Loss of Control - Collision with Terrain
Quantum Helicopters Ltd.
Bell 206L (Helicopter) C-FRCL
Legate Creek, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Bell 206L (LongRanger) helicopter (serial number 45019, registration C-FRCL) was being operated by Quantum Helicopters Limited at Legate Creek, just north of Terrace, British Columbia. At about 1030 Pacific daylight time, the pilot started long-line operations to move a drill rig at about 4200 feet above sea level on a steep hillside. The first and second lifts were completed uneventfully. Upon lifting the third load, the helicopter descended into the valley before it climbed slowly. It needed two orbits to climb to a sufficient height to make its approach to the landing area. When the load was about three feet above the drill deck, the helicopter descended rapidly and the load came down hard. While the ground crew attempted to unhook the load, it popped back into the air. The load slammed onto the deck again and the helicopter fishtailed. The load was abruptly lifted back into the air once again and the helicopter began to spin with its tail bent. The load remained attached to the helicopter and became lodged in trees. Tethered by the long-line, the spinning helicopter descended in an arc and crashed into the cliff. It ended up hanging inverted. The pilot was critically injured and died of his injuries the next day. There was no fire. The emergency locator transmitter broke out of its mount and was ejected from the helicopter, where it emitted a signal for about 15 hours.
Other Factual Information
The weather in the area on the day of the accident was cloudy with rain showers, calm winds, and a temperature of about 12°C.
The accident site was initially observed by helicopter. The tail section was separated from the main wreckage, with many pieces strewn about the hillside, some above and some below the main wreckage (see Photo 1). The wreckage was recovered and transported to an examination facility.

The tail boom showed evidence of being struck by the main rotors at least twice and was broken into four major pieces. The break surfaces were consistent with overload fractures and none showed evidence of reverse bending.
The forward break showed damage that was consistent with the tail boom being bent to starboard. Scarring from the main rotor strike showed the section was bent to about 80°. A dent on the horizontal stabilizer's port vertical fin indicated the elevator was full up when it was hit, which is consistent with a pilot input of full aft cyclic. There was a dent in the tail rotor pitch control rod that indicates there was full right pedal at the time of impact. The main rotor blades were broken off about three feet from their roots. One blade was swept back in its grip and the latch bolt was broken by overload forces. The deck that supports the hydraulic servos and the main rotor transmission had separated from the roof. All of the breaks on the deck and the deck support were from overload. The wreckage showed damage consistent with high engine power at impact.
The helicopter was modified with a Rolls Royce 250 C20R engine (STC #SH4169NM) that allowed sustained performance to a higher density altitude. A tear-down examination of the engine and its accessories revealed no anomalies, except in the power turbine governor (PTG) and fuel control unit (FCU). The PTG and FCU were tested and did not perform at their optimum level. However, the engine manufacturer indicated that the engine would perform without apparent problems at the density altitude at the time of the accident.
New main rotor blades were installed 36 flying hours before the accident flight. An examination of the helicopter controls showed no pre-impact breaks. The hydraulic servos were checked and no anomalies were found.
"Collective Bounce" is a divergent vertical motion of the helicopter amplified by the pilot's left arm moving the collective. This phenomenon can occur when the resonance of the blades matches that of the long-line slung load and collective movements to correct this get out of phase, due to the response lag. The helicopter can self-destruct by about the fifth bounce.
Examination of the pilot collective showed that the pilot adjustable friction lock had been set to remove all friction Footnote 1. The built-in collective friction is required to be set by maintenance personnel at between 4.0 to 4.5 pounds. This friction was found to be about two pounds. The manufacturer's maintenance manual requires this built-in friction to be checked every 100 hours. The company's maintenance records show that the last 100-hour inspection was carried out 21 flight hours prior to the accident. There was no evidence to suggest the collective friction was adjusted. The helicopter manufacturer issued an Operations Safety Notice (OSN-GEN-76-6) on 18 October 1976 reminding operators that minimum prescribed friction is necessary to preclude collective bounce by "reducing the effect of pilot over-control; reducing effects of wind gusts and turbulence through rotor to the airframe; and preventing feedback from external sling loads into the airframe."
The electrical external cargo release was checked and functioned properly. The manual/emergency release mechanism was also checked and was found to have an accumulation of rust, impairing its operation. Because this check was carried out six weeks after the accident, it could not be determined if the rust that was found in the mechanism was present at the time of the accident. Both of these releases operated the belly hook.
The operation was being carried out with a Canam 100-foot Plasma long-line (7/16-inch diameter) rated for 3000 pounds. This long-line was tested and showed that it stretched about one foot with a 1500 pound load, and contracted that same amount when the load was removed and the line manually agitated. Tests on a new 7/16-inch Canam Plasma long-line showed similar characteristics. Other pilots confirmed these observations where loads were reported to bounce when using this type of long-line. Using a 9/16-inch diameter long-line was said to eliminate the bounce. This is consistent with tests on a similar line where a 1500-pound load caused minimal stretch.
The long-line had a heavy-duty swivel, but there was no mechanism for the pilot to release the load at the lower end of the long-line. The load was attached to the long-line with a gated hook which was normally unhooked by the drill crew on the ground. Except in an emergency, the helicopter's belly hook release is not normally used. There was no evidence to suggest that an emergency release was attempted.
The pilot's door had been removed prior to the accident flight so he could lean out to see the load. This is commonly known as vertical reference flying.
The pilot was very experienced on the type of helicopter and the work being carried out. He had about 11 500 flight hours in total and about 7500 hours on type. He was the chief pilot and part owner of the company. He was appropriately trained, qualified, and certificated for the flight in accordance with existing regulations. His flight and duty times for the weeks before the accident were not excessive and were within the regulatory standards prescribed. As is typical with many pilots involved in vertical reference flying, the pilot did not use the shoulder restraint system provided. The pilot was wearing a flight helmet.
For a tail rotor control failure where there is a complete loss of thrust, the emergency procedures section of the approved aircraft flight manual (AFM) calls for the pilot to first reduce the throttle to flight idle. However, it notes that when a suitable landing site is not available, the large vertical fin may permit controlled flight at low power levels and sufficient airspeed.
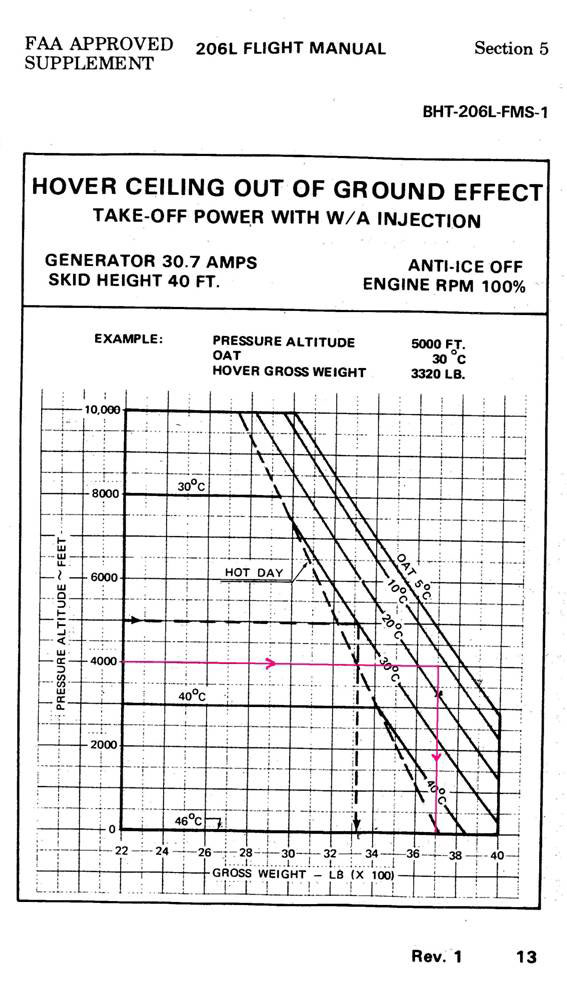
At the start of the drill move operation, the configuration of the helicopter allowed for a payload of about 1300 pounds. The third load was a hydraulic power unit and, according to its manufacturer's brochure, it should weigh 1225 pounds dry. The helicopter's maximum gross weight is 4000 pounds After adding the weight of the rigging and the long-line, the estimated gross weight of the helicopter with its load should have been a little less than 4000 pounds After the accident, the load with the rigging was recovered and the weight was recorded to be 1550 pounds, increasing the helicopter's gross weight to about 4235 pounds. According to the AFM, the helicopter's ability to hover out-of-ground-effect (HOGE) was limited to a gross weight of approximately 3700 pounds, assuming the engine was operating normally (see Appendix A – B206L HOGE Chart). The gross weight was estimated to be 535 pounds heavier.
Analysis
Because there was no evidence of progressive failure or weather related problems, this analysis will focus on helicopter operations and systems.
The hard landing of the load is consistent with the helicopter sinking rapidly as it slowed and due to limited performance as predicted in the HOGE chart.
The pilot may have attempted to correct a nose-down pitch if the helicopter was forward of the load when a large collective input was made. This would explain why there were indications that the cyclic was in the full aft position.
The main rotor blades struck the tail boom in a flight regime (hover) where contact is highly unlikely. The deck support did not break as an initiating factor, and because the tail boom did not break before it was hit, there had to be some other abnormal event to bring the main rotor in contact with the tail boom.
There are a limited number of events that can cause a main rotor to strike the tail boom, but only collective bounce is able to generate the divergence necessary to bring this about under the accident circumstances:
- The drop of the load (three feet) onto the drill deck would initiate a bounce.
- The pilot was leaning out the right door with his left arm extended fully to reach the collective stick (susceptible to an uncommanded movement from a bounce).
- While the lack of built-in friction could have been mitigated by the pilot applying friction, this was not done and the collective did not serve to help dampen the pilot's arm movement after the initiating bounce.
- The long-line stretch aggravated vertical movement of the load (bounce).
- The main rotor blade was flexing down when the helicopter was hovering (divergent vertical movement).
- Although the load was very heavy for the helicopter, it dropped and rose quite quickly (disproportionate to the normal collective movement), indicating uncommanded power changes.
Therefore, collective bounce likely caused the main rotor to strike the tail boom, probably in the early stages of the divergent vertical movements.
When the tail boom was struck, the drive to and control of the tail rotor was lost and the helicopter began to spin to the right. While the pilot would have applied left pedal to try to stop the spinning, it would have no effect. Another way to stop a helicopter from spinning about its yaw axis is to reduce throttle, which was not done. A third way is to get air flow across the vertical stabilizer, weathercocking the airframe. This can be accomplished by getting forward speed, and the pilot may have been attempting to do this as he headed toward the cliff just before the external load lodged in the trees. It is also possible that the helicopter's movement toward the cliff was due to the change in the center of gravity when the tail was displaced and the climb was part of the collective bounce. In either case, the pilot lost control of the helicopter.
It was not determined why the pilot did not release the external load. However, two possibilities exist: he may not have tried the main (belly) hook electrical release, or the angles and load on the hook prevented it from opening. It is unlikely the pilot would have let go of the collective stick to pull the manual/emergency hook release because he was being centrifuged out the door. If he had, he may have found that mechanism not functioning properly.
The right pedal input at impact may be explained by the pilot's attempt to get his upper body back inside the helicopter as it spun. He may have pushed his foot on the right pedal to counter the centrifugal forces of the spin.
There is an increased risk of injury in the event of an accident when the pilot's upper body is unrestrained. This is compounded by the removal of the door. In this case, the helicopter struck the cliff inverted and on the pilot's side. Even if the pilot was able to pull himself inside the helicopter, because the door was removed, there was nothing to stop his upper body and head from striking the rocks, or being squeezed in the door frame.
Review of the Bell 206L performance charts, available in the AFM and supplements, indicated that the helicopter would not hover out-of-ground-effect with the load it was carrying. While most helicopter flight manuals contain these charts, they are often not included in the limitations section and can, therefore, be interpreted as guidance material. There is a risk that not adhering to these performance charts will result in damage to the helicopter, loss of control, or both.
Findings
Findings as to causes and contributing factors
- The helicopter was operating at a weight that, when forward speed was reduced, caused it to descend rapidly and the load to hit the drill deck hard. The hard landing of the load, combined with the pilot's body position, long-line stretch, and low collective friction initiated collective bounce, causing the main rotor blades to strike the tail boom.
- The tail rotor drive and anti-torque control were lost, causing the helicopter to spin about its yaw axis due to high engine torque; the pilot lost control and the helicopter collided with terrain.
- Long-lines that stretch have been known to induce vertical oscillations and there is a risk of these oscillations accelerating to a point beyond pilots' control.
- While most helicopter flight manuals contain performance charts, they are often not included in the limitations section and can, therefore, be interpreted as guidance material. There is a risk that not adhering to these performance charts will result in damage to the helicopter, loss of control, or both.
- Operating with an unrestrained upper body and without a door increases the risk of injury in the event of an accident.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on
Appendices