadian Runway Friction Index
- CRM
- crew resource management
- CVR
- cockpit voice recorder
- DACP
- designated approved check pilot
- DFO
- Director of Flight Operations
- DGCA
- Director General, Civil Aviation (Transport Canada)
- DME
- distance measuring equipment
- ELT
- emergency locator transmitter
- EMT
- emergency medical technician
- FAA
- Federal Aviation Administration (United States)
- FARs
- Federal Aviation Regulations (United States)
- FCTM
- flight crew training manual
- FDR
- flight data recorder
- FO
- flight operations
- FOIPD
- Frequency of Inspection Policy Document
- FOM
- flight operations manual
- fpm
- feet per minute
- FTE
- full-time equivalent
- GFA
- graphic area forecast
- GNSS
- global navigation satellite system
- GPI
- ground point of interception
- GPS
- global positioning system
- HAT
- height above touchdown zone elevation
- IAM
- Inspection and Audit Manual
- IFR
- instrument flight rules
- ICAO
- International Civil Aviation Organization
- ILS
- instrument landing system
- IMC
- instrument meteorological conditions
- in Hg
- inches of mercury
- ISA
- International Standard Atmosphere
- LOSA
- line operations safety audits
- MDA
- minimum descent altitude
- METAR
- meteorological actual report (aviation routine weather report)
- MF
- mandatory frequency
- MHz
- megahertz
- N
- north
- NACIS
- National Aviation Company Information System
- NAP
- national audit program
- NCAMX
- National Civil Aviation Management Executive
- NCP
- northern chief pilot
- NDB
- non-directional beacon
- nm
- nautical miles
- NOTAM
- notice to airmen
- NOTIP
- National Organization Transition Implementation Project
- NPRM
- notice of proposed rulemaking
- NTSB
- National Transportation Safety Board (United States)
- OD
- operations directive
- OFP
- operational flight plan
- OLS
- obstacle limitation surface
- OPI
- office of primary interest
- OPS
- SPEC 99 operations specification 99
- PAPI
- precision approach path indicator
- PF
- pilot flying
- PIC
- pilot-in-command
- PNF
- pilot not flying
- PNR
- Prairie and Northern Region (Transport Canada)
- POI
- principal operations inspector
- PPC
- pilot proficiency check
- PRIA
- Pilot Records Improvement Act (United States)
- PV
- program validation
- RCAP
- Restricted Canada Air Pilot
- RDCA
- Regional Director, Civil Aviation (Transport Canada)
- RDIMS
- Records, Document, and Information Management System
- RIP
- restricted instrument procedures
- RNAV
- area navigation
- SCP
- southern chief pilot
- SD
- safety directive
- SIC
- second-in-command
- sm
- statute miles
- SMS
- safety management system
- SOPs
- standard operating procedures
- TC
- Transport Canada
- TCCA
- Transport Canada Civil Aviation
- TCH
- threshold crossing height
- TEM
- threat and error management
- TP
- Transport Canada publication
- TSB
- Transportation Safety Board of Canada
- TWA
- Transwest Air
- TW350
- Transwest Air Flight 350
- VASIS
- visual approach slope indicator system
- VOR
- very high frequency omni-directional radio range
- W
- west
- °
- degrees
- ′
- minutes
- °C
- degrees Celsius
- °M
- degrees magnetic
- °T
- degrees true