Loss of Engine Power and Collision with Terrain
Bighorn Helicopters Inc.
Bell 206B Jet Ranger (Helicopter) C-GCHE
Cranbrook, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
At 1209 mountain daylight time, the Bighorn Helicopters Inc. Bell 206B Jet Ranger helicopter (registration C-GCHE, serial number 1249) took off from the company heliport on the outskirts of Cranbrook, British Columbia, with the pilot and two passengers on board. The helicopter then carried out a low-level visual inspection of high-voltage electrical power lines that passed through the suburban areas of Cranbrook. At about 1306, as the helicopter was flying southbound at about 120 feet above the ground, a sudden loss of engine power occurred causing rapid loss of rotor rpm. The helicopter descended quickly and landed heavily on a paved street below the flight path. The helicopter struck a pedestrian on the sidewalk adjacent to the impact point, as well as a motor vehicle travelling west on the street.
The helicopter broke into several pieces and burst into flames. The three occupants of the helicopter and the pedestrian were fatally injured at impact. The motor vehicle was damaged but its occupant was uninjured. The helicopter was destroyed by an intense fuel-fed, post-crash fire. The emergency locator transmitter (ELT) was consumed by the fire and it is unknown if it transmitted a signal. The accident site is located within the city of Cranbrook at latitude 49°29′56″ N and longitude 115°45′40″ W, at an elevation of about 3100 feet above mean sea level.
Factual information
History of Flight
The flight profile was established by BC Hydro and had been pre-planned by the pilot and his two passengers, both BC Hydro power line technicians. The mission was to visually examine the 60 kVA (kilovolt-amperes) electrical power transmission lines that ran north from the Moyie/McGillivray area, through the city of Cranbrook, out to the east of the city, and then northwest (see Appendix A – Planned Power Line Inspection Route).
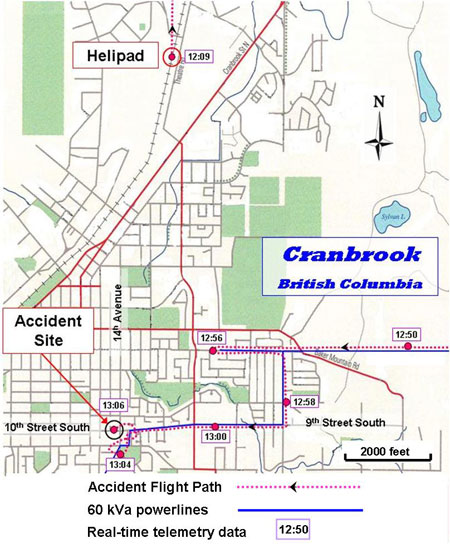
The task required the technicians to identify and record any line and pole anomalies so that a ground party could inspect and repair them at a later date. To accomplish this task effectively, it was necessary for the inspection to be carried out at about 20 to 30 feet above the line or pole heights, at a ground speed in the order of 25 knots. Real-time telemetry data received from the helicopter during the accident flight confirm that such a profile was flown during the portion over the city. These data are not sent continuously from the helicopter, but rather in two-minute packets, resulting in voids in the flight path tracking. However, sufficient data blocks were recorded to recreate the flight path.

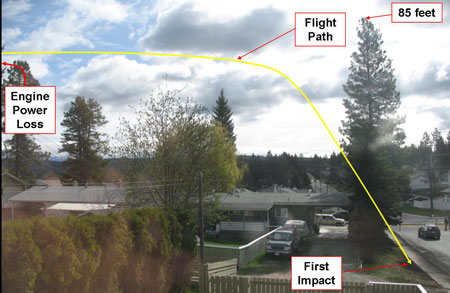
The accident flight took off from the Bighorn Helicopters Inc. helipad in the northern part of the city at 1209, Footnote 1 flew along the power lines to the northwest of the city, and retraced that route to follow the lines to the east, then turned south. At 1247, the helicopter turned west to follow the lines into the city residential area. At 1258, the helicopter was flying south down 30th Avenue South, Footnote 2 then turned right to follow the power lines west on 9th Street South. Four minutes later, in the vicinity of 10th Street and 14th Avenue, the helicopter carried out several low-altitude manoeuvres (see Photo 1 and Appendix B – Cranbrook City Map), apparently examining the power lines in that area. It was flying south-southwest over 14th Avenue (midway between 7th and 10th Streets) at about 120 feet above ground level (agl) and 25 knots when the engine lost power (see Photo 2). The helicopter descended rapidly; the final few seconds of flight were uncontrollable and in free-fall from about 85 feet above the ground.
Weather
The meteorological conditions in the area at the time of the accident were suitable for visual flight, with an overcast sky and a wind generally from the southwest at about 10 knots, and no reported turbulence. The temperature was not formally recorded at the accident site, but the 1300 Cranbrook Airport hourly observation recorded the temperature as 12°C, and the urban area was likely slightly warmer. The weather conditions did not contribute to the accident circumstances.
Pilot
The pilot was certified and qualified for flight in accordance with existing regulations. He held a valid Canadian pilot licence (Commercial Pilot – Helicopter) and had accumulated about 5100 hours of total flying experience, of which 1600 hours were on Bell 206 helicopters. He had begun to work for Bighorn Helicopters Inc. as a line pilot in July 2007 and had met all company recurrent ground and flight training requirements. The pilot was appropriately rested before commencing his duty day. This Cranbrook BC Hydro operation had started on the day of the accident, and the pilot had flown about 2.5 hours for BC Hydro. He was characterized by clients and peers as being a competent and cautious pilot.
Helicopter Information
The accident helicopter was a Bell 206B Jet Ranger and was manufactured in 1974 by the Bell Helicopter Company in Texas, United States. Since then, the helicopter had accumulated about 16 500 total hours in service. The maintenance logs and records indicated that the helicopter had been certified, equipped, and maintained in accordance with existing Canadian regulations and approved procedures.
Crash Site and Wreckage Information
At the accident site, the direction of the final seconds of flight was essentially into the prevailing wind. The helicopter struck the gently rising ground on 10th Street South, about 300 feet west of 14th Avenue South. It was generally an open area but had several obstructions that the pilot may have tried to avoid during descent. On the east side of the crash site, there were two tall evergreen trees, with the higher being about 85 feet tall. As well, there was a set of residential power lines running north-south, and a residence below (see Photo 2). Given the relative positions and motions of the car, the helicopter, the pedestrian, and the trees, it is unlikely that the pilot saw either the pedestrian or the car before impact.
During the last two seconds of flight, the helicopter descended almost vertically to the street in a nose-up, left-side-down attitude. The tail boom stinger and tail rotor blades struck the ground first, causing the tail rotor gearbox section to break off. The main fuselage then struck the street with such force that the landing skids broke up and the cabin, engine and transmission platform, and airframe structure collapsed, bursting the fuel cell. The helicopter slid forward about 20 feet, rotated about 200°, and came to rest heading opposite to its flight path. Both rotor blades were intact and street-impact damage to one blade was confined to the outboard three-foot section. Seconds after impact, a fire began and, within a minute, it had intensified into a fierce fuel-fed fire, with a large stream of burning fuel flowing down the street gutter. The Cranbrook Fire Department arrived within four minutes of the crash and extinguished the fire; about 60 per cent of the helicopter was consumed. The engine, main transmission, and rotor head survived the fire. Some components thrown free during breakup were unaffected by the fire.
The airframe wreckage was examined to the extent possible, but the level of mechanical and thermal destruction prevented any determination of flight control continuity. For the few airframe components that did survive, no indication was found of any pre-accident anomaly or malfunction with the flight controls, the drive train, or other aircraft system that could have contributed to the accident circumstances.
Engine Examination
The engine installed in the accident helicopter was a Detroit Diesel Allison Division of General Motors Corporation model 250-C20, serial number CAE-821311. The Rolls-Royce Corporation is the current Federal Aviation Administration (FAA) type certificate holder for this model engine. Footnote 3 The engine is a modular design, comprising compressor, turbine, and accessory gearbox assemblies, and is rated at 400 shaft horsepower (shp).
The engine was removed from the accident helicopter and disassembled by an approved engine overhaul facility under the direct supervision of the TSB. During this examination, the fuel control unit (FCU) and the power turbine governor (PTG) were removed and subjected to further examination and analysis.
Both the FCU and the PTG were installed on the engine in June 2006 as new components. At the time of the accident, they had accumulated about 1130 hours of continuous service, well within the time before overhaul (TBO) of 2500 and 2000 hours for the FCU and PTG respectively.
The engine had suffered some external thermal damage to the accessory gearbox section, but otherwise was intact and could be examined in detail. In summary, the examinations of the compressor, turbine, and gearbox assemblies revealed that the engine was rotating relatively slowly at impact with the ground, and at an rpm considerably less than self-sustaining. This rpm was consistent with usual engine spool-down. No mechanical reason for the low rpm was found in the engine assemblies and no pre-impact damage or anomaly was seen.
Gas Turbine Fuel Control Unit
The Honeywell FCU (model DP-N2) is the basic component of the fuel controlling system for the Rolls-Royce 250-C20 series gas turbine engines. It is a pneumatic-mechanical device that schedules fuel flow to the engine and provides proper engine operation and specification performance. The FCU is mounted on the engine accessory gear case, and is driven at a speed proportional to gas producer turbine speed (N1). Of the six parameters required by the fuel control to properly schedule fuel flow, two are linked to the PTG.
The accident FCU was disassembled and examined in detail. It had been exposed to extreme temperatures during the post-crash fire and had suffered remarkable thermal damage. The TSB tests showed no mechanical anomaly that could have affected the function of the FCU (see TSB laboratory report LP 098/2008 for further details). However, a latent malfunction of the FCU could not be ruled out.
Power Turbine Governor
The Honeywell PTG (model AL-AA2) complements the Honeywell DP-N2 FCU and is an essential element of the fuel management system on the Rolls-Royce 250-C20 series engines. The function of the governor is to maintain the speed of the power turbine (N2) by resetting the main fuel control during engine operation. This resetting establishes the gas producer turbine speed (N1) required to supply N2. A malfunction of the PTG in flight would certainly affect the correct operation of the FCU and, depending on the type of PTG failure, could cause the engine to lose power.
The PTG was disassembled and examined in detail. It too had been exposed to extreme temperatures during the post-crash fire and had suffered thermal and mechanical damage. The single anomaly found was a loose spacer shim inside the unit.
The Honeywell PTG was originally manufactured with spacer shims on two shafts. Subsequently, Honeywell determined that one of the shafts did not require shims and these were removed from the design, altering the illustrated parts catalogue (IPC) and the maintenance/servicing instructions. However, several units were unintentionally assembled by Honeywell with spacer shims on both shafts after the design change took effect. TSB research revealed that shims had been found in that location in other overhauled PTGs, and that Honeywell was aware of the practice. The accident PTG was manufactured after the design change.
A detailed examination was carried out by the TSB Laboratory in Ottawa (see TSB laboratory report LP 098/2008 for further details). A scanning electron microscope examination of the loose spacer shim revealed that it had been installed on the cam follower pin between the cavity wall and the end of the lever assembly. This was the shaft that no longer required shimming. The other shaft was still in place with its associated shims.
Therefore, it can be concluded that the loose spacer shim had been deliberately installed at manufacture and had separated from the shaft during disassembly after the accident. No evidence was found of interference by the spacer shim as installed. It had been assembled correctly in accordance with previous assembly instructions. No link to any PTG functional anomaly was identified.
Given that this model of PTG had failed in the recent past, the TSB examined the accident unit to determine if these previous failure characteristics were present and had any impact on the function of the PTG in the circumstances of this accident. No suspicious damage of the vulnerable parts was found, leading to the preliminary conclusion that the problematic areas of weakness likely did not play a role in PTG malfunction. However, a latent anomaly in the PTG could not be ruled out.
Previous TSB Investigation
In the course of investigating a dual engine power loss accident in February 2005 (TSB investigation report A05P0038), the TSB discovered that the same PTG units were apparently problematic. In April 2005, the TSB issued an Aviation Safety Advisory (A050009-1) to Transport Canada (TC), wherein the TSB in part revealed that records from a major repair and overhaul facility in Canada indicated that the PTG on the Rolls-Royce 250-C20 series engine had an average service life of 1150 hours Footnote 4 since repair/overhaul before repair was required. The PTG on C-GCHE had accumulated 1130 hours since new.
Similar PTGs on the Pratt & Whitney (PWC) PT6T3 engines had an average of 1600 hours before repair was required. It is noteworthy that the TBO for the PTG is 2000 hours for the Rolls-Royce application, and 4500 hours for the PWC application. The thrust of the TSB Advisory was to suggest that TC may wish to review the applicable TBOs for the PTG unit. In July 2005, TC responded that its review of the service difficulty reporting database did not indicate a chronic problem with the TBOs, and proposed no further action.
Helicopter Weight and Balance
Shortly before take-off on the accident flight, the pilot reportedly added fuel to achieve a total of 75 US gallons on the cockpit fuel quantity gauge, which was more than adequate for the proposed mission. The helicopter flew for 57 minutes before the accident, and as a result, the fuel remaining would have been about 50 US gallons or 350 pounds. It was evident from the rivulet of burning fuel at the accident site that a large amount of fuel was on board at impact.
TSB investigators calculated that the gross weight of the helicopter at the time of the accident was about 2850 pounds. With reference to the Bell 206B rotorcraft flight manual (RFM), the maximum gross take-off weight is 3200 pounds (internal load). These calculations also indicated that both the longitudinal centre of gravity (CG) and lateral CG were within certified limits. The weight and CG were within prescribed limits.
Hover Performance
The crash site was about 3100 feet above sea level (asl) and, with an air temperature of 12°C, the density altitude would have been in the order of 3400 feet asl. With reference to the Bell 206B RFM, the hover ceiling out of ground effect (HOGE) chart ensures that the helicopter can hover without the performance benefit of ground effect, by providing a maximum allowable gross weight for varying conditions of pressure altitude and outside air temperature. For the environmental conditions at the time of the accident, the HOGE chart showed that the weight of the helicopter with the three occupants on board would have been within the HOGE performance capability of the helicopter (see Appendix C - Hover Ceiling Out of Ground Effect).
Helicopter Autorotation
Helicopter autorotation is a complex aerodynamic process. A simplified description to aid the reader follows.
Autorotation permits a helicopter to descend in a controlled manner after engine power loss or other catastrophic mechanical failure and still permits the pilot to carry out a safe landing; it applies to all helicopters regardless of the number of engines installed. As in a "dead-stick" landing with a fixed-wing aircraft, there is no possibility of a go-around following an autorotation resulting from an actual emergency; there is no second chance.
A critical aspect of autorotation is the entry manoeuvre immediately following the loss of engine power because the pilot must react quickly to conserve rotor rpm. Of the other factors affecting autorotative flight, the altitude at the time of the loss of engine power immediately establishes several important elements of successful descent and landing. The greater the height above the landing surface, the greater choice of suitable landing areas, the more time to establish and maintain control of the helicopter, and the longer the glide distance. Low-altitude flight reduces all these margins to the point where successful autorotative flight and landing may be impossible.
The no-engine landing after an autorotative descent is a challenging manoeuvre for any helicopter pilot since it involves skills not frequently practiced within an unforgiving flight regime. For this accident, the pilot had several obstacles to avoid, namely the residential power lines, tall trees, several houses, and vehicular traffic. These all greatly restricted the pilot's manoeuvring and choice of landing sites. Further, he was faced with the dilemma of extending the glide to avoid the houses at the expense of controlled flight. In these circumstances, the pilot had insufficient altitude to maintain functional rotor rpm following the engine power loss, and the final few seconds of flight were uncontrollable and in free-fall from about 85 feet above the road.
Height Velocity Diagram
The height velocity diagram (HVD) is unique to helicopter operations. For the single-engine helicopter, the HVD shows in graph format those combinations of airspeed and height above the ground where either a fully developed autorotative glide can be entered or a safe landing carried out, after the helicopter suffers an engine power loss. There is also the supposition that the pilot is able to carry out a successful engine-out landing.
The HVD itself is constructed by progressive trials during the original certification flight test regimes by the helicopter manufacturers' test pilots. The HVD is not a limitation in the RFM, but rather a guide to pilots to show the flight profiles where they are exposed to the greatest risk resulting from engine power loss, and so identifies height and speed combinations to avoid or pass through quickly. These combinations are clearly identified on the graph by shaded (hatched) areas.
The two-part HVD for the Bell 206B is contained in Section 3 – Performance of the RFM and is shown in Appendices D and E of this report. Note that the airspeed is referenced in miles per hour (mph). The HVD shows that a pilot should not expect to establish full autorotation from heights between 40 and 200 feet above the ground, unless the airspeed is above 45 mph. In the case of C-GCHE, the helicopter was at about 120 feet agl and travelling at about 30 mph; with such height and speed, the helicopter could not have achieved full autorotation before it struck the ground.
Crashworthiness/Survivability
The level of airframe destruction demonstrates extreme impact forces and is consistent with high vertical speed. Such damage is characteristic of the magnitude of impact forces that exceed human tolerance levels, and as a result, the crash was not survivable. The pedestrian was struck forcefully by a main rotor blade and could not have survived the trauma. Medical information and injury patterns indicate that the pilot and front passenger in the cockpit were wearing full seat restraints, and the pilot was wearing a flight helmet; the rear passenger was also wearing his full seat belt and harness.
Canadian Aviation Regulations Requirements for Flight over Built-up Areas
The Canadian Aviation Regulations (CARs) and Commercial Air Service Standards (CASS) prescribe the altitudes at which aircraft may be flown. These requirements include: CARs Section 602.14 – Minimum Altitudes and Distance; CARs Section 602.15 – Permissible Low Altitude Flight; CARs Section 702.22 – Built-Up Area and Work Zone; and CASS Section 722.22 – Built-Up Area and Work Zone.
CARs Section 602.14 is a general prohibition. It forbids operating an aircraft over a built-up area unless it is operated at an altitude from which it would be possible to land without creating a hazard to persons or property on the surface. In any case, that altitude for helicopters is not to be lower than 1000 feet above the highest obstacle within a horizontal distance of 500 feet. In circumstances other than these, the aircraft is not to be operated at a distance of less than 500 feet from a person, vessel, vehicle or structure. CARs Section 602.12 deems a helicopter to be over a built-up area when it is within 500 feet horizontally of that built-up area.
The CARs recognize that certain forms of aerial work necessitate flight at lower altitudes. For flights over built-up areas, CARs Section 602.15 provides two lets. In this case, only the second, SubSection 602.15(2), would allow operations at lower altitudes provided the flight is authorized either under Subpart 603 – Special Aviation Events, or under CARs Section 702.22. While the accident flight was involved in aerial inspection, the flight was being conducted for hire and reward — a commercial operation — in which case it would be bound by the requirements of Part VII of the CARs and not those under Subpart 603.
Bighorn Helicopters Inc. holds two air operator certificates issued under Subpart 702 - Aerial Work and Subpart 703 – Air Taxi Operations of the CARs. As the accident flight involved power line patrol, it would have likely been operating under the auspices of the Subpart 702 certificate.
SubSection 702.22(2) allows a person to operate over a built-up area at altitudes and distances less than the general prohibition if the person is so authorized by the Minister, or is authorized to do so in an air operator certificate; and complies with the CASS.
To obtain air operator authority, SubSection 722.22(1) of the CASS requires an aerial work zone plan to be submitted to the TC Aviation Regional Office at least five working days in advance of the operation and prescribes the information that must be submitted. Furthermore, Subsection 722.22(3) requires the air operator to submit an application, show a requirement for operating certificate authority, and amend its company operations manual (COM) to include the routes and conditions for their use.
The specific criteria by which TC grants or withholds authorization to meet the requirements for procedures and precautions to be taken to ensure that no hazard is created to persons or property on the surface, including locations of forced landing areas in the event of an emergency, are unknown. Furthermore, the standard is silent on the type of aircraft that can be used for such flights; for example, the circumstances under which single-engine versus multi-engine aircraft could or should be used.
In summary, Bighorn Helicopters Inc. could not avail itself of the let under SubSection 602.15(1). It was not subject to Subpart 603; rather it was bound by the requirements of the general prohibition under Section 602.14 and/or the conditions set out in Subpart 702. Bighorn Helicopters Inc.'s COM is silent on low-level aerial inspection operations. It had not applied for, or received, authorization from the Minister of Transport, nor had it submitted an area work zone plan.
Previous Low-Altitude Operations
Low-altitude aerial inspection flights over built-up areas have been undertaken in Canada for at least the past 30 years, and regulatory requirements for such flights have existed in one form or another throughout.
During this investigation, an informal survey of helicopter operators was conducted. It became evident that much misunderstanding existed regarding the interpretation and application of altitude requirements. In all likelihood, low-altitude aerial inspection flights are being carried out over built-up areas in Canada without full compliance with regulatory requirements.
Analysis
The helicopter was functioning normally until an event caused the engine to either lose power or shut down. The cause of the loss of engine power was not determined. The interruption to engine power resulted in rapid loss of rotor rpm to the point where the pilot was unable to effectively control the helicopter. The helicopter descended almost vertically and collided heavily with the street and collapsed. The three occupants could not have endured the impact forces and the pedestrian was struck forcefully by a rotor blade. In summary, there are two causal events: a loss of engine power and a loss of flight control, in that order.
The analysis will focus on the loss of engine power, the possibility that FCU or PTG function contributed to the accident circumstances, and the flight performance that was available from the helicopter and its effect on the accident circumstances. Further, the interpretation of applicable CARs will be discussed.
Loss of Engine Power
A loss of engine power is the result of either pilot action or mechanical event. A pilot can roll off the throttle or close the firewall fuel valve, but given the low profile of the accident flight, there is no scenario in such flight conditions to cause an experienced pilot to do so, with one exception — a complete loss of tail rotor thrust. The tail boom and tail rotor survived the accident and an examination revealed no tail rotor anomaly. Accordingly, it is unlikely that deliberate pilot action precipitated the engine power loss.
A helicopter comprises three major parts — the engine(s) including related systems, the rotor system drive train, and the airframe with its related systems. It can be reasonably argued that few airframe failures can cause a helicopter turbine engine to lose power or stop. Despite the destruction of much of the helicopter, critical components did survive, and no evidence was found that an airframe or drive train event caused the engine to lose power.
From an engine-related perspective, fuel exhaustion or starvation can also be a cause. In this accident, fuel exhaustion was not a factor as demonstrated by the large amount of spilled fuel at the accident site. Fuel starvation, resulting from blocked or fractured fuel lines for example, cannot be ruled out.
Loss of Flight Control
There was no indication of any pre-accident malfunction of any flight control or rotor drive system on the helicopter that could have contributed to a loss of control of the helicopter.
Engine Performance
No evidence was found to suggest that any of the engine modules had suffered any pre-impact mechanical event that would have contributed to a loss of engine power.
Fuel Control Unit Performance
Had the FCU malfunctioned in some manner, the effect on the engine operation could have been immediate. The FCU could have malfunctioned as a result of internal anomalies, blocked or leaking pneumatic lines, or as a result of anomalous signals from the PTG. Either way, the FCU would have commanded the engine improperly. Depending on the type of malfunction, the FCU could have commanded the engine to either increase or decrease speed, with the associated rotor rpm increase or decrease. It is known that the engine rpm and the rotor rpm suddenly decreased seconds before impact, and the rotor speed decayed remarkably in descent.
The accident FCU was thermally damaged, precluding functional testing, and as a result, the in-service function of the FCU was not assessed. Examination of the FCU and its components did not identify a failure mode that could have led to the sudden loss of engine power. However, this does not rule out the possibility that the FCU did malfunction. It could have precipitated the loss of power either individually or in combination with the PTG.
Power Turbine Governor Performance
Because the PTG was installed new and remained on the engine since that time, it can be deduced that the spacer shim found loose was placed on the shaft during manufacture in accordance with pre-design change specifications. There had been no reported functional anomalies with the PTG in over 1100 hours of service since its installation on the accident engine in June 2006. However, given the remarkable shortfall in average service life of the units, it is possible that the PTG malfunctioned.
Operating Environment
Several operational conditions existed to present the pilot with a greater-than-usual challenge for an emergency landing following the loss of engine power, namely:
- obstructions on the final flight path;
- low airspeed;
- low height above the terrain;
- low rotor rpm; and
- short time frame.
The above factors individually represent significant difficulty for a pilot to achieve a successful outcome, but when combined, they pose operational challenges that a pilot may not overcome. Furthermore, each factor has a negative synergistic effect on the other, and the resulting situation deteriorates rapidly.
Rotorcraft Flight Manual Information
The RFM includes valuable information that identifies operational conditions posing high risk in the event of a loss of engine power. The HVD shows that low altitude and low airspeed combinations present a significant challenge to pilots in landing successfully from an event that requires an immediate landing, such as an engine malfunction. On the HVD, such higher risk zones are labeled "avoid" areas and represent the worst circumstances for recovery.
Accident Flight Conditions
In reviewing the accident flight path, it can be seen that the helicopter was frequently exposed to the higher-risk avoid zones of the HVD during its passage over the built-up areas of Cranbrook. Under these conditions, the helicopter would not have had sufficient altitude or time to develop autorotative flight following a sudden loss of engine power. As a result, the pilot would have had no opportunity to conserve rotor rpm and a high rate of descent would have developed rapidly. Any manoeuvring by the pilot to avoid obstacles would have exacerbated this deteriorating condition.
Low-Altitude Flight
The likelihood of a loss of power is independent of the altitude, the speed, or the terrain. However, the risk of an unsuccessful landing following a power loss increases with lowering altitudes and speeds, and worsening terrain. The HVD assumes that the terrain is suitable and considers altitude and airspeed only, without any discrimination for other operational factors, such as pilot skill or experience, weather, or obstacles. The HVD is thus a best-case scenario and shows the optimum flight path profile for take-off, landing, and en-route regimes, based upon helicopter aerodynamic performance.
The CARs prescribe conditions for low-altitude flight in helicopters over built-up areas that, in general, ensure the manner of operation does not create a hazard, and that the altitude (height) of a flight is such that an immediate landing can be made without creating a hazard. The provisions of the CARs are based upon hazard management and do not specifically take aerodynamic risk, such as the HVD, into account. For example, though the CARs permit deviation from the prescribed altitude minima, they do not imply that the helicopter is safe to fly at the same height inside the avoid areas of the HVD.
The operation of the helicopter inside the HVD avoid areas, or the apparent non-compliance of the operations with the applicable CARs respecting low-altitude flight, had absolutely no link to the loss of engine power, and neither was causal. The severity of the outcome, however, was influenced by the low altitude and airspeed, and the landing site environment.
Low-Altitude Flight Safety Defences
Information contained in the RFM (such as the HVD) assist operators and pilots in choosing the most appropriate flight profiles for their missions and take into account helicopter performance. Even though the CARs prescribe regulatory limitations and procedures, it is important that they be applied in concert with the RFM information. It is noteworthy that a constantly repeating theme throughout the CARs is that flight operations must not create a hazard to people or property on the surface. Accordingly, the final responsibility for safe operational practices remains with individual helicopter operators and pilots.
Canadian Aviation Regulations Requirements for Low-Level Flight over Built-up Areas
The requirements governing flights over built-up areas are located in several areas of aviation regulation; they are complex and subject to wide interpretation, such as when an aircraft is or is not over a built-up area and which requirements would apply where and under what circumstances.
While the accident flight involved the aerial inspection of power lines, these were located within a residential community. The helicopter performed manoeuvres over homes in the vicinity of the power lines. Therefore, the accident flight took place over a built-up area and would have been bound by the general prohibition under Section 602.14 and/or the conditions set out in Subpart 702.
Like many operators, Bighorn Helicopters Inc. interpreted its low-level power line operations to be either a flight inspection or being conducted other than over a built-up area. If the former was true, Bighorn Helicopters Inc. would likely have seen itself exempt from the general prohibition as granted under SubSection 602.15(1). But flight inspection is limited to navigation aid inspection and obstacle assessment.
If the company viewed its operation as being conducted elsewhere than over a built-up area, the general prohibition would have required the helicopter to be operated at 500 feet. However, paragraph 602.15(2)(b) allows operation at lower altitudes and distances if the aircraft is operated without creating a hazard to persons or property on the surface and the aircraft is operated for the purpose of aerial inspection, including power line patrol. Under these circumstances, Ministerial approval or authorization is not required.
Regardless of the specific requirements, the condition that such flights shall not create a hazard to persons or property on the surface is constantly repeated. In the absence of clear direction and guidance, companies may select the requirements that impose the least stringent conditions. Therefore, low-level aerial inspection flights over built-up areas will continue, thereby creating a hazard to persons and property on the surface. While TC may not have articulated the criteria by which it will grant or withhold authorizations for low-level flights over built-up areas, it became clear during this investigation that this flight would not likely have been authorized using a single-engine helicopter.
The following TSB laboratory report was completed:
LP098/2008 – Bellows Analysis
This report is available upon request from the Transportation Safety Board of Canada.
Findings
Findings as to causes and contributing factors
- The engine lost power at an altitude and airspeed combination that did not permit fully developed autorotative flight, resulting in rapid loss of rotor rpm, an extremely high rate of descent, and a severe collision with the terrain.
- The helicopter was being operated at a height and airspeed combination that the helicopter manufacturer had determined would, in the event of an engine power loss, preclude a successful descent and landing.
- During the final seconds of the flight path, the pilot was hindered by several obstacles that afforded him only one clear landing site that was beyond the gliding range of the helicopter. The pilot's efforts to avoid the house and reach that site exacerbated the already high rate of descent.
- The helicopter was not in a controlled descent and, coupled with the decaying rotor rpm, the pilot's ability to control the helicopter was decreasing so rapidly that the last 85 feet of height was in free-fall.
Findings as to risk
- Flights conducted at altitudes that do not permit safe descent, manoeuvring and landing following an event that requires a single-engine helicopter to land immediately create risk to persons and property, particularly in built-up areas.
- The Canadian Aviation Regulations requirements for low-level aerial inspection flights over built-up areas are complex and subject to wide interpretation. In the absence of clear direction and guidance, companies may select the requirements that impose the least stringent conditions. Therefore, low-level aerial inspection flights over built-up areas will continue, thereby creating a hazard to persons and property on the surface.
Other Finding
- The cause of the loss of engine power was not determined; it is possible that a mechanical event with the fuel control unit or the power turbine governor occurred, or fuel starvation, or some combination of these.
Safety action
Action Taken
Transport Canada
Since the accident, Transport Canada (TC) crafted a logic chart for pilots and operators to guide them in correct decision making regarding the minimum altitudes and distances over built-up areas prescribed by the Canadian Aviation Regulations (CARs). TC plans to reproduce this chart in the TC publication TP 185E, Aviation Safety Letter.
TC performed a search of the Service Difficulty Reporting System for power turbine governor (PTG) reports and 400 were retrieved. TC sent a letter to the Federal Aviation Administration (FAA), the country of type design responsibility, requesting a review of the service difficulty reporting data. The FAA has been requested to provide its analysis regarding the reliability of the governor and if any corrective action is necessary.
Bighorn Helicopters Inc.
Bighorn Helicopters Inc. revised its operational practices regarding low-altitude flight and introduced a higher level of internal oversight. Additionally, it embarked upon a dedicated safety management system.
BC Hydro
As a result of the accident, BC Hydro immediately suspended all helicopter operations to allow time to develop policies and associated procedures concerning the use of helicopters. In June 2008, an interim policy was set forth and, in summary, required company users to:
- justify the use of a helicopter;
- select the appropriate helicopter; and
- obtain senior management approval for each helicopter flight request.
The intent of this policy is to ensure that the associated risks are identified and managed in advance, and that only necessary flights are arranged and approved. The policy and procedures were provisional in nature, pending the development and implementation of a more extensive helicopter management system.
BC Hydro also engaged an international aviation risk management company to carry out a risk assessment of all BC Hydro flight profiles. In turn, it has developed a framework for a helicopter management system, which incorporated hazard identification and mitigation, vendor selection and audits, helicopter selection criteria, standard operating procedures, and associated training. Subsequently, BC Hydro engaged a Canadian aviation consultant to guide its efforts in implementing that system.
In the meantime, BC Hydro implemented an interim company policy of requiring twin-engine helicopters for those at-risk operations where a single-engine helicopter would have been required to operate inside the avoid areas of the height velocity diagram (HVD). Single-engine helicopters continue to be used in power line patrol operations, but those flights are specifically prohibited from operating inside the avoid areas of the HVD. Furthermore, BC Hydro is exploring the use of recent technology — such as Lidar and very high quality imaging systems — that allow the collection of detailed data from helicopters operating outside the height-velocity envelope and without passengers on board.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .