Collision with water
Government of Canada, Department of Transport
MBB BO 105 S CDN-BS-4 (helicopter) C-GCFU
M’Clure Strait, Northwest Territories
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 09 September 2013, at 1638 Mountain Daylight Time, the Canadian Coast Guard Messerschmitt-Bölkow-Blohm BO 105 S CDN-BS-4 helicopter (registration C-GCFU, serial number S 727) operated by the Government of Canada, Department of Transport, call sign CCG364, took off from the Canadian Coast Guard Ship (CCGS) Amundsen with 1 pilot, the vessel's master and a scientist on board for a combined ice measurement and reconnaissance mission in the M'Clure Strait, Northwest Territories.
At 1738, CCG364 informed the CCGS Amundsen that it would be arriving in 10 minutes. When the helicopter had not arrived, its position was checked on the flight following system at 1805, which was displaying the helicopter's position as 3.2 nautical miles from the vessel. Starting at 1818, the CCGS Amundsen's crew attempted several times to communicate by radio with the pilot, without success. At 1824, the vessel proceeded toward the helicopter's last position displayed on the flight following system. At 1847, debris was spotted. The 3 occupants were recovered using the vessel's fast rescue craft; none of them survived. The helicopter sank in 458 m of water. The accident occurred during daylight. No 406-MHz emergency locator transmitter signal was received by the satellite system.
1.0 Factual information
1.1 History of the flight
The Government of Canada, Department of Transport,Footnote 1 helicopter pilot was assigned to shipboard duties and boarded the Canadian Coast Guard Ship (CCGS) Amundsen in Resolute Bay, Nunavut, on 05 September 2013, for a 42-day assignment. That day, the pilot flew 4.7 hours, taking off and landing 34 times to effect the vessel's scheduled crew change.
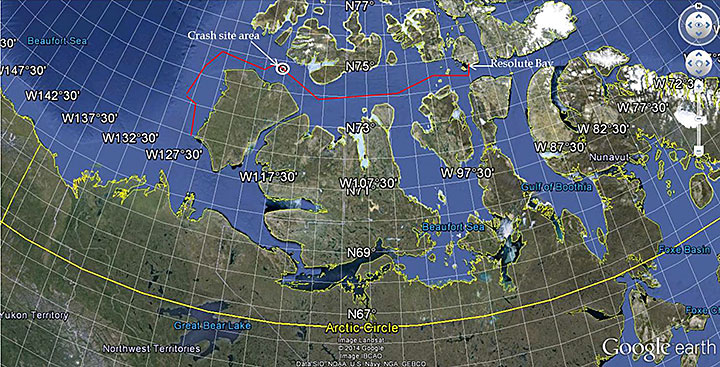
The following day, the CCGS Amundsen departed its anchorage at Resolute Bay with 73 people on board for the second leg of the ArcticNet Beaufort Regional Environmental Assessment (BREA) research program.Footnote 2 The planned route for this portion of the second leg was to continue westbound along the northern shore of Banks Island, Northwest Territories, and then descend along the western coast of the island to perform the next scientific research activities (Figure 1).
In preparation for a flight on 08 September 2013, the helicopter was refuelled with 66 gallons, which brought the total fuel quantity to 125 U.S. gallons.Footnote 3 This flight was to take place with the pilot, a scientist and the CCGS Amundsen's master on board. It is unknown if the pilot knew before refuelling that the master would be on board the flight. However, the flight was cancelled due to an inoperative igniter box on the No. 1 engine. The igniter box was replaced and the aircraft was returned to service.
On the following day, 09 September 2013, at 1638,Footnote 4 flight CCG364 took off from the CCGS Amundsen with the pilot, the master and a scientist on board. The scientist, seated in the passenger seat on the left, was equippedFootnote 5 to conduct ice thickness measurements. The master, seated behind the scientist, was on board to conduct an ice reconnaissance mission in order to determine the CCGS Amundsen's best route to the next scientific station located west of Banks Island. Northerly winds had moved the ice to the southern portion of M'Clure Strait, resulting in close- to very close-pack old iceFootnote 6 along the western north shore of Banks Island. An ice service specialistFootnote 7 is normally on board Canadian Coast Guard (CCG) vessels assigned to most arctic operations, including scientific missions. However, there was none for this mission.
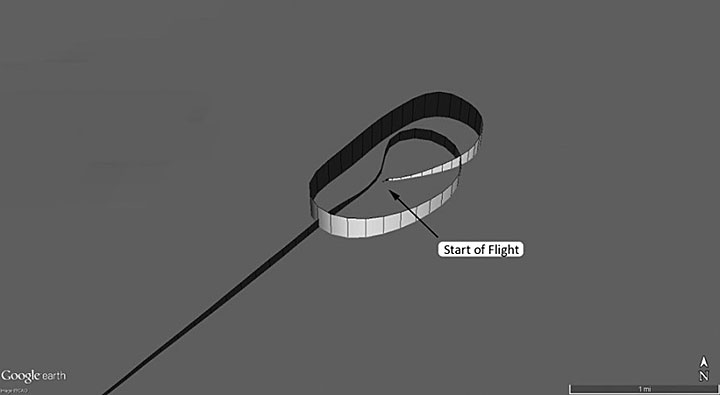
The flight consisted of 3 legs flown in a triangular pattern. The flight track data of the occurrence flight was extracted from the onboard flight following and satellite communications systemFootnote 8 recovered with the wreckage. The data shows that, upon departure off the vessel, the helicopter climbed while orbiting to approximately 1500 feet above sea levelFootnote 9 (asl) before descending to the altitude used to carry out the ice measurement survey—approximately 20 feet above the surface of the ice—as it proceeded southwest for about 24 minutes (Figure 2). Two survey runs were conducted during this first leg.
At about 20 nautical miles (nm) from the vessel, the helicopter turned northwest for the second leg, during which 2 other survey runs were carried out (Figure 3).
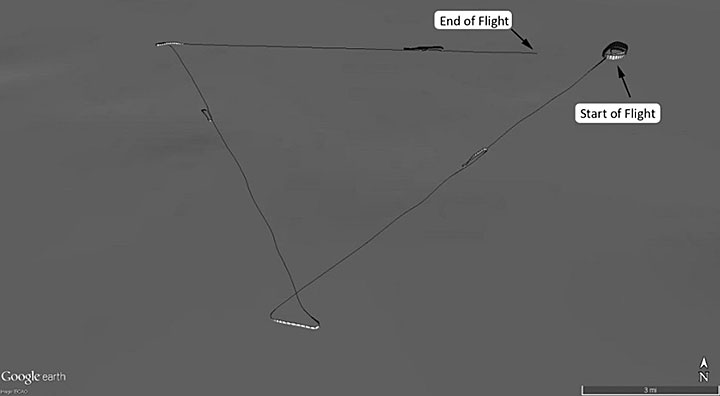
At 1724, approximately 20 nm from the vessel, and while heading eastbound for the third leg, the helicopter made a descent from about 500 feet asl and levelled off at the survey altitude, where it remained for a period of about 9 minutes.Footnote 10 The helicopter then made a climbing left turn southwest bound, followed by a right descending turn eastbound to about 40 feet before making another left climbing turn to reach approximately 550 feet at 1737:34.
At 1738:14, CCG364 called the CCGS Amundsen to report that its estimated time of arrival (ETA) was in 10 minutes. At that time, the helicopter was in descent at approximately 390 feet. That was the last recorded message from the pilot. The helicopter continued its descent toward the survey altitude and levelled off at 36 feet at 1739:19, while eastbound. For a period of 3 minutes and 30 seconds, the helicopter maintained an altitude varying between 23 and 39 feet.Footnote 11 Footnote 12 It then made a slow descent for 13 seconds before colliding with water at 1743:02. The 3 occupants evacuated the helicopter before it sank to the sea floor 458 m below (approximate position: 74°45′49" N, 117°43′56" W).
1.1.1 Recovery of occupants
At 1805, 27 minutes after CCG364′s last broadcast, the helicopter's position was checked on the flight following system's (FFS) control display unit (CDU) located in the wheelhouse. The FFS CDU indicated that the helicopter was at a distance of 3.2 nm, on a bearing of 287° true from the vessel. The last and only displayed position available to the crew in the wheelhouse was on the FFS CDU as N 74° 45.56, W 117° 49.52Footnote 13 at 1741. SeveralFootnote 14 attempts to establish contact with CCG364 were then made, to no avail.
At 1824, the decision was made to proceed toward the helicopter's last displayed position. However, due to ice conditions, the vessel could not proceed direct. At 1841, the Trenton Joint Rescue Coordination Centre (JRCC) was informed of the situation.
At 1847, some floating debris was spotted. Six minutes later, the vessel was stopped and a fast rescue craft (FRC) with 4 rescuers on board was lowered from it to proceed toward the observed debris.
At 1854, 2 of the 3 occupants were located and found to be floating and unresponsive. They were brought on board the FRCFootnote 15 and were showing signs of drowning.Footnote 16 No vital signs were observed. The FRC returned to the vessel and transferred the 2 occupants at 1905 since the third occupant could not be located.
From 1904 to 1907, the CCGS Amundsen made 3 mayday calls,Footnote 17 to no avail.
At 1907, the third occupant was located floating, also unresponsive, and was brought on board the FRC showing signs of drowning and no vital signs.
At 1909, the CCGS Amundsen phoned Trenton JRCC to request support for a medical evacuation. The closest military air asset, a C130, was in Winnipeg, Manitoba, about 1582 nm away, while the closest marine asset, the CCGS Henry Larsen, was in Resolute Bay, Nunavut, about 345 nm away. While looking for the most appropriate and expeditious air asset, the CCGS Henry Larsen was tasked to proceed toward the accident site while the CCGS Amundsen was heading in the opposite direction for a rendezvous. The plan was then to use the CCGS Henry Larsen's helicopter to conduct the medical evacuation.
At 2008, the requested support for the medical evacuation was cancelled since the 3 occupants were deceased.
1.2 Injuries to persons
| Injury | Crew | Passengers | Others | Total |
|---|---|---|---|---|
| Fatal | 1 | 2 | – | 3 |
| Serious | – | – | – | – |
| Minor/None | – | – | – | – |
| Total | 1 | 2 | – | 3 |
1.3 Damage to aircraft
The helicopter was substantially damaged on impact with the surface of the water. There was severe upper frontal damage of the windshield and instrument panel. The tail boom was separated near the front of the tail boom and 3 main rotor blades had been torn off at their roots (Photo 1).

1.4 Other damage
There was an estimated 79 U.S. gallons of fuel remaining at the time of the impact. Approximately 105 gallons of water and fuel were recovered from the helicopter's fuel tank; no fuel in any measureable quantity was known to have escaped. Approximately 1 litre of synthetic turbine oil (BP 2389, MIL-PRF-7808G) escaped from the 2 accessory gearboxes,Footnote 18 and approximately 4 litres escaped from the No. 2 engine oil tank.Footnote 19
1.5 Personnel information
The pilot was certified and qualified for the flight in accordance with existing regulations, and held a valid Canadian airline transport pilot licence - helicopter, with type ratings on the BH06, BH12, BH47, HU50, S313, S318, S342 and MBH5.Footnote 20 The licence was endorsed with a group 4 instrument rating, which was valid until 01 December 2014.
The pilot had joined Transport Canada (TC) in 1985, and had accumulated a total of 10 218 hours of flight time, including a total of 3910 hours on multi-engine helicopters, mostly as pilot in command. The pilot was certified on the MBH5 in 1987, and had since accumulated approximately 3100 hours on type. According to the pilot's training records, the last pilot proficiency check on the MBH5 was conducted on 28 November 2012 and was valid until 01 January 2014. The pilot completed underwater egress training on 28 September 2011, which was valid until 01 October 2014. The pilot's exact experience related to ice measurement missions with the ice-probe installation is unknown, but while flying Coast Guard operations, the pilot completed several over-water flights and ice patrols. According to the pilot's log book, the last ice measurement mission with the ice-probe was in 2010.
The pilot's flight and duty time limits were not exceeded. In the days prior to the occurrence, the pilot flew 4.7 hours on 05 September 2013. Nothing indicates that the pilot had been assigned to tasks other than flying while on board the vessel that could have caused fatigue. On the day of the occurrence, no signs of unusual behaviour or fatigue were observed.
1.6 Aircraft information
1.6.1 General
The Messerschmitt-Bölkow-Blohm (MBB) BO 105 S CDN-BS-4 is a light, twin-engine, multi-purpose helicopter developed by Bölkow in Munich, Germany. MBB became a part of Eurocopter in 1992 and was renamed Airbus Helicopters Deutschland GmbH in 2014. The BO 105 production continued until 2001. A total of 1407 BO 105s have been manufactured, of which 660 are still in service, and have accumulated a total of 8 million flight hours collectively.
The accident helicopter was manufactured in 1985, and was powered by 2 Rolls-Royce 250 C20B engines, developing 420 shaft horsepower (SHP) each. There was no data in the TSB's Aviation Safety Information System (ASIS) indicating that the helicopter had been involved in an accident prior to this occurrence. The helicopter was maintained by Transport Canada Aircraft Services Directorate (ASD) maintenance personnel and flown by TC ASD pilots. Records indicate that the aircraft was certified and equipped in accordance with existing regulations. The helicopter's weight and centre of gravity were within the manufacturer's prescribed limits at the time of the occurrence.
The helicopter had flown about 8866 total hours, including 2095 hours since the completion of the last scheduled major airframe inspection (OPS 4) on 16 May 2007. It had undergone a 100-hour inspection on 10 April 2013, about 91 flight hours before the accident flight. The helicopter's technical records did not indicate any outstanding or recurring maintenance issues.
The CCG, through TC ASD, uses the BO 105 for various tasks, which may include re-supply of vessels, light stations, and other remote sites; aids to navigation, search and rescue (SAR); and other duties related to Fisheries and Oceans Canada and CCG programs.
1.6.2 Flight following system on board
The helicopter was equipped with a flight following and satellite communications system manufactured by SkyTracFootnote 21 (model ISAT-200R, serial number 30267). This system is not required by TC regulation and is considered additional flight safety enhancement equipment. The ISAT-200R provides automatic, global, and real-time flight following, text messaging, data transfer, and satellite phone capabilities. The ISAT-200R was recovered with the wreckage and sent to the TSB laboratory to extract its data. The extracted data provided information such as time, latitude, longitude, heading, ground speed, and altitude, all recorded at 5-second intervals.
The data showed that the helicopter carried out a total of 6 survey runs flown at low altitudeFootnote 22 for periods ranging from approximately 7 to 9 minutes, except for the last run that ended in the impact, which lasted about 3 minutes. In total, during the 65-minute flight, the pilot spent approximately 43 minutes, or 66% of the air time, flying survey runs between 13 and 30 feet above the surface.
The data showed that just prior to the accident, at 1739:19, the helicopter had levelled off at 36 feet while eastbound and maintained an altitude varying between 23 and 39 feetFootnote 23 until 1742:49. The average ground speed during this period was 67 knots. The aircraft then descended slowly until it collided with the water. The data showed a ground speed of 68 knots and an altitude of 3 feet at 1743:02, the time of the last recorded data. The descent for the last 13 seconds of flight corresponds to a rate of 166 feet per minute.
1.6.3 Emergency flotation system
The helicopter was equipped with a flotation systemFootnote 24 designed to enable an emergency water landing and to keep the helicopter afloat. The floats can be deployed in flight at altitudes of 3000 feet or less and at airspeeds of 80 knots or less. Once deployed, the airspeed is limited to a maximum of 100 knots. The flotation system consists of a left-hand and right-hand float subsystem attached to the helicopter's skids (Figure 4).
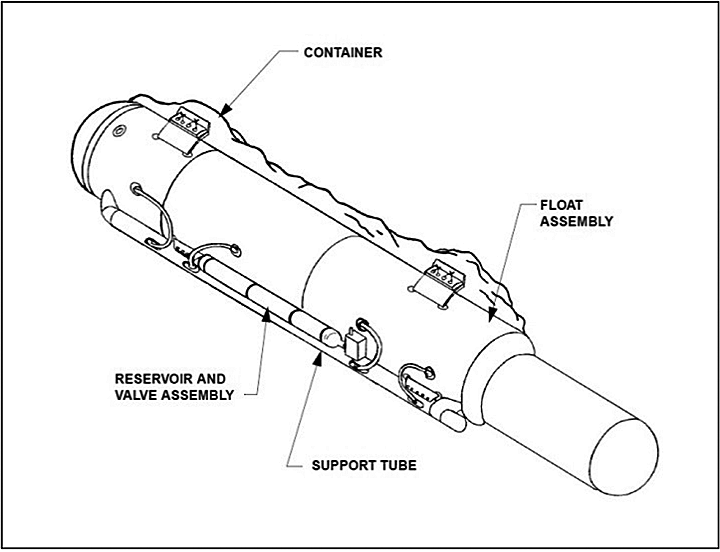
Both float subsystems remained attached to the helicopter during the accident sequence and were found within their respective containers. Both reservoirs that store nitrogen were charged within the manufacturer's specification. With the exception of damage related to impact and water submersion, no anomalies or pre-existing defects were noted that would have prevented the flotation system from operating normally. There was no indication that the flotation system was activated prior to or at the time of the impact. A review of the maintenance records indicated that both float subsystem assemblies were maintained in accordance with the manufacturer's recommendations and had no outstanding maintenance issues at the time of the accident.
1.6.4 Emergency locator transmitter
The helicopter was not equipped with an automatically deployable emergency locator transmitter (ELT), nor was it required to be by regulation. However, it was equipped with a fixed ELT 406 MHz, manufactured by Artex Aircraft Supplies Inc. (model C406-2HM, part number 453-5001 Rev. M, serial number 170-08846). The ELT was found attached to the right side of the fuselage in the rear cargo section and was recovered for examination. An ELT is activated automatically by impact forces or manually via the remote activation switch located in the cockpit. In this occurrence, both the switch on the ELT and the remote activation switch were found in the armed position.
The 406-MHz ELT on the occurrence helicopter was designed to transmit a 406-MHz signal for 440 to 520 milliseconds, repeating every 47.5 to 52.5 seconds. However, the first transmission after activation is deliberately delayed for 50 seconds in order to prevent false alarms that can occur during routine ELT maintenance activities. While the delay helps to ensure that the signal received by the COSPAS-SARSAT satellite system is a legitimate distress signal, this delay may prevent the broadcast of an actual distress signal in a ditching scenario if the aircraft submerges before a signal is emitted. In addition, in rotorcraft accidents, there tends to be considerable uncertainty in the attitude of the aircraft at the moment of impact. In this occurrence, no signal was received by COSPAS-SARSAT satellite system.
Many of these issues are being addressed in a joint Results Through Collaboration in Aviation (RTCA) and European Organisation for Civil Aviation Equipment (EUROCAE) committee on the next generation of 406-MHz ELT. The committee is creating standards for automatically triggering an ELT based on abnormal flight data prior to crashing. The ELT would start to transmit a signal at an accelerated rate almost immediately upon activation, and continue to transmit a signal numerous times in the first minutes of operation. These features would meet the requirements of the International Civil Aviation Organization (ICAO) Global Aeronautical Distress and Safety System (GADSS) for autonomous distress tracking scheduled for 2021.
Examination of the ELT showed that water had filled the unit, likely due to the water pressure at the depth from which the aircraft was recovered. The internal circuitry was corroded and the lithium batteries had leaked. Therefore, it was not possible to test the ELT as the internal electronic components were too badly damaged by corrosion. It could not be determined if the ELT activated following the impact. Even if it had activated, the signal would have been attenuated once submerged. It is likely that the helicopter sank before a 406-MHz signal could be transmitted.
1.6.5 Underwater locator beacon
The helicopter was equipped with a Dukane model DK-100 (serial number DV12562) underwater locator beacon (ULB). The ULB is designed to activate upon immersion and to transmit an acoustic signal at 37.5 kHz. This signal propagates well in water and is normally easily detected using portable hydrophone detection equipment. During the search for the recovery of the helicopter, a hydrophone search for the ULB was carried out, but a steady and consistent beacon signal could not be detected. A test ULB was lowered into the water and the beacon was easily detectable.
The ULB from the accident helicopter was initially examined and tested at the TSB laboratory. It was further examined and tested under TSB supervision at the manufacturer's facilityFootnote 25 to determine what would cause it to perform sporadically, as during the search and recovery operations. The reason the signal was not consistently received during the search and recovery operations could not be determined. There was no evidence of any damage or water ingress into the unit. There was sufficient battery power available to allow the unit to perform as designed and, once activated, the ULB produced a continuously repeating transmission that was on frequency in all temperatures and pressures tested. However, once cooled, it was noted that there was a tapered shape to the output pulse. This would have resulted in a reduced output power for a portion of the pulse and may have affected the effective range of the unit, but it would not have produced the intermittent performance as noted by the investigators during the wreckage search.
1.6.6 Seats and safety harnesses
Each front seat was longitudinally adjustable and equipped with a 4-point safety harness consisting of a lap belt and automatic locking shoulder harnesses (Photo 2). The 3-person fixed-position rear bench seat was equipped with a 3-point safety harness for each seat, the shoulder harness was not an automatic locking type. The design of the front and rear seat belt system was such that the seat belt buckle latch had to be raised to insert the metal tongues on the lap belt and shoulder straps. Closing the buckle latch locked the 4 belts together. Lifting the buckle latch released the seat belt system.

When the helicopter was recovered, it was noted that all of the occupants' seat harnesses were released. There was no indication that any of the lap belt or shoulder harness tongues had been forced from the buckle assembly. Examination of occupants' safety harnesses did not identify any discrepancies that would have prevented normal operation.
The pilot's seat had been pushed back to the end of the right (outboard) rail and slightly short of the left rail end. The seat frame was deformed and buckled in a way that was consistent with the back having been forced backward. These observations suggest that a backward force had been applied to the upper body of the occupant and transmitted to the back of the seat. The left front seat was found secured with no sign that it had been displaced during the occurrence. No deformation of the seat frame was observed. The absence of significant damage to the left front seat suggests it had not been exposed to the same rapid ingress of water that the pilot's seat had. The rear bench seat's left supporting strut had fractured and was deformed forward. It is considered likely, therefore, that the left-front vertical strut fractured due to the dynamic loading caused by the vertical deceleration of the occupant at the time of impact.
1.6.7 Video camera pod and movie camera system
The helicopter was equipped with a video camera pod (video pod). The installation of the video pod was approved in accordance with Aircraft Services Service Bulletin (ASSB) 351-0177. The ASSB allowed for a video pod to be installed on either or both side boarding steps, attached to the skid gear. Typically, the video pod would be installed on the left boarding step and its cables would be routed through a modified window panel installed in the left rear door. When the ice probe system was also installed, the video pod cables and ice probe cables would be fastened together, and all of them would be routed through the same modified window panel in the left rear door.
In August 2013, the occurrence helicopter had been configured to allow for a movie camera system to be installed on the left skid gear in accordance with supplemental type certificate (STC) 0-LSH10-188.Footnote 26 Due to the design of the movie camera system,Footnote 27 it was not possible to install both the movie camera and a video pod on the left skid gear at the same time. On the day of the occurrence, the movie camera was not installed and the left boarding step had been replaced by the movie camera support tube, but since moving the video pod from one side to the other involves considerable work, it was decided to leave the video pod on the right side even if the movie camera was not in place on the left skid gear.
1.6.8 Ice survey system
1.6.8.1 General description
The helicopter was equipped with an ice survey system, which included a forward-facing boom (ice probe), a computer system, and interconnecting cables. The ice probe, which housed a laser altimeter and sensors for measuring the depth of snow and ice, was attached to the nose of the helicopter (Photo 3). The computer system connected to the ice probe was retained in the rear seat and recovered with the wreckage. Only pieces of the ice probe were recovered; none of the housed equipment was retrieved.

The modification pertaining to the installation of the ice survey system was approved in accordance with JCM Aerodesign Limited's STC SH01-4,Footnote 28 and the system had been installed on the CCG BO 105 since 2001. STC SH01-4 references the following documents:
- Drawing JCM-003011 revision nc dated 10 January 2001;
- Flight Manual Supplement (FMS) No. 003011FMS dated 02 February 2001.
Drawing JCM-003011 revision nc includes information pertaining to the installation of the boom and its supporting tube assemblies. FMS No. 003011FMS includes the mandatory operating limitations, a section that provides a general description of the modification, and a photograph showing the routing of the interconnecting cables.
On 05 February 2001, ASD issued ASSB 351-0262, “Installation of JCM Aerodesign Ice Probe per STC SH01-4,” as a cover document to the STC. This method is used to track STCs in ASD's maintenance program.
1.6.8.2 Ice probe installation
Test flights were carried out as part of the STC process. To obtain the flight test permit, JCM Aerodesign Limited developed a report that described how the helicopter was to be configured for the test flights and included photographs of the cable routing. The initial installation of the ice probe system, which included the routing of the cables, was carried out by ASD on a CCG helicopter. In accordance with the report, the cables were routed along the left side of the fuselage during the test flights. No test flights were carried out with the cables routed along the right side of the fuselage. The STC holder documented the installation details and conveyed this information in the form of Maintenance Manual Supplement (MMS) No. 003011MMS (26 March 2008). The MMS was developed to satisfy the requirements of Federal Aviation Regulation (FAR) 27.1529 (Amdt. 27-3, Eff. 10/17/68), pertaining to the Rotorcraft Maintenance Manual requirement.
The documentation pertaining to the installation of the cables that was available to ASD maintenance personnel included
- FMS No. 003011FMS;
- MMS No. 003011MMS;
- JCM Aerodesign Report No. 003011D (Technical Description); and
- EISFlow™ Installation and Operations Manual.
All of these documents include photographs showing the cables routed along the left side of the fuselage. However, none of them state that cables must be installed on the left side, and none contain a note or warning prohibiting the installation on the right side.
Since 2001, ASD had been installing the ice probe cables along the left side of the helicopter in accordance with the photographs in the numerous documents. ASD has no record of the cables being installed in any other manner, nor was there any request made to deviate from the routing indicated in the photographs. No safety reports relating to the installation of the ice probe system have been recorded in ASD's safety reporting database.
1.6.8.3 Ice probe installation on the day of the occurrence
During the first use of both the ice probe and the video pod after the reconfiguration to allow for the movie camera system to be installed on the left skid in August 2013, it was decided that the ice probe cables would be routed along the right side of the fuselage. Although there were no published instructions for routing the cables in this manner, ASD maintenance personnel positioned the cables such that the routing was similar to the routing used on the left side. In doing so, the cable bundle was routed above the right side static port and Pitot tube (Photo 4).

During the first flight with the cables installed in this manner, erroneous airspeed indications were noted. The helicopter returned to the vessel and landed without further incident. ASD maintenance personnel concluded that the location of the cable bundle was likely interfering with the airflow in the area of the Pitot tube and static port, resulting in the erroneous airspeed readings. It could not be determined if the altimeter was also affected by the discrepancy.
The cable bundle was then re-routed along the lower right side of the fuselage, below the Pitot tube and the static port. During subsequent flights, there were no indications of erroneous airspeed indications. There was no record made in the journey log for either the change in cable routing or for the erroneous airspeed indications experienced during the first flight. Additionally, ASD had no record of a modification proposal for the change in cable routing.
When the occurrence ASD maintenance personnel arrived on the ship, the ice probe had been removed but the cables were still installed along the lower right side of the fuselage, below the Pitot tube and the static port. During this ASD maintenance personnel's first installation of the ice probe and video pod, the cables were removed from the right side and re-installed on the left side so that they were installed in accordance with MMS No. 003011MMS and the supplied photographs. ASD maintenance personnel were then made aware of the previous changes to the video pod and advised that the cables had been installed on the right side to accommodate these changes. On 08 September 2013, the cables were removed from the left side and reinstalled on the right side, routed in a manner that was similar to the previous right side installation. The ice probe cable bundle, with a diameter of approximately 4 cm, was routed about 6 cm above the static port and secured in place by multiple layers of heavy grey tape instead of going through Adel clamps as shown in Photo 4. A record of the cables and video pod being installed along the right side was made in the aircraft journey log.
After the helicopter was recovered, it was noted that the cables had been torn away from the boom and were no longer held in place by the multiple layers of tape. This most probably happened during the impact sequence. The cables were still routed through the right rear door; however, the door had separated from the helicopter.
During the occurrence flight, the cables had been routed in a manner similar to the first installation along the right side of the helicopter in which erroneous airspeed indications were observed. It was not possible to determine if the airspeed indications were accurate during the occurrence flight.
1.7 Meteorological information
1.7.1 Introduction
The following meteorological information is a summary of a meteorological analysis report prepared by Environment Canada.
1.7.2 Aviation weather
On 09 September 2013, the western portions of the Canadian Arctic Archipelago were under the influence of a stationary ridge of high pressure extending from a broad area of high pressure centred near 80°N 118°W towards 70°N 098°W. The lower levels of the atmosphere were covered with multiple layers of cloud across the area including Banks, Prince Patrick, Victoria and Melville islands.
There are a limited number of aerodrome routine meteorological reports (METAR) from the Canadian Arctic Archipelago that include reports of sky condition (cloud heights and amounts), visibility and present weather. The closest METAR reporting location at the time of the occurrence would have been Sachs Harbour (CYSY), Northwest Territories, on the southwestern shore of Banks Island, about 200 nm away. The 1700 METAR indicated that the wind was from the east at 11 knots with a visibility of 15 statute miles (sm) with broken clouds at 1700 feet above ground level (agl) and another broken cloud layer at 25 000 feet agl, temperature of +2 °C and a dew point of +1 °C. A number of non-METAR weather observations are available for the area around the M'Clure Strait, but none of these provides sky conditions, visibility, or present weather.
Graphic area forecasts (GFA) include clouds and weather charts as well as icing, turbulence and freezing level charts. The GFAs covering M'Clure Strait (GFACN37) that were issued on 09 September 2013 covered the area that included M'Clure Strait and Parry Channel as well as Banks, Prince Patrick, Melville and Victoria islands.
The GFA clouds and weather chart issued at 1141 and valid at 1200 (before the accident) and the chart valid at 1800 (17 minutes after the accident) depicted a large area of broken cloud with patchy ceilings between 500 and 1000 feet agl (Appendix A). There was also a forecast of local (25% or less of the area covered) visibilities reduced to 2 sm in snow and locally 1 sm in light freezing drizzle and mist in any onshore flows. The corresponding icing, turbulence, and freezing level charts indicated an area of moderate mixed icing in the cloud layers east of the surface ridge of high pressure and moderate clear icing in the local freezing drizzle (Appendix B).
AIRMETs are used to amend the GFA, and SIGMETs are used to warn pilots of hazardous meteorological conditions and amend the GFA if the phenomenon had not been forecast. No AIRMETs or SIGMETs were issued for the area around the time of the accident.
On 09 September 2013, the end of evening civil twilightFootnote 29 calculated at the accident location occurred at 2259. The azimuth of the sun was 238.3 degrees east of north and the sun's altitude was 13.3 degrees above the horizon. The sun was therefore behind and to the right of the helicopter while it was flying eastbound toward the vessel.
1.7.3 Actual marine weather
The CCGS Amundsen is equipped with an automated observing station, which reports temperature, dew point temperature, wind direction, wind speed, sea surface temperature, atmospheric pressure and pressure tendency.
On 09 September 2013, at 1700—41 minutes before the accident—the reported wind was from 130° at 6 knots. At 1800—17 minutes after the accident—the wind was from 140° at 3 knots, the outside air temperature was −1.4 °C and the sea surface temperature was −0.6 °C. After 1400, the dew point temperature was 1 to 2 °C cooler than the air temperature. Since the dew point temperature was cooler than the sea surface temperature throughout the day, it is unlikely that mist and/or freezing fog would have been occurring near the vessel. There is a high probability that the visibility would have been unrestricted during the afternoon and early evening hours. Photographs and videos taken during the flight showed that visibility was good, with no precipitation and with a defined line of horizon.
1.7.4 Ice conditions
The crew of CCGS Amundsen was receiving daily ice charts and satellite image analyses of the Parry Channel and M'Clure Strait. RADARSAT-2 imagery and ice concentration charts produced by the Canadian Ice Service were used to determine the ice conditions in the M'Clure Strait on the day of the occurrence.
The imagery taken closest to the time of the occurrence was taken at 1921:38 on 09 September 2013, 1 hour and 38 minutes after the occurrence, or 57 minutes after the ship's crew started to navigate toward the helicopter's last known position (LKP). In Figure 5, the ship and helicopter trajectories are indicated on the RADARSAT-2 imagery in order to see their track in relation to the ice conditions at the time of the occurrence.
Ice movement (flow) was measured from the image taken at 1403:36 on 09 September 2013, 3 hours and 40 minutes before the accident. The use of images taken before and after the occurrence allowed investigators to determine an approximate position of the edge of ice at the time of impact, which is represented by the red dashed lines in Figure 5.
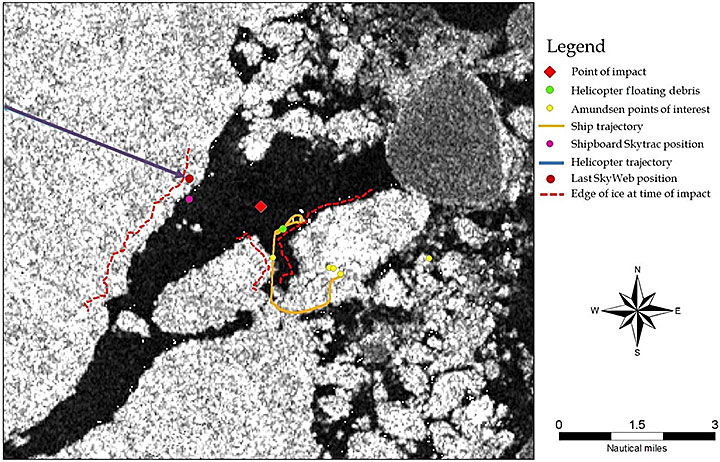
The imagery indicates that the open water area the helicopter was overflying was about 2.3 nm wide. Based on the actual wreckage position indicated on the RADARSAT-2 imagery, the helicopter crashed about 0.7 nm before reaching the next ice edge.
When the CCGS Amundsen was heading toward the helicopter's LKP, it was operating in very close pack ice, with a total ice concentration of 9+/10;Footnote 30 8/10 of thick first-year ice in big floe,Footnote 31 one-tenth of old iceFootnote 32 in big floe, and one-tenth of new iceFootnote 33 (Appendix C).
1.8 Aids to navigation
The CCGS Amundsen is equipped with a non-directional beacon (NDB), distance measuring equipment (DME) and the SkyTrac FFS as navigation aids to pilots conducting shipboard operations. These aids to navigation on board the vessel were all functional the day of the occurrence, with no defects reported.
The helicopter was equipped with an automatic direction finder (ADF), which, when in use, provides the pilots with a bearing to the ship's NDB; a DME, which provides a distance from the vessel; and the CDU interface of the FFS, which provides a bearing and distance to the vessel when in use. It was also equipped with a portable global positioning system (GPS), a Garmin GPSMAP 396 unit, as a navigation aid.Footnote 34 There were no defects recorded in the aircraft journey log concerning this equipment on board the helicopter.
1.9 Communications
1.9.1 Inflight communications procedures
During flight operations, the standard practice is to maintain a radio watch, even when the aircraft is equipped with an FFS.
According to the Shipboard Helicopter Information and Procedures Manual,Footnote 35 the standard schedule of communications procedures during normal flight operations includes the pilot
- establishing radio contact with the bridge after engine start-up;
- requesting take-off clearance from the flight deck officer (FDO) prior to each takeoff;
- advising the bridge when airborne and clear of the vessel;
- making a position report to the vessel every 15 minutes if the aircraft is not equipped with NavLink, or every 30 minutes if it is equipped with NavLink;
- providing the vessel with an ETA as soon as possible after takeoff;
- confirming the ETA at least 10 minutes prior to landing; and
- requesting landing clearance from the FDO at least 1 minute before landing on board.
In this occurrence, the last communication made by the pilot was the radio call to provide an ETA in 10 minutes. No distress call was heard or recorded.
1.9.2 Procedures for lost communications
According to the Shipboard Helicopter Information and Procedures Manual,if no contact has been made with the helicopter for any 15-minute period or by the next expected communication time
- a communications search will be carried out; and,
- if no contact is made within a further 15 minutes, SAR measures will be initiated.
In this occurrence, the last communication with the pilot took place at 1738, when the 10-minute ETA was reported. As per the normal communications procedures described above, in section 1.9.1 above, the next expected call would have been at around 1747 to request clearance just prior to landing. Therefore, according to the procedures, a communication search should have been initiated at 1748. However, the first attempt to communicate with the pilot was made at 1818, 30 minutes later.Footnote 36
According to procedures lost communications, the next step would have been to initiate SAR measures by 1803—15 minutes after the call that was expected at 1748 for landing clearance. At 1805, a member of the wheelhouse crew checked the helicopter position displayed on the SkyTrac FFS CDU, which was showing the helicopter being 3.2 nm from the vessel. At 1818, a communications search began, and at 1824, SAR measures were initiated and the vessel proceeded toward the last displayed position on the FFS CDU.
1.10 Aerodrome information
The vessel's flight deck serves as an aerodromeFootnote 37 for flight operations. There were no operational issues with the flight deck facilities on the vessel that could have had an adverse effect on the flight of CCG364.
The Shipboard Helicopter Information and Procedures Manual provides a single source of information and guidance for the ship/helicopter team. According to the Manual, the FDO duties are normally conducted by the chief officer, but may also be conducted by a qualified deck officer or boatswain. The FDO is responsible to the master or, in the master's absence, to the officer of the watch. In this occurrence, since the master was on board the helicopter, the master's duties were carried out by the chief officer, and the FDO duties were carried out by the second officer. The FDO was equipped with a portable very high frequency (VHF) radio to communicate with the helicopter pilot either directly or through the wheelhouse crew.
1.11 Recorders
1.11.1 Flight recorders
The helicopter was not equipped with a flight data recorder (FDR) or a cockpit voice recorder (CVR), nor was it required to be by regulation.
The benefits of recorded flight data in aircraft accident investigations are well known and documented. Flight recorders have been considered primary tools in large aircraft accident investigations for decades. Numerous TSB aviation investigation reports have referred to investigators being unable to determine all the reasons why an accident occurred due to the lack of on-board recording devices. Currently, CVRs and FDRs are considered the most comprehensive methods of capturing large amounts of flight data for accident investigation purposes. Investigation reports involving aircraft not equipped with flight recorders occasionally contain data downloaded from GPS, engine monitors, or other non-crash–protected, non-volatile memory sources in lieu of flight recorder and radar data. Investigations that are able to use data from flight recorders as well as from other recorder sources that contain non-volatile memory are more likely to identify safety deficiencies than investigations that do not.
Commercially operated aircraft weighing less than 5700 kilograms are usually not fitted at manufacture with the system infrastructure required to support an FDR, and conventional FDRs would require modifications in order to be installed in this category of aircraft. Several stand-alone, lightweight flight recording systems that can record combined cockpit image, cockpit audio, aircraft parametric data, and/or data-link messages, and that require minimal modification to the aircraft to install, are currently being manufactured. Several helicopter operators have already embraced this type of technology as a basis for the Flight Operational Quality Assurance (FOQA)Footnote 38 program recommended by the Federal Aviation Administration (FAA).
In the TSB Aviation Investigation Report A11W0048, the Board recommended that:
The Department of Transport work with industry to remove obstacles and develop recommended practices for the implementation of flight data monitoring and the installation of lightweight flight recording systems by commercial operators not currently required to carry these systems.
Transportation Safety Recommendation A13-01
Transport Canada supports this recommendation and is planning to proceed with the development of an Advisory Circular in 2015/16 to describe recommended practices regarding flight data monitoring (FDM) programs. In addition, TC will be consulting, through focus groups, to identify obstacles within Transport Canada's mandate and make recommendations for mitigation of those obstacles with respect to the installation of lightweight flight recording systems for commercial operators not required to carry these systems.
The Board is encouraged by the intent of Transport Canada to work towards meeting the issues identified in the recommendation; however, the work is ongoing. Therefore, the TSB has assessed TC's response to the recommendation as satisfactory intent. The TSB will continue to monitor the progress of the implementation of the planned actions progresses and will request further information from TC to reassess the deficiency.
1.11.2 Pictures and video clips
A Canon camera, model PowerShot G10, was recovered from the wreckage and brought to the TSB laboratory to see if any data could be extracted. Thirty-one images and 3 videos dated 09 September 2013 were extracted for photogrammetric analysis.
There was a significant difference between the video and still images and it is believed that the still images are more representative of the actual light conditions at the time. While the first video was recorded in colour, the second and third videos were recorded in black and white (Figure 6).

The review of the 3 video clips found that visual cues varied throughout the flight, but improved during the third leg. The video of the third leg showed that:
- the light was brighter than in the previous 2 videos;
- shadows were discernible and the sun was low in the sky, at approximately the helicopter's 5 o'clock position;
- dark overcast sky ahead created a distinct horizon against the white ice surface;
- the texture of the ice varied from smooth to jagged and broken; and
- no open water was in view.Footnote 39
No images or videos showed evidence of an imminent accident. However, the last image from the photos taken at 1732:57—approximately 10 minutes prior to the accident—was used for the photogrammetric analysis (Photo 5).

Using a 3-dimensional computer-aided design model of the BO 105, and based on the time the picture was taken as well as the sun's altitude and azimuth, the helicopter model was oriented to match the shadow seen in the picture to determine the helicopter's altitude and the direction it was facing at the moment the image was taken. It was determined that the helicopter was heading eastbound on a track of 96°, at an altitude of approximately 16.5 feet above the ice to the lowest point on the skid, with a bank of approximately 1 degree left and a pitch of approximately 1.5 degrees down. These parameters are consistent with aircraft attitude and altitude related to ice measurement operation.
In the 3 videos recovered, the upper left corner of the helicopter instrument panel appears in the image periodically, showing engine gauges. Frame captures from each segment showing the engine gauges were enhanced to show any instrument indications. The gauges for the oil temperature (OIL TEMP), oil pressure (OIL PRESS), turbines outlet temperature (TOT), and mast momentFootnote 40 were visible. The OIL TEMP for both engines and the main rotor transmission were all operating in the green arcs. The TOT, the OIL PRESS for the No. 1 engine and the main rotor transmission were also in the green arcs. Unfortunately, the TOT and the OIL PRESS gauges for the No. 2 engine were not visible on the frame captures. Based on the above indications, it is reasonable to believe that both engines were operating normally at the time the last picture and video were taken.
The images also show that the scientist had a laptop computer on his lap with the screen cover opened. The laptop computer is part of the scientist's equipment used for ice measurement operations.
1.11.3 Vessel recorder
The CCGS Amundsen was fitted with a voyage data recorder (VDR), although it was not required to be by regulation.Footnote 41 The VDR, a Rutter VDR-l 00G3, is capable of recording audio, videoFootnote 42 and National Marine Electronics Association (NMEA) data.
Shortly after the occurrence, the VDR data was saved by the crew on the vessel. The audio data was used to determine if any calls from the pilot might have been missed that could have explained the delay of the helicopter's arrival. Once on the vessel, the TSB investigators were provided with the saved data. Investigators used a variety of data from the VDR and the time of an audio noise that they did not attribute to interference to calculate a possible impact position using the helicopter track from the SkyWeb server logs. That position was used as a starting point for the search to recover the wreckage. During the search for the wreckage, a small debris field of light material (panels) and Plexiglas was located on the sea floor within 15 m of the calculated impact position. Therefore it was determined that 1742:59, the time at which the audio noise was recorded on the VDR, was the time of impact. This information allowed investigators to locate the wreckage with a level of precision that avoided days of searching.
The VDR files were provided to the TSB laboratory in Ottawa for further analysis. Viable audio, NMEA and video data from 1254 on 07 September 2013 to 1254 on 10 September 2013 had been recovered. Data from 1615 on 09 September 2013 to 2045 on 09 September 2013 was extracted from the package. By reviewing the video data, it was established that CCG364 was visible on radar leaving the vessel. A total of 6 radar images captured the helicopter in the vicinity of the vessel. Evidence of the helicopter being near the vessel at the time of impact with the water could not be found in the video data.
Audio recordings from 1600 on 09 September 2013 to 2100 on 09 September 2013 were also extracted for analysis. The audio files contained 5 separate channels. Two were VHF channels and the remaining 3 were area microphones located on the wheelhouse of the CCGS Amundsen. The audio quality was considered to be good.Footnote 43 No distress call from CCG364 was recorded.
1.12 Wreckage and impact information
1.12.1 Preliminary wreckage examination
On 25 September 2013, the aircraft wreckage was recovered and put on board the CCGS Amundsen and then transferred to the CCGS Henry Larsen, which was assisting in the search and recovery operation. During the search for the wreckage using a remotely operated vehicle (ROV), several other pieces of wreckage were located. However, due to the weather and deteriorating ice conditions, only the main wreckage was recovered. The recovered wreckage consisted of the cockpit, fuselage, landing skids, main transmission, rotor head (with one of the 4 rotor blades remaining), and both engines. The tail boom, severed just aft of the fuselage, was not recovered; the cockpit was compromised and missing several window and door sections.
Investigators from the TSB and Rolls-Royce conducted a wreckage and engine examination on board the CCGS Henry Larsen on 25 September 2013. Physical evidence observed on the aircraft power train components supports engine operation during the impact sequence. No evidence of pre-impact damage or abnormal operation was noted on either engine.
The wreckage was placed in a hangar on the CCGS Henry Larsen and transported to St. John's, Newfoundland and Labrador, under the TSB's supervision, where it arrived on 12 October 2013. It was then ground-transported to the TSB laboratory in Ottawa for further examination.
1.12.2 Impact damage signature and impact geometry
The wreckage examination was conducted at the TSB laboratory; representatives from Airbus Helicopters Deutschland GmbH, the German Federal Bureau of Aircraft Accident Investigation (Bundesstelle für Flugunfalluntersuchung [BFU]),Footnote 44 TC, and the CCG attended as observers.
The damage examination of the main structure and the ice probe indicated that the helicopter flew into water in a slight nose-down attitude and slightly banked to the right at a speed of approximately 54 knots. It is considered most probable that the damage observed on the top right-front of the helicopter occurred later during the crash sequence. Since the helicopter came to rest upside down, it is possible that this damage occurred when it struck the ocean floor. It is also possible that the helicopter's forward momentum on initial impact and the large resistance force from the water acting on its bottom surface created a moment of rotation that caused the helicopter to flip forward.Footnote 45
The examination of the tail boom section that remained attached to the helicopter revealed deformations and material transfer consistent with a rotor blade impact. The examination of ROV images taken on the sea floor suggests that the separated portion of the tail boom was also damaged due to rotor blade impact. As the separated portion of the tail was not recovered, it was not possible to conduct a detailed examination to confirm this hypothesis.
1.12.3 Flight controls examination
Examination of the flight control system and its components did not identify any abnormalities that would have prevented normal operation, and control continuity was observed throughout the systems. Although the tail boom had been severed during the impact sequence, ROV images of the tail rotor components were consistent with the tail rotor system being intact at the time of impact.
1.12.4 Instruments and annunciators examination
The instruments and annunciators were recovered with the wreckage for examination with respect to their indications at the time of impact. Microscopic examination of the instrument dial faces and internal mechanisms did not reveal any witness marks that may have indicated their position at the time of impact.
The bulb filaments from the annunciator panel light bulbs were microscopically examined to determine if they were on or off at the time of impact. Typically, a lamp filament will exhibit deformation such as elongation or stretching of the filament coil if it was hot when shocked; it may fracture into one or numerous pieces if sufficiently shocked when cold; or it may not show any change. There was no elongation or stretching of any of the filaments.
1.13 Medical and pathological information
Once on board the vessel, the 3 occupants were brought to the hangar on stretchers. None of the 3 occupants showed vital signs, but they did show signs of drowning. Resuscitation manoeuvres were carried out on the pilot but were stopped after a few minutes. No resuscitation manoeuvres were attempted on the master or the scientist. The 3 occupants were pronounced dead by the health officer.
The CCGS Amundsen sailed back to Resolute Bay, where the Royal Canadian Mounted Police (RCMP) took custody of the deceased on behalf of the medical examiner (ME). The deceased were then transported to the ME's facility in Edmonton, Alberta, where external examinations of the 2 passengers and the autopsy of the pilot were carried out on 16 September 2013. The ME concluded that the 3 occupants' death was the result of cold water immersion. Nothing indicates that the pilot's performance was degraded by physiological factors.
1.14 Fire
There was no pre-crash or post-crash fire.
1.15 Survival aspects
1.15.1 General
All of the occupants survived the impact but succumbed to drowning following cold water immersion. Research has shown that survival rates in Canadian civilian-registered helicopter accidents into water are consistent with previously reported worldwide data and remain at about 78%.Footnote 46 The research also shows that the lack of warning time prior to water impact and the final resting position of the helicopter—either sinking or inversion of the helicopter—are the major contributors to fatalities. Furthermore, drowning remains the primary reported cause of death in helicopter accidents into water.
When a helicopter inverts, the sudden inversion means that not only do the survivors have to escape from being completely submerged in cold water, but they also have to navigate their way out upside down, which is conducive to disorientation.Footnote 47
1.15.2 Life raft
Subsection 602.63(5) of the Canadian Aviation Regulations (CARs) states:
No person shall operate over water a multi-engined helicopter that is able to maintain flight with any engine failed at more than 50 nautical miles, or the distance that can be covered in 30 minutes of flight at the cruising speed filed in the flight plan or flight itinerary, whichever distance is the lesser, from a suitable emergency landing site unless life rafts are carried on board and are sufficient in total rated capacity to accommodate all of the persons on board.
In this occurrence, the flight was carried out over an area covered with an ice concentration of 9+, which included floes with widths of 500 to 2000 m. Eight-tenths of the area had a thickness greater than 120 cm. This ice thickness can safely support a load limit of 58 000 kilograms,Footnote 48 which is well above the helicopter's maximum certified take-off weight. Continuous ice capable of supporting the helicopter could have been used as a suitable emergency landing site. Therefore, the CARs requirement to carry a life raft on board did not apply to this flight. However, according to CCG Fleet Order 218.00, Helicopter Safety Equipment Requirements, and the Operations Manual, Canadian Coast Guard Helicopters,Footnote 49 the helicopter must be equipped with a TC-approved life raft whenever the flight plan of a CCG helicopter includes flight over water.
The TC-approved life raft installed on the occurrence helicopter was manufactured by the Winslow Life Raft Company in February 2008. The raft is a certified aviation appliance meeting the FAA Technical Standard Order (TSO) C-70a. The raft is mounted vertically on the rear of the centre pedestal, just in front of the rear seats. It is designed to hold 6 occupants and has an overload capacity of 9 passengers. The raft mounting structure had separated from the centre pedestal during the accident sequence. However, when the helicopter was recovered, the life raft was found still fastened to the rack and in the general area where it would normally be located within the cabin.
The service validation certificate indicated that the raft was valid for service and was due for its next servicing in April 2014. During the examination, the raft inflated to its design shape and pressure. However, after a period of 24 hours, the lower buoyancy tube of the life raft was observed to have completely deflated. A small cut, approximately 6 mm in length, in the exterior wall of the lower buoyancy tube was found and identified as the source of the leak. The lack of evidence of punctures or cuts to the exterior valise of the raft, or to the metalized poly wrap in which the raft was vacuum packed, indicates that the cut was likely present before the raft was packed. Given that the raft is capable of staying afloat with just 1 buoyancy tube inflated when the raft is at its overload capacity, it is unlikely that there would have been an issue with just 3 occupants.
1.15.3 Passenger transportation suit regulatory requirements
Currently, the regulatory requirements and standards for aircraft passenger transportation suit system (PTSS) are contained in CAR 602.63(7)(a) and CARs Standard 551.407.
Subsection 602.63(7) of the CARs states in part:
Where a helicopter is required to carry life raft […], no person shall operate over water having a temperature of less than 10 °C unless
(a) a helicopter passenger transportation suit system is provided for the use of each person on board […]
Following TSB investigation A09A0016, TC indicated that these provisions do not apply to flight crew suits. That seems to contradict subsection 602.63(7)(a), which states that “each person on board” has to be provided with a helicopter PTSS. It would be reasonable to believe that each person includes the flight crew. However, because some of the design features of the PTSS are not compatible with wearing a helmet or headset, interfere with flight control range of movement or limit flexibility, and contribute to thermal fatigue (overheating), TC reviewed the requirement for a unique flight crew transportation suit system.Footnote 50 TC subsequently proposed an amendment to paragraphs 602.63(7)(a) and (b)Footnote 51 of the CARs, which included the requirement for each crew member to wear a helicopter crew member transportation suit. TC indicated that the development of the crew transportation suit standard would take some time and, until then, the new regulation would permit operators to choose to use any crew-specific suits that provided adequate protection.
Although there currently is no TC specification for this type of transportation suit, in 2006, the European Aviation Safety Agency (EASA) published the following suit design standards, which apply to both crew and passengers:
- European Technical Standard Order (ETSO-2C502), Helicopter Crew and Passenger Integrated Immersion Suits;
- European Technical Standard Order (ETSO-2C503), Helicopter Crew and Passenger Immersion Suits for Operations to or from Helidecks Located in a Hostile Sea Area.
In this occurrence, since the CARs did not require a life raft to be carried on board, as stated in section 1.15.2 of this report, passengers were not required to be provided with or wear a PTSS based on the CARs.
Section 551.407 of the CARs Part V StandardsFootnote 52 defines aircraft PTSS as
a personal immersion suit system that reduces thermal shock upon entry into cold water, delays onset of hypothermia during immersion in cold water and provides some flotation to minimize risk of drowning, while not impairing the wearer's ability to evacuate from a ditched aircraft.
According to the CARs, the current design standardsFootnote 53 and other standardsFootnote 54 apply to PTSS and are acceptable criteria as a basis of certification. Despite the fact the CARs refer to the current design standards as CAN/CGSB-65.17-99, published in 1999, a new standard was developed in 2012Footnote 55 according to the Standards Council of Canada website. However, there are currently no known products qualified to this most recent standard. According to CAN/CGSB-65.17-99 standard, the PTSS must provide thermal protection of at least 0.75 clo.Footnote 56
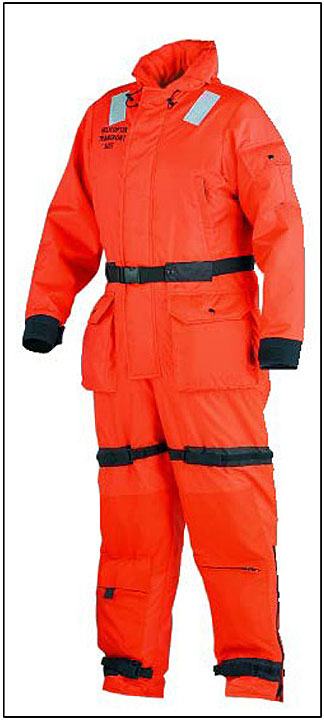
Both the master and the scientist were wearing a Mustang Survival model MS2175 TC helicopter transport suit (Figure 7), which is approved by ASD/CCG for use as an immersion suit. However, this model is not certified to any standard and has an insulation value of 0.4 clo in still water. This suit is based on Mustang Survival's original floater suit concept with modifications to assist the wearer in a safe egress from a ditched helicopter. Compared to the floater suit, the helicopter transport suit has less buoyancy, which allows for safe egress, and has additional anti-exposure protection that affords the wearer increased in-water survival time. Mustang Survival advises that buoyancy should be enhanced by adding a manually inflatable life preserver. According to the manufacturer, this product is intended to provide flotation and hypothermia protection in the event of cold water immersion.
The MS2175 TC suit is equipped with a neoprene hood and 3-fingered lobster-claw-style gloves, which are stored in the 2 integral calf pockets. The suit's wrist and ankle cuffs are equipped with a hook-and-loop type attachment to allow for individual adjustment. The suit design allows for water ingress at the neck and at the wrist and ankle cuff locations.
The suits are supplied in sizes ranging from extra small to triple extra-large. Both the master and the scientist were wearing a large (42-46 inch) suit. Based on the suit's sizing chart and the fact that both individuals were wearing winter clothing, the large size would have been appropriate. No donning/doffing instructions are provided with the suit.
During recovery, it was noted that both passengers' suits were full of water and that neither passenger was wearing the hood or gloves. Examination of the suits noted that the hoods and gloves were in the storage pockets and that the pockets were zipped closed. According to TC publication TP13822, Survival in Cold Waters: Staying Alive, the 3-fingered lobster-claw-style glove “(…) in practice works very well, but any tasks that require fine tactility will not be easy.”
According to the CAN/CGSB-65.17-99 standard, one of the performance requirements for helicopter PTSS is “righting”, which is defined as:
The suit system shall turn the wearer from a face-down position to a face-up position within 5 [seconds] or allow the wearer without assistance to turn himself or herself from a face-down position to a face-up position within 5 [seconds]. If a suit system has auxiliary buoyancy, the suit system shall be designed to meet these requirements when the auxiliary means of buoyancy is used as well as when it is not used.Footnote 57
Neither of the 2 passengers wearing the MS2175 TC suit was found floating completely on their back.
1.15.4 Aircraft Services Directorate / Canadian Coast Guard immersion suit policy
According to the Operations Manual, Canadian Coast Guard Helicopters,Footnote 58 it is mandatory for CCG helicopter crews and passengers on board a multi-engine helicopter flying over water at distances greater than 15 nautical miles from ship, shore, or continuous ice capable of supporting the helicopter, to wear immersion suits. CCG Fleet Order 218, Helicopter Safety Equipment Requirements, identifies the same requirements for its personnel; however, the document refers to the suit as a helicopter passenger transportation suit system (HPTSS). ASD and CCG documents use the terms immersion suit, passenger transportation suit system, and dry suit interchangeably even though each of these types of suits has its own unique characteristics.
In this occurrence, even when the helicopter was flying over open water, it was always within 15 nm from continuous ice capable of supporting the helicopter in case of an emergency landing. Based on this, there was no requirement to wear immersion suits or HPTSSs, but the Speciality Operations Catalogue (SOC) requires flight crew and technical crew to wear appropriate survival equipment for the area of operation. However, the SOC does not define area of operation in order to determine what is considered appropriate as survival equipment.
The Operations Manual, Canadian Coast Guard Helicopters,Footnote 59 requires that when life rafts are required to be carried and the water temperature is less than 10 °C hypothermia protection be provided for each person on board. While ASD and the CCG strongly encourage crew and passengers to wear approved immersion suits/PTSS at all times when a flight is taking place over water, it is not mandatory to wear them if the combined water and air temperature is above 25 °C. This is to protect against the risk of heat exhaustion and dehydration that can occur with the constant wearing of immersion suits.
1.15.5 Aircraft Services Directorate flight crew immersion suits
Following the Marystown, Newfoundland and Labrador, accident (A05A0155), the joint ASD/CCG Passenger Safety Working Group recommended that an improved crew immersion suit be provided. CCG helicopter operations are conducted under significantly different conditions from off-shore oil exploration and production industry operations. ASD faced the challenge of finding a constant-wear suit that provided not only a high level of protection but also a good degree of usability in normal operations throughout all seasons of the year. A risk assessment of over-water operations was conducted and after a review of available industry equipment, and a 12-month trial with both pilots and aircraft maintenance engineers testing different suits, the Viking immersion suit model PS4089 with quilted liner number PS4830 was selected and purchased.

The Viking PS4089 is a waterproof GORE-TEX® suit with a waterproof zip fastener, neoprene collar and wrist seals, and attached waterproof socks (Figure 8). Neoprene 3-finger lobster-claw-style gloves and a hood are stored in the lower leg pockets. A set of zippers had been incorporated into the suit to allow for the Switlik life vest to be attached directly to the suit. The suit does not completely seal water out due to the split neck seal design and, therefore, some leakage does occur.Footnote 60 There is no inherent buoyancy provided by the PS4089 suit,Footnote 61 and it provides limited thermal protection when dry. Buoyancy is provided by a separate flotation vest, and thermal protection is provided by the thermal lining. When dry, the suit has an insulation value of 0.7 clo in still water. However, when filled with water, the suit insulation decreases to as low as 0.15 to 0.2 clo. The requirement of a minimum clo value of 0.75 for PTSS does not apply to flight crew and there is currently no definition or regulatory standard for a flight crew immersion suit. The ETSO set a minimum of 0.5 clo value for a flight crew suit.
On 10 April 2012, the pilot was provided with personally fitted PS4089 immersion suit and a PS4830 thermal liner.Footnote 62 The pilot received training on the use and maintenance of the suit. The importance of zipping the suit completely closed was reinforced during the donning/doffing portion of the suit training sessions. On the day of the occurrence, the pilot was wearing the suit with the supplied insulated thermal lining.
During recovery, it was noted that pilot's suit was full of water and that the zipper was done up to about the mid-sternum position. Examination of the suit noted that the hood and gloves were in the storage pockets and that the pockets were closed. Additionally, a small tear was noted on the back of the right upper sleeve. To completely close the zipper requires the use of both hands: one to pull the zipper, the other to ensure the zipper does not get caught on the suit material. As the zipper is being pulled past the neck, the wearer must bend their head back and to the right, which allows the zipper to be pulled straight.
During flight, it was a common practice for ASD pilots to leave their immersion suits partially unzipped, to about the mid-sternum position. In May 2011, TC ASD issued an internal documentFootnote 63 that described the new immersion suit and the philosophy behind its use. The document stated in part:
Viking suit design incorporates a “split neck” seal, which allows the suit to be partially unzipped during some flight conditions. A set of zippers has been incorporated that allow the Switlik life vest to be attached directly to the suit while at the same time allowing the suit zipper to be partially unzipped. In order to achieve the maximum protection, it is of critical importance that the suit be fully zipped up and closed to the top of the neck seal prior to entering the water. It should be worn like this any time there is a risk of entering the water following an emergency or an intentional water landing where it is possible that the aircraft will not remain upright.
The memo included a note stating that:
Crew and passengers are encouraged to wear approved immersion suits even when conditions do not require their mandatory use. Additionally, any time the PIC [pilot in command] believes conditions justify the wearing of immersion suits, passengers and other crew members shall wear an immersion suit regardless of the criteria listed in the memo.
1.15.6 Personal flotation device
According to the Operations Manual, Canadian Coast Guard Helicopters and the CCG Fleet Order 218.00, where the flight plan includes flight over water, all passengers aboard CCG helicopters must wear a CCG-approved personal flotation device (PFD) for the duration of the flight. The Switlik HV-35C helicopter crew vest is approved for use and was the type of PFD worn by all the occupants.
The Switlik HV-35C helicopter crew vest has a mesh back and is equipped with 2 buoyancy chambers, each with its own manual CO2 inflator,Footnote 64 and an oral inflation tube. The vest incorporates 2 pockets, each with a cover flap, which is held in place by a hook-and-loop type fastener and a locking buckle (Photo 6).

The HV-35C is FAA-certified in accordance with TSO C13d. According to TC, life preservers that are certified to TSO C13d are approved for use in Canada.
TSO C13d states the preserver must support the wearer in the flotation attitude when no more than one-half of the flotation chambers are inflated and the other flotation chambers are fully deflated. The life preserver must right the wearer who is in the water in a face-down attitude within 5 seconds of activation. The inflated life preserver must keep the mouth and nose of a completely relaxed wearer held clear of the water line with the trunk of the body inclined backward from the vertical position. The mechanical means to inflate the preserver is to pull the cord assemblies attached to each inflation device. The force to do this must not exceed 15 pounds.
The HV-35C inflation and use instructions state:
- Do not inflate life vest while inside the aircraft.
- After exiting the aircraft pull sharply on the inflation lanyards.
- If life vest does not inflate or is not firm blow into the oral inflation tubes.
- Pull tab on water activated battery to turn on light.Footnote 65
The donning procedure pictogram on the vest indicates that both lanyards are to be pulled at the same time.
In March 2013, ASD's Chief, Maintenance Quality Assurance, was advised by one of ASD's base personnel that an improperly folded PFD had been found, and that the vest overhaul manualFootnote 66 did not contain a reference drawing that illustrated the instructions for folding the PFD. Before the end of the month, a corrected version of the vest overhaul manual was provided to the base and the individual was instructed to review the latest procedures.
On 23 September 2013, another instance of an incorrectly folded PFD was discovered by the same individual at the same base. ASD immediately performed an internal quality assurance review, and on 25 September 2013, issued Campaign Notice 010-25-60-027, Switlik life preserver folding procedure.
In March 2014, ASD found 7 PFDs that were incorrectly folded. To clarify the folding procedures, ASD issued a second campaign notice (010-25-60-027 Rev A), on 15 May 2014, and produced and distributed an instructional video for personnel responsible for inspecting and folding life vests. The vest manufacturer's instructions require the flotation cells to be accordion folded as opposed to being rolled.
In order to ascertain the potential hazard of an improperly folded PFD, ASD performed a deployment test.Footnote 67 An ASD employee donned the vest then pulled only the right side lanyard. The right side cartridge activated, causing the buoyancy chamber bladder to inflate. It was noted that the right side seal released immediately, allowing the right side of the bladder to expand. However, the left side seal did not immediately release, which prevented the left side of the bladder from inflating. With movement of the arms, the left side seal released, which allowed the left side of the bladder to inflate. The left side lanyard was then pulled and the second buoyancy chamber bladder fully inflated.
The master was recovered wearing an un-inflated PFD. A TSB investigator tested the PFD by pulling on both lanyards. Both cylinders activated and when the PFD began to inflate, it was noted that the collar hook-and-loop type fastener did not immediately release. Not knowing about the packing issue at the time of this test, it was not possible to determine if their flotation cells had been rolled or accordion folded.
The scientist was recovered wearing a partially inflated PFD; only the left side was inflated. When the TSB examined the PFD, it was noted that both cylinders had been activated. However, it could not be determined if both had been activated by the scientist or if they had been accidently activated while or after the scientist was being pulled out of the water.
Although the pilot had donned the PFD prior to departing on the flight, the fully inflated PFD was floating near the pilot and was recovered separately. The investigation examined the PFD and found no discrepancies, and no damage was noted on either portion of the zipper or the buckle. Since the PFD had been inflated, it was not possible to determine if the flotation cells had been rolled or accordion folded. All 3 crew PFDs were manually inflated and held pressure.
Once informed about the issue of PFDs not being folded correctly, the TSB examined the 4 spare PFDs recovered with the helicopter. All 4 were found with their flotation cells rolled up instead of accordion folded. The last maintenance inspections for the PFDs on board C-GCFU were conducted in July 2013. The 3 occupants' PFDs had been inspected in the same manner as the 4 spare ones.
1.15.7 Flight helmets
The pilot was wearing a helmet at the time of the occurrence. According to CCG Fleet Order 218.00, any passenger occupying the front seat of a CCG helicopter must wear the flight helmet provided on the aircraft. The flight helmet worn by the scientist was found separately within the helicopter wreckage. Both ends of the chinstrap were fastened together,Footnote 68 but the right side strap had been torn away from its attachment at the helmet. This suggests that the scientist had been wearing the helmet at the time of impact. The master had not been wearing a helmet, nor was it required. In addition to offering protection, the helmet may provide head insulation.
1.15.8 Personal locator beacon
Personal locator beacons (PLB) are not required by regulation. However, according to CCG Fleet Order 218, Helicopter Safety Requirements,
(…) all PFDs worn by CCG personnel onboard CCG aircraft are to be equipped with a functioning PLB. The carrying of a PLB is not a mandatory requirement when flying onboard an aircraft which is being followed with a satellite flight following system.
The 3 occupants' PFDs were equipped with a waterproofFootnote 69 PLB (Aerofix 406 GPS/IO, model PLB-200) manufactured by ACR Electronics Inc. (Figure 9).

When initially provided to TSB investigators, the master's and scientist's PLBs were found stored in their PFD's right side pocket, whereas the pilot's PLB was found outside of the pocket, attached to the PFD via its lanyard. It could not be determined if the pilot had pulled the PLB out of the pocket or if it had been accidentally pulled out during or after recovery.
The PLB transmits distress signals to COSPAS-SARSAT network satellites on both 406 MHz and 121.5 MHz, and is fitted with an internal GPS receiver that will determine the latitude and longitude of the unit's position. When GPS data is included in the distress message, SAR reaction time is greatly improved because location identification of the beacon becomes accurate to within 100 m.Footnote 70
The PLB is designed to be manually deployed and activated. To activate the PLB, the antenna must be unfastenedFootnote 71 from the case and moved into the upright position. The operator must then lift the cover to reveal the keypad and press the self-test and GPS I/O buttons simultaneously for at least ½ second and less than 5 seconds. To ensure proper operation, the antenna needs to be unobstructed, with a clear view of the sky; therefore, it cannot be covered by anything such as clothing, survival equipment, or water. According to the manufacturer, it is important to keep the antenna dry and away from the water for best results. Water detracts from the PLB's performance and reduces its effectiveness.
The examinations and tests of the 3 occupants' PLBs determined that they were within the manufacturer's specifications and that there were no anomalies that could have prevented them from performing as designed at the time of the occurrence. The tests did not verify the PLB's GPS function upon activation or its ability to incorporate GPS coordinates in the distress message, as the TSB laboratory's shielded test facility prevented signal transmission into or out of the room. However, even without the GPS coordinates incorporated in the distress message, the COSPAS-SARSAT network can still locate the distress beacon to within an area of 1 to 2 km.Footnote 72
1.15.9 Helicopter underwater egress training
The CARs do not require that ASD have its flight crews complete helicopter underwater egress training (HUET). However, ASD had been recommending that its flight crews take HUET since the mid-1990s. ASD implemented mandatory HUET in 2011. Since 2012, this training has been carried out with the flight crews wearing their individually fitted suits. ASD has indicated that almost all of its pilots have taken the new training. Recurrent training is required and is provided every 3 years. At the time of the occurrence, it had been almost 2 years since the pilot had taken HUET.
The scientist had not taken HUET, nor was it required by regulation. However, CCG Fleet Order 536.00, which was approved in 2007, strongly recommended that all employees required to regularly fly on board helicopters take HUET. According to the Fleet Order, all employees who are required to be on board helicopters to carry out their duties and are interested in taking the course can receive HUET. However, priority is given to frequent travelers, which are defined in the Fleet Order as employees of CCG required to fly in helicopters, as part of their job duties or as a passenger, on a monthly or more frequent basis—more than 12 times in a calendar year. Nothing indicates that the master had taken HUET.
1.15.10 Frequency and fidelity of basic survival training
The Industrial Foundation for Accident Prevention (IFAP) in Australia conducts the majority of HUET for the offshore oil industry in Australia. IFAP has determined that skills acquired during training are subject to significant decay within 6 to 12 months of initial training.Footnote 73 The IFAP also recommended that students should be over-trained to combat the serious hazards of a ditching. They concluded that:
Studies of procedural skills and the performance of safety functions generally show that the most significant degree of [dunker] skill decay occurs within 6-12 months of initial training. Evidence indicates that the current statutory two year period for helicopter underwater escape training without proper interim refresher training is too long.
Research sponsored by the oil and gas industry has similarly highlighted the importance of refresher training in maintaining the procedural skills associated with escaping from a submerged helicopter. In a 1997 study,Footnote 74 over one third of participants who had previously received HUET training were unable to effectively complete an underwater egress and, even after 6 months post-HUET training, frequently performed tasks in the wrong order. In addition to emphasizing the importance of recurrent training, the report called for additional study to determine an optimal interval between training sessions. ASD does not provide any additional training to mitigate procedural skill decay occurring in the 3 years between recurrent HUET sessions, nor is it required by regulation.
1.15.11 Water immersion
1.15.11.1 Canadian Coast Guard passenger briefing video
A passenger briefing video is available to all individuals who travel on CCG's vessels. The video covers general safety around the helicopter and the helicopter's safety features, and includes instructions on life vest donning and operation, PLB operation, and life raft operation and entry from both the helicopter and the water. CCG's practice is to have those who are new to helicopter operations view the video.
1.15.11.2 Cold water immersion phases
There are 4 phases of cold water immersion.Footnote 75 The first phase, cold shock, is the primary cause of crew and passenger drowning in helicopters that ditch in cold water.Footnote 76 Footnote 77 Even with the protection of an immersion suit, the sudden exposure to the cold water causes a gasp reflex, hyperventilation, and involuntary water intake. The gasp reflex and hyperventilation can last from 10 to 120 seconds. In this occurrence, the occupants were immediately exposed to cold shock as the helicopter inverted into the −0.6 °C water before it sank in. Like the gasp reflex, hyperventilation is a natural reaction to cold. Although this physiological response will diminish, panic can cause a physiological continuance of hyperventilation, which can lead to fainting. The intensity and length of the cold shock response is dependent on the amount of skin that is cooled, the rate of cooling, and the ultimate lowest temperature. In conjunction with this, the heart rate increases to dangerously high levels and may cause cardiac arrest or arrhythmia.Footnote 78 Footnote 79 As the temperature of the water decreases, so does the average breath-holding time. In near freezing water, breath-holding time in a well prepared test subject drops dramatically to about 10 to 15 seconds.Footnote 80
The second phase of cold water immersion is cold incapacitation. During this phase, the muscles and nerve fibres cool, which decreases their ability to function and leads to limitations fine motor movements and then gross motor movements.Footnote 81 Footnote 82 In 0 °C water, the decline in physical performance could start within 1 to 2 minutes, and complete incapacitation could occur within 10 to 20 minutes. Without gloves, muscle and nerve cooling would quickly decrease hand dexterity and strength.
The third phase is hypothermia. Normal body core temperature is 37 °C. The clinical threshold for mild hypothermia is 35 °C, with the following classifications: Mild Hypothermia, 35–32 °C; Moderate Hypothermia, 32–28 °C; and Severe Hypothermia, less than 28 °C. An adult human body in normal winter clothing will normally take at least 30 minutes before reaching mild hypothermia in 0 °C water and more than 2 hours before becoming severely hypothermic with a risk of cold-induced ventricular fibrillation.Footnote 83 The addition of thermal protective clothing will delay the onset and severity of hypothermia. Factors that affect body heat loss, clothing insulation, and rate of core cooling include water current, sea state, amount of body exposed to the water, body mass, and percent of fat.
Circum-rescue collapse is the fourth phase and can occur just before, during, or after rescue/extraction.Footnote 84 Symptoms range from physical collapse to fainting, to cardiac arrest and death. Rescue can cause mental relaxation and decreased stress hormone production (e.g., epinephrine), which can lead to a large drop in blood pressure, and as the cold, irritableFootnote 85 heart works harder to maintain blood pressure, it can stop.
For practical purposes, a significant risk of immersion hypothermia is usually considered to arise in water colder than 25 °C. Using 25 °C as the definition of cold water, the risk of immersion hypothermia in North America is nearly universal during most of the year.Footnote 86
1.15.11.3 Cold water immersion model
The cold water immersion modelFootnote 87 was used to predict the rate of core cooling for each victim, using factors such as water and air temperature, type of clothing and suit worn, age, height, and weight (Table 2).
| Core body temperature | Pilot | Master | Scientist |
|---|---|---|---|
| 34 °C | 78-90 | 90-132 | 96-138 |
| 28 °C | 162-186 | 180-252 | 192-270 |
Based on the cold water immersion model, the core temperatures of the 3 victims were predicted to be no lower than 34 °C when recovered (mild hypothermia). At a core temperature of 34 °C, the victim would likely still be conscious, but would be incapacitated for all but gross motor actions involving general movements of the arms and legs.
The times for the pilot are calculated with the suit zipped to about the mid-sternum position, which is the position the zipper was in when the pilot was found. The pilot's suit was full of water, which would have negated the insulation value of the thermal liner and would have resulted in faster cooling. It is noteworthy that, when an intact Viking PS4089 suit is completely zipped closed and worn with the insulation liner, the length of time for the core body temperature to reach 34 °C would be up to 7 hours.
Neither the scientist nor the master was wearing the supplied hood or other means of head insulation. It has been demonstrated that immersion of the back of the head in cold water can increase the core cooling rate to some extent.Footnote 88
The pilot was found floating face up, and not wearing a PFD. The scientist was found on his side, with the PFD only partially inflated. The master was found face down; the PFD was not inflated. Without the additional buoyancy provided by a properly inflated PFD, all of the occupants would have required more effort and movement to maintain their airway above the water, which would have resulted in increased heat loss.
1.15.12 Cold water drowning
If drowning occurs in water with a temperature above 20 °C, brain death normally occurs in 4 minutes or less. If drowning occurs in cold water, especially below 10 °C, the brain can survive longer periods without oxygen before irreversible damage occurs.Footnote 89 Survival after 10 to 30 minutes of immersion is often reported. The greatest amount of time anyone has survived being submerged in ice water is 66 minutes (although this is an extreme example).Footnote 90 Since core temperatures were not measured when the victims were recovered from the water, it is not known to what extent any brain cooling occurred in this occurrence. Because neither their bodies nor their airways were completely or continuously submerged beneath the water surface, brain cooling would have been less extensive than what is normally seen in cold-water drowning. As a result, there is little probability that brain cooling had an impact on their survival or the success of post-rescue resuscitation efforts.
1.16 Tests and research
1.16.1 Personal flotation device testing in a swimming pool
Following the occurrence, the TSB conducted PFD testing in a swimming pool; ASD provided the type of immersion suit worn by CCG helicopter pilots and 4 PFDs. Two of the PFDs were prepared according to the manufacturer's instructions, with the air bladders accordion folded inside the life vest covering. The other 2 PFDs were prepared with the air bladders rolled inside the life vest covering, which is the manner in which the spare PFDs on board the occurrence helicopter were found. It is likely that the 3 occupants' PFDs were also rolled rather than folded.
Four inflation tests were conducted. For the purposes of the test, the subject was in the water at the deep end of a swimming pool wearing the immersion suit and a PFD. The vest was attached and deployed as described below. The immersion suit was fully zipped for the first 3 tests and unzipped to mid-sternum for the fourth test.
The tables below represent the result of these tests.
| Vest condition | Properly packed—accordion folded. |
|---|---|
| Method of attachment | Zipped to immersion suit and buckled. |
| Method of inflation | Toggles pulled independently—right side first. |
| Observations | On entry into the water, a significant quantity of air was trapped in the suit, which made it difficult for the subject to roll from front to back. The suit provided sufficient flotation to keep the subject on the surface. On initial deployment of the right side toggle, the vest did not fully inflate. The yellow air bladder was observable only at the back of the jacket. On deployment of the left side toggle, the vest opened fully and kept the subject floating face up. This suggests that with the vest properly packed, one cartridge should be sufficient to fully inflate the applicable collar of the vest. Only the front inflation collar (which is activated with the left side toggle) remained inflated throughout the test. Inspection revealed that the rear inflation collar was leaking through the manual inflation valve. Attempts to manually inflate the vest were unsuccessful. |
| Vest condition | Properly packed—accordion folded. |
|---|---|
| Method of attachment | Buckled only; zipper undone. |
| Method of inflation | Toggles pulled simultaneously. |
| Observations | The vest inflated correctly and immediately. When inflated, the vest remained on the subject and the subject was maintained floating face up. The inflated vest was uncomfortable, placing pressure on the subject's face, neck and ears. |
| Vest condition | Improperly packed—rolled. |
|---|---|
| Method of attachment | Zipped to immersion suit. |
| Method of inflation | Toggles pulled independently—right side first. |
| Observations | Only the right side of the vest inflated when the right side toggle was pulled. With the vest packed in this manner, one cartridge was not sufficient to release the hook-and-loop fastener on the covering and allow the collar to fully inflate. The vest inflated completely when the second toggle was pulled. |
| Vest condition | Improperly packed—rolled. |
|---|---|
| Method of attachment | Zipped to immersion suit and buckled. |
| Method of inflation | Toggles pulled simultaneously. |
| Observations | With both toggles pulled, the vest inflated immediately and completely. |
During the test the following was observed:
- Zipping the suit with one hand only from mid-sternum all the way up was impossible. Even with 2 hands, help from a third person was required to zip it all the way up.
- The subject was able to remove the fully inflated life vest while in the water. However, in cold water, this would have been much more difficult since the loss of manual dexterity would have made finding and opening the zippers and buckle difficult.
- The subject was able to reach all of the pockets on the immersion suit and life vest while floating in the water with the vest fully inflated.
- The subject was able to locate (albeit with some difficulty) and use both manual inflation tubes.
- Diving below the surface with the immersion suit on and the life vest off was extremely difficult due to the buoyancy provided by the suit (even with the suit partially unzipped and with water in the suit).
1.16.2 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP197/2013 – Switch Examination
- LP198/2013 – Non-Volatile Memory Recovery
- LP205/2013 – Float System Examination
- LP214/2013 – ULB Examination
- LP222/2013 – Instrument Examination
- LP232/2013 – Helicopter Structure and Seat Examination
- LP235/2013 – Flight Control Continuity Examination
- LP243/2013 – Photogrammetric Analysis of Videos
- LP047/2014 – Life Raft Testing
- LP052/2014 – PLB Activation Test
1.17 Organizational and management information
1.17.1 Canadian Coast Guard
1.17.1.1 General
The Canadian Coast GuardFootnote 91 (CCG) provides key maritime services, including SAR, to Canadians. It ensures safe and accessible waterways and plays a key role in ensuring the sustainable use and development of Canada's oceans and waterways. In this occurrence, the CCGS Amundsen was chartered by ArcticNet in support of ArcticNet's 82-day scientific mission.
1.17.1.2 Particulars of the vessel
| Name of vessel | Amundsen, previously Sir John Franklin |
|---|---|
| International Maritime Organization (IMO) number | 7510846 |
| Port of registry | Ottawa, Ontario |
| Flag | Canada |
| Type | Icebreaker, science and exploration |
| Gross tonnage | 5910 |
| Length | 90.22 m |
| Draft | 9.6 m |
| Built | 1978, Vancouver, British Columbia |
| Propulsion | 2 fixed-pitch propellers driven by 6 diesel electric AC/DC engines |
| Cargo | Scientific equipment and personnel |
| Crew | 40 crew, 33 ArcticNet scientists |
| Registered owner(s) | Canadian Coast Guard |
| Manager(s) | Commissioner, Canadian Coast Guard |
1.17.1.3 Description of the vessel
The Amundsen is of typical steel hull icebreaker construction (Photo 7). The vessel was purpose built as Sir John Franklin icebreaker registered in 1979 and decommissioned in 1995. In 2003, the vessel was modernized and refitted under the commission of ArcticNet.

The vessel was recommissioned to the CCG with the agreement that it would be crewed by Coast Guard personnel and be dedicated to Arctic scientific exploration from May to December. Part of the vessel refit included the fitting of a 2.3 m x 2.3 m moon pool. The moon pool allows personnel on board to conduct oceanographic surveys without cutting through the ice. It also allows for the deployment of remote operated vehicles, such as that which was used for the search and recovery of the helicopter.
The Amundsen navigation bridge is equipped with the required navigational equipment, including 2 radars, 2 electronic chart systems (ECS), 2 global positioning systems (GPS) and an IceVue system. The vessel can be navigated from any of the 3 command stations—port, centre, and starboard.
1.17.1.4 Canadian Coast Guard's rescue specialists
CCG rescue specialists (RSs) are regular vessel crew members who, in addition to performing the duties required by the work description of their position on board the vessel, volunteer to undergo the RS training to provide this service. They are responsible for effecting rescue and extrication of casualties in the maritime environment, providing pre-hospital emergency care for survivors, and first aid to people carried on board CCG vessels.
When there is a delay in accessing definitive medical care, or where advanced medical interventions are required, RSs provide care based on direction received from a medical authority on shore. In this occurrence, there was an health officer (HO) on board who was the lead for any medical emergency. Therefore, the main task of the RSs was initially to recover the occupants and bring them onboard the vessel as soon as possible. Due to space constraints in the FRC, it was impossible for the RSs to attempt resuscitation manoeuvres on the occupants until they were brought on board the vessel and taken care of by the HO.
According to the CCG Fleet Order 535.00, a minimum of 2 designated RSs should be on board a medium icebreaker such as the CCGS Amundsen. In this occurrence, there were 4 RSs on board.
1.17.1.5 Rescue specialist training
The initial RS training program consists of 120 hours of classroom training and approximately 24 hours of homework and study during the course. The training program consists of 10 modules, including treatment for victims of hypothermia and cold near-drowning. The student must obtain a mark of 80% or more to pass. Students achieve a passing mark if all performance objectives are achieved during simulations, exercises and practical tests. Once the course is completed and passed, the RS certification is valid for 3 years. All 4 RSs on board the vessel had valid certificatesFootnote 92 on the day of the occurrence.
1.17.1.6 Health officers
The HOs on board CCG's vessels are hired under contract through a pool of qualified candidates. The HO on the CCG Amundsen on the day of the occurrence graduated as a nurse in 1973 and had been working on contract for the CCG since 2003.
An HO is defined in the CCG Health Officer ManualFootnote 93 as a Registered NurseFootnote 94 (RN) with advanced nursing practiceFootnote 95 skills working aboard Coast Guard vessels. According to the Framework for the Practice of Registered Nurses in Canada,Footnote 96 RNs develop expertise in their chosen areas of practice through self-learning, speciality certification,Footnote 97 mentorship programs, advanced academic education, and utilization of best practice guidelines.Footnote 98 At the time of the occurrence, the HO had a valid Cardiopulmonary Resuscitation and Automated External Defibrillator certificate, which must be renewed every 2 years.
Aboard the vessel, the HO works directly under the master's direction. However, the HO is the lead for any medical emergency.
Among the HO's responsibilities described in the CCG Health Officer Manual is the responsibility for administering adjuvant therapy, including oxygen, intravenous therapy, injections, splints, slings, tensor bandages, and cardiopulmonary resuscitation (CPR), based on individual patient requirements.
In this occurrence, the HO was advised to get ready to receive patients with possible hypothermia symptoms. Warm blankets, therapeutic oxygen, and intravenous solutions were prepared. Since the medical facility onboard could not accommodate 3 patients at the same time, the 3 recovered aircraft occupants were brought into the vessel's hangar in order to be examined and receive first aid treatment.
1.17.1.7 First aid and medical services aboard Canadian Coast Guard vessels
In the event of medical emergencies or injuries at sea, vessels may have to divert to the closest port of refuge to evacuate the patient. The time taken to reach port or to evacuate the patient depends on many variables, including distance to be travelled, sea conditions, weather conditions, seaworthiness of the vessel, and speed of the vessel. The time taken to evacuate the patient may be measured in days. In this occurrence, the vessel was approximately 2 days from Resolute Bay, which was the closest port to which the 3 occupants could have been brought for further treatment had they survived.
According to the CCG Fleet Safety Manual,Footnote 99
the common source of reference to be carried aboard CCG vessels for emergency medical response is the International Medical Guide for Ships published by the World Health Organization. This publication has been adopted and endorsed by the International Maritime Organization and the International Labour Organization for seafarers.
The guide covers several topics, including death at sea and medical care for survivors at sea. According to the guide, the main vital signs that indicate how well the body is performing are body temperature, pulse rate and rhythm, respiration rate, blood pressure, and level of consciousness.Footnote 100
According to the International Medical Guide for Ships, “aperson who is suffering from hypothermia may look dead, but still be alive.” The Guide also indicates that:
A patient with moderate or severe hypothermia, especially if he is not shivering, requires external rewarming:
- place a waterproof sheet on a bunk, and lay the patient on the sheet;
- cover him with two or three blankets;
- put four towels (or other large pieces of cloth) into a bowl of hot water (about 40 °C), then put the dripping wet towels into four plastic bags;
- put the plastic bags on the patient's armpits and groin;
- after 10 minutes replace with fresh wet hot towels; and
- continue until the patient's temperature is over 32 °C.Footnote 101
In this occurrence, once recovered from the water, all 3 occupants were unconscious, showing no signs of breathing, and were all showing signs of drowning. Due to the lack of space inside the FRC, no first aid treatment or resuscitation manoeuvres could be attempted. Once brought into the vessel's hangar, vital signs, except for body temperature, were checked. None of the occupants was showing signs of breathing, and a pulse rateFootnote 102 could not be felt. They were all pale and had dilated pupils. CPR was attempted for a few minutes on the pilot, to no avail. He was pronounced dead at 1920, 15 minutes after being brought on board the vessel. Considering that the master and the scientist were showing similar physical conditions, it was felt that attempting CPR would also be unsuccessful. Therefore, no CPR was attempted on the master and the scientist, and both were pronounced dead shortly after their arrival in the hangar.
1.17.2 Transport Canada Aircraft Services Directorate
The Transport Canada Aircraft Services Directorate is responsible for the provision, maintenance, and modification of aircraft and for the provision of services in support of TC operations, as well as selected other federal government department and agency programs, such as the Canadian Coast Guard. This includes the provision of appropriate professional training to pilots, as well as to maintenance personnel. ASD is considered a commercial air carrier and operates in accordance with the CARs and CARs Standards. It holds operating certificates for operations under CARs subparts 702, 703 and 704.Footnote 103 The occurrence flight was conducted in accordance with CARs subpart 702.
ASD operates a fleet of 39 aircraft, consisting of 13 fixed-wing aircraft and 26 helicopters, including 14 BO 105s. The BO 105s are owned by the CCG but operated and maintained by ASD. ASD is the largest operator of BO 105s in the country, with 14 of the 18 BO 105s registered in Canada.
The TSB database shows that, in the 20-year period from 09 September 1993 to 10 September 2013, there were 4 BO 105 helicopters accidents in Canada;Footnote 104 the helicopters were operated by ASD. Two of these accidents were fatal.Footnote 105 There was no indication that any of these 4 accidents was caused by a mechanical problem. The TSB database also shows that a total of 20 mandatory reportable incidents concerning the BO 105 have been reported to the TSB: 8 of the incidents related to engine anomalies,Footnote 106 1 was related to a transmission gearbox malfunction, 1 was a declared emergency, 1 was a risk of collision in flight, and 9 were related to sling loads being released either intentionally or as a precautionary or emergency measure. The occurrence pilot was involved in one of the above reportable incidents (a sling load release in 1999).
1.17.3 Aircraft Services Directorate safety management system
The CARs do not require that the ASD have a safety management system (SMS). Nevertheless, ASD has been proactive in developing a fully integrated SMS and a safety program within its organization through its Safety Services Division. The role of the Safety Services Division is to provide services that support the fully integrated SMS and the safety program within ASD.
Since 05 June 2012, ASD has been considered a transitioning enterprise by TC Civil Aviation (TCCA), which means that ASD meets the following criteria set out in Civil Aviation Directive (CAD) 107-004, Aviation Enforcement – Safety Management Systems:
- The enterprise has an internal reporting program that is supported and promoted by the company's management.
- The enterprise has a reactive event analysis process adequate for determining root cause and developing corrective measures.
Since it is not yet a regulatory requirement, ASD's SMS has not yet been assessed by TC. However, ASD and all its operational programs are subject to oversight and review by TC. Surveillance activities carried out by TC on ASD have included audits, program validation inspections (PVI), and process inspections; these will be discussed later in the report.
ASD promotes a non-punitive reporting policy within its organization. Employees are encouraged to share information openly and to report any safety hazard, even if it involves operational errors, knowing that they will not be penalized for an unintentional error. From 01 December 2010 up to the day of the occurrence, a total of 11 hazard reports related to helicopter operations had been submitted to the Safety Services Division and recorded in the ASD hazard registry. The following were related to the BO 105 operations:
- Safety wire installed on the emergency float switch cover prevented the pilot from lifting the cover.
- Insufficient number of sleeping bags on board the aircraft for the number of passengers.
- Dry suit inefficient at keeping pilot warm to work outdoors.
- Unapproved installation of equipment could interfere with co-pilot's tail rotor pedal input, should dual control be installed.
- Debris hazard on ramp.
Except for the unapproved installation of equipment that could interfere with flight controls, all the other hazards reported have been followed up and their status is considered closed. The unapproved installation of equipment could only interfere with the co-pilot's tail rotor pedal input if the dual flight controls were installed. The occurrence aircraft was not equipped with dual flight controls other than the tail rotor pedals. However, these were locked and could not receive any accidental input by the front seat passenger.
1.17.4 Risk assessment
ASD conducted a risk assessment related to ice probe operations in late 2009. The risk assessment documentation indicated that the limitations of the ice probe equipment required the survey to be conducted at a height of 15 to 18 feet above the ice and at a speed of 70 knots. The hazard identified in the risk assessment was the inadvertent contact with the surface, known as controlled flight into terrain (CFIT),Footnote 107 due to the following possible scenarios:
- Distraction caused by any mechanical malfunction, such as a single engine failure, a master caution indication, or a warning tone, which can cause a lapse in concentration and result in a loss of altitude and ground contact.
- Lapse in concentration for any other reason, resulting in a loss of altitude and ground contact.
- Loss of situational awareness due to lack of, or loss of, suitable visual cues needed to determine aircraft attitude, which can cause a loss of altitude and result in ground contact.
- Failure to recognize a pressure ridge in the ice due to less-than-ideal visual cues or momentary distraction causing collision with the pressure ridge.
The risk assessment notes:
Scientific studies have determined that it takes the average person 2 to 3 seconds to recognize a change to a situation and a further 1 to 2 seconds to react. Flight in the conditions mentioned above leaves little time to react to a distraction or emergency.
Following the hazard identification and the risk associated with it, 3 options were examined to control the risk:
- Fly the survey at a higher altitude.
- Fly the survey at a significantly reduced airspeed, similar to hover taxi speed.
- Develop a set of operating procedures that
- minimizes forward speed, while respecting safe single-engine operating speed;
- limits the length of time spent operating at low altitudes;
- ensures low-level flights are conducted into wind whenever possible; and
- establishes minimum weather, visibility, and contrast limits.
It was noted that flying the survey at a higher altitude was the most effective means of reducing risk, but that the ability to do this depended on the limitation of the survey probe. It was also noted that assessing the capabilities of the equipment was beyond the scope of the risk assessment. A number of potential problems with flying the survey at a reduced airspeed were identified; most notably, the flight would be conducted below the single-engine best rate of climb speed of 60 knots.
The recommended risk control option retained was to establish procedures in the SOC (Appendix D) if it was not possible to fly the survey at a higher altitude. This option was accepted on 22 January 2010. In order to determine if the guidance in the catalogue was effective, post-flight interviews were conducted with CCG pilots in the fall of 2010 and again in January 2011, following survey missions. Based on these interviews, the guidance material was determined to be effective at mitigating the risk to an acceptable level in this operation.
However, a few months before these interviews, some CCG pilots had suggested that the time limit of 5 minutes spent flying at low altitude should be increased to 25 to 30 minutes. It was decided that 30 minutes was too long, and in most cases not necessary. Therefore, it was agreed that 15 minutes should be the maximum limit, and only under ideal conditions of contrast and visibility over a solid icepack. The SOC was not amended to reflect the increased duration of flight below 200 feet, and nothing indicates that a new risk assessment was done to determine the level of risk associated with this increased time limit.
The SOC reduces the maximum gross weight to 4850 pounds for low-level ice survey operations to allow single-engine climb performance. This maximum weight did not take into consideration the reduction of the rate of climb by 200 feet per minute when the engine anti-icing system is selected ON. However, in the event of an engine failure, the weight of the aircraft could have been reduced by 300 pounds per minute by using the fuel dump system.
1.17.5 Regulatory oversight of the Aircraft Services Directorate
Transport Canada has the regulatory responsibility for the oversight of the aviation industry. ASD holds a TC air operator certificate, is a TC-approved maintenance organization, and is considered to be a commercial operator.
Transport Canada is working to evolve its approach to conducting surveillance activities from one in which traditional inspections and audits were used to ensure compliance with regulations, to one which also examines systems to determine if they are effective at achieving compliance and if they are being used regularly. This change in approach is consistent with the move toward SMS; however this new approach is being used for all operators, whether or not they are required to have an SMS.Footnote 108
This can also be described as a systems approach to surveillance, since it aims to ensure that the enterprise has the appropriate systems in place and that these are working. TC defines a system as: “a group of inter-dependent processes and people working together to achieve a defined result. A system comprises policies, processes and procedures.”Footnote 109 As such, the focus in system level surveillance should be on the operators' policies, processes, and procedures.
In addition to SMS, this approach can be used to conduct oversight on any required system, which could include a quality assurance program or system, training system, maintenance control system, operational control system, weight and balance system, documentation control system, or emergency preparedness system.Footnote 110
1.17.6 Surveillance process
Transport Canada's Staff Instruction (SI) SUR-001Footnote 111 describes the procedures to be used by TCCA personnel when carrying out surveillance on civil aviation document holders. The document aims to provide TCCA with the tools necessary to ensure the enterprise has effective policies, procedures and processes to proactively manage risk, while encouraging the enterprise to take ownership of these processes and their continual improvement. Three types of surveillance activities are described: SMS assessments, PVIs, and process inspections. While all 3 types of surveillance will be used for enterprises required to have an SMS, only PVIs and process inspections are used for those not required to have an SMS.
The PVI is the routine surveillance method, replacing the traditional inspections. For subpart 703 and 704 air operator certificate holders, which are not required to have an SMS, the PVI is to focus on operational control and to be in sufficient depth to ensure that the certificate holder has processes in place to effectively provide operational control and to enable them to be in compliance with the regulations.
The process inspection examines a single process to determine if it meets regulatory requirements. It is intended to provide information to support decisions related to the level of risk associated with a certificate holder and the additional surveillance that may be required. Any process may be the subject of a process inspection, although templates were developed for the most commonly examined processes (e.g., training). Where a process inspection reveals safety related issues, a PVI may be conducted on an urgent basis to collect sufficient material to support the issuance of a formal report and certificate action,Footnote 112 if necessary.
According to Issue No. 04 of Staff Instruction SUR-001, when surveillance activities resulted in findings, document holders were required to provide a corrective action plan (CAP) to TCCA within 30 days of the surveillance report being completed. At a minimum, the CAP was expected to include a review of the non-conformance, a root-cause analysis identifying what caused the non-conformance to occur, proposed corrective actions, an implementation timeline, and confirmation of managerial approval for the corrective action. Failure to submit a CAP could result in a notice of suspension of the operating certificate.Footnote 113
The principal inspector was responsible for reviewing the CAP against the above criteria within 10 working days. If the CAP was acceptable, a plan for either administrative or on-site follow-up was to be produced and the certificate holder notified. If the CAP was deemed unacceptable, the certificate holder was notified of the deficiencies. A CAP which was found to be unacceptable could result in either the opportunity to amend the CAP or a notice of suspension. The former was preferred in cases where the changes required were simple and the time was expected to be short for the operator to amend the CAP and for TCCA to reassess it. The notice of suspension was reserved for CAPs requiring major changes. In the event a revised CAP was unacceptable, this version of TC's procedures indicated the principal inspector would issue a notice of suspension.
Certificate holders were informed of the timeframes and type of planned follow up when notified that a CAP had been accepted. The relevant principal inspector was expected to conduct the follow up and to close the finding when the corrective action had been completed. In the majority of cases, this was expected to be within 90 days. All findings for a PVI were expected to be closed within 6 months; a risk assessment was to be conducted if CAP implementation was outside this timeframe.
1.17.7 Transport Canada surveillance frequency
Transport Canada Civil Aviation's Civil Aviation Directive (CAD) SUR-008 identifies the frequency with which surveillance activities are to be carried out. Prior to the occurrence, the most recent PVI at ASD was conducted by TC in September 2011. The version of CAD SUR-008 in effect at that time indicated that all holders of certificates issued under parts III, IV, V, VII, and VIII of the CARs were to have a PVI every 12 months, unless specific risk indicators warranted a shorter interval.Footnote 114 The directive specified that this frequency was to be followed to the extent that resources would allow and that any deviation was to be communicated to the Director, Standards.
A revised version of CAD SUR-008Footnote 115 was issued on 25 May 2012. This new version indicated that the surveillance interval for a certificate holder is determined by means of a risk assessment, which takes into account factors such as the size and complexity of the operation, recent changes to the operation, and the history of the operator. The risk profile of an organization is to be updated annually. The directive provides a process for determining the organization's risk level and impact, which is then applied to a matrix to determine the surveillance interval rating. Enterprises with surveillance interval matrix ratings of 5D or 5E are to be subjected to a PVI every year. ASD had a rating of 5D (Appendix E).
1.17.8 The 2011 program validation inspection
The PVI conducted by TC in September 2011 resulted in 15 findings: 9 related to flight operations and 6 related to maintenance. The flight operations findings were related to operational control (3), flight and duty times (1), flight crew training records (2), company manuals (2), and flight documentation (1). Of the findings related to operational control, one was described as critical and another as major. The critical finding cited 2 incidents involving CCG helicopters as examples of a lack of operational control. The November 2011 letter communicating the results of the PVI to ASD indicated: “The organization failed to demonstrate that their Operational Control and Quality Assurance Programs conform to the minimum regulatory requirements as set out in CAR 571, 573, 605, 703, 704 and 706.”
On 16 December 2011, ASD submitted its first set of CAPs related to the 15 findings. These CAPs were evaluated by the principal TCCA inspectors and, on 01 February 2012, ASD was informed that 6 of the 9 flight operations CAPs and all 6 of the maintenance CAPs had been found to be unacceptable. The reasons provided related to a lack of analysis of the causes of the non-conformances, meaning the evaluating inspectors were not assured that ASD had properly identified and addressed the reasons for the non-conformances.
ASD was provided the opportunity to revise the CAPs that had been found to be unacceptable, with an original deadline of 10 February 2012. On 09 March 2012, ASD submitted a revised set of CAPs to TCCA. Assessment by the principal TCCA inspectors resulted in all of the revised CAPs being evaluated as acceptable on 16 March 2012. TCCA planned to complete administrative follow-up by the end of April 2012.
The revised CAPs provided more analysis of the causes for the non-conformances than the original submissions. Much of the corrective action was quite extensive. For example, in response to the flight operations findings, ASD indicated it planned to:
- undertake revisions to the company operations manual;
- implement a flight operations quality assurance program; and
- conduct a review of all shipboard helicopter operations procedures in concert with Coast Guard.
Given the scope of the corrective action proposed, ASD requested an extension on the deadline to provide a progress report to TCCA. This request was received on 15 May 2012, and an extension was granted until the end of June. At the end of June 2012, ASD submitted its follow-up response, which TCCA found unacceptable. TCCA met with ASD to review problems with the information provided. The findings of the PVI remained in open status, pending the implementation of the planned corrective action by ASD.
Also in June 2012, ASD was informed that TCCA considered it to be transitioning enterprise by TCCA. This designation, given to organizations who are voluntarily implementing an SMS, meant that TCCA had determined by means of a document review that the organization had an acceptable internal reporting program and reactive event analysis process in place. The designation meant that in the event of a non-intentional contravention of the regulations, TCCA would allow the certificate holder the opportunity to determine, by itself, proposed corrective measures to prevent recurrence.
Transport Canada Civil Aviation received the amended Company Operations Manual in September 2012. At that time, both corrective action related to the implementation of flight operations quality assurance and the review of shipboard procedures for helicopter operations were still outstanding.
At the time of the occurrence, in September 2013, the findings from the 2011 PVI — including the critical finding related to operational control — remained open, because TCCA had not received assurance that the actions proposed by ASD in the corrective action plans had been successfully implemented.
No new PVI was initiated prior to the occurrence, since the 2011 PVI had not been closed.Footnote 116 No certificate action was taken, as TCCA was continuing to work with ASD to ensure the corrective actions stipulated in the CAPs were implemented.
1.17.9 The 2013 process inspection
Following the occurrence, TCCA initiated a process inspection focused on CCG rotary wing operations. Conducted from 25 September 2013 to 06 December 2013, the inspection evaluated processes related to operational control, the safety oversight component of ASD's SMS and ASD's flight crew training program. In addition to the accident, the initiating causes of the process inspection were ASD's increasing risk indicator and its ongoing difficulties meeting CAP commitments following the 2011 PVI. The risk indicator is generated by the National Aviation Safety Information Management System which tracks information on the operator on 10 hazard areas. In the case of ASD, recent incidents and the number and scope of findings from the 2011 PVI would have increased its risk indicator.
As a result of the process inspection, TCCA became aware of a number of issues with the manner in which the ice probe operation was being conducted. Specifically, the regulator took exception to the fact that the procedures relating to the ice probe operation were published outside of the Company Operations Manual (COM) and that there were no formal ground or flight training programs relating to the operation.
The 9 findings resulting from the process inspection are summarized below:
- Operational Control—Aircraft Limitations (Moderate): No process was in place to ensure operational procedures were kept up-to-date with rotorcraft flight manual (RFM) revisions and a number of RFMs were found to be out of date.
- Operational Control—Aircraft Dispatch (Moderate): Discrepancies were noted in weight and balance information between different sources used by flight crews.
- Operational Control—Information Dissemination (Moderate): Flight crew guidance for the ice probe operation was introduced outside of the COM. In addition, operational restrictions put in place following the accident were communicated verbally and by e-mail and were not based on a documented risk assessment.
- Operational Control—Carriage of Persons (Moderate): In addition to guidance material being published outside of the COM, no training program related to the ice probe operation was provided. Further, the master of the CCGS Amundsen was carried on board during the flight, although his presence was not essential during the ice probe portion of the flight.
- Operational Control—Over Water Flights (Major): The procedure for ice probe flights was not validated to ensure float inflation requirements were met. Also identified were several instances where pilots had not been issued immersion suits and one instance where a pilot without an immersion suit had been dispatched for an overwater flight that met immersion suit criteria.
- Training Program—Aerial Work (Major): Procedures for ice probe flights were introduced outside the COM; no ground or flight training program was approved and a briefing/self-study was deemed to be acceptable for initial and recurrent training for the ice probe flights.
- Operational Control—Flight Planning (Major): Deficiencies were noted in the COM with respect to the requirement for operational flight plans and the retention of operational flight plans.
- Training Program—Flight Crews (Major): Deficiencies were noted in pilot training records. In particular, no records of surface contamination and winter operations training were available, and flight operations were voluntarily suspended until the training could be completed.
- Operational Control—Crew Dispatch (Moderate): Instances were noted where pilots were dispatched as PIC [pilot-in-command] without the required flight experience; it was also noted that no process was in place for flight authorizations, tasking or manifests.
1.18 Additional information
1.18.1 Operational control
As required by Commercial Air Service Standards section 722.12, “operations conducted under Subpart 702 of the Canadian Aviation Regulations require, as a minimum, a Type D operational control system,” which was the case for the occurrence flight. Flight following for a Type D system consists of monitoring a flight's progress and notifying the appropriate air operator and SAR authorities if the flight is overdue or missing. Operational control is delegated to the pilot-in-command of a flight by the operations manager, who retains responsibility for the day-to-day conduct of flight operations.
1.18.2 Flight following and flight watch
The Operations Manual, Canadian Coast Guard Helicopters, Part 2, section 2.6.1 states that, “A flight watch system is required to continuously monitor night visual flight rules (VFR) flight from initial take-off to final destination”. Since this occurrence was conducted in day VFR conditions, there was no requirement to continuously monitor the flight's progress. According to the Operations Manual, Canadian Coast Guard Helicopters, Part 1, section 4.29, when CCG helicopters are assigned to CCG vessels, the flight following and monitoring of the flight progress of all flights are provided by the facilities on the vessel.
1.18.2.1 Bridge activities during helicopter operations
Procedures for shipboard helicopter operations are contained in the Shipboard Helicopter Information and Procedures Manual and are complemented by the Fleet Safety Manual DFO/5737, the Operations Manual – Transport Canada Helicopters and Masters Standing Orders. The Shipboard Helicopter Information and Procedures Manual outlines the responsibilities, chain of command and general duties of specific individuals and groups during flight operations. Roles for bridge operations are defined only while the helicopter is taking off and landing.
On the day of the occurrence, while the helicopter was in flight, the vessel was being maneuvered for tasks related to the scientific mission. Specifically, the vessel was being maneuvered through ice by the first officer, as officer of the watch, in order to find a specific size of ice floe. Since the master was on board the helicopter, the chief officer (CO) assumed responsibility for the vessel and its crew, and he was on the bridge supervising the scientific work and standing by for the helicopter. The CO is authorized to act in the master's absence to make decisions and to take control of the vessel's movements as required. In addition to the CO, the first officer and his wheelsman and the second officer and his deck crewman were standing by on the bridge while waiting for the helicopter to return.
At approximately 1740, the second officer and the deck crewman left the wheelhouse to prepare the flight deck for the helicopter's arrival when they heard that the ETA was in 10 minutes. The vessel continued its maneuvers. At 1818, once informed that communication with the helicopter had been lost, the CO assumed control of the vessel from the first officer, and ordered and supervised the SAR effort.
1.18.3 Flight following system
1.18.3.1 General
At the time of the occurrence, the Coast Guard was in its first season with a new FFS. The system was still considered to be in development, as it had passed 2 of the 3 acceptance testing phases specified in the contract with the supplier. A new FFS was required because the existing system (NavLink) was becoming difficult to maintain as it was reaching the end of its useful life.
CCG's Integrated Technical Services (ITS) oversaw the development and implementation of the FFS. This involved developing a statement of requirements (SOR) in consultation with CCG Fleet, and identifying possible solutions to meet the requirements. Research conducted by ITS concluded that there was no commercially available solution that fully met the stated requirements. The most expedient means of developing the system was to use commercial off-the-shelf hardware with a customized user interface and customized software.
1.18.3.2 Statement of requirements
The specifications contained in the SOR are summarized below:
- The system shall allow the tracking of aircraft from vessels as a stand-alone system and from shore over a Web-based service.
- The system must provide the ability to track a CCG helicopter from a vessel and vice versa as a stand-alone unit, displaying the asset call sign, position, bearing and distance.
- Aircraft equipment must be certified for aircraft use and an STC [supplemental type certificate] shall be provided to permit installation on all helicopter types in the CCG fleet.
- The system must be operable in all weather conditions at all latitudes.
- Position information shall be provided by the unit's own GPS and be accurate to within 30 m.
- The same display used on the helicopter is acceptable on the vessel.
- The helicopter position shall be broadcast every 2 minutes. This shall be able to be increased to every 30 seconds.
- The vessel's position shall be broadcast every 4 hours. This shall be able to be increased to every 2 minutes.
- The system shall be capable of being manually selected to transmit an emergency signal and position report with notification to a pre-selected list of contacts and any asset tracking the helicopter/vessel. “This notification must be immediately evident to the receiver and require acknowledgement before being removed from the receiver's system.”
- The foot print of the interface should be as small as possible.
- The system should not require extensive training to be operated.
- Appropriate training shall be provided to pilots and vessel's officers “in collaboration with the manufacturer.”
- Appropriate training shall be provided to TC and CCG technicians “by the manufacturer.”
There were no additional requirements with respect to the characteristics of the user interface, such as the display of latitude and longitude. There was no requirement for an aural alarm for an aircraft in emergency or in the case of an overdue aircraft, since it was believed that the wheelhouse crew would be monitoring the display.
1.18.3.3 Flight following system architecture and interface
Vessel officers and helicopter pilots can obtain each other's position information using the FFS through a control display unit (CDU) that combines 2 units—a CDP300 (serial number 104-300-01) and a DVI300 (serial number 105-300-01). On board the helicopter, the CDU is located at the bottom center of the instrument panel. On the CCGS Amundsen, the CDU is located at the chart table on the aft, starboard side of the wheelhouse (Figure 10).

While the previous NavLink system relied on a direct HF radio link between the vessel and the helicopter, the SkyTrac FFS employs GPS position reports transmitted via a satellite communication system and managed by SkyTrac's data centers. These position reports are transmitted at the user-specified position interval (PI) and these position reports are used by the Web-based SkyWeb application for the purposes of tracking an asset (helicopter or vessel). The default PI is 4 hours for the vessel, and 2 minutes for the helicopter. The PI determines the frequency at which the vessel and helicopter positions are automatically sent to the server. Position reports are also sent to the server manually via CDU selections made by the user.
At the time of the occurrence, the Shipboard Helicopter Information and Procedures Manual had not been updated to reflect the use of the new FFS, which was still in the development phase. According to the manual, the responsibility for monitoring the NavLink equipment during flight operations rests with the officer of the watch. Pending amendment to the manual, the CCG issued the Operations Circular (OC 07-2013) in June 2013, which outlined standard operating procedure (SOPs) for the use of the new FFS.
The SOPs stated that, prior to commencing helicopter operations, the vessel crew must perform the following on the FFS CDU:
- Change its position interval (PI) from 4 hours to 2 minutes to ensure that the vessel and the helicopter receive position information every 2 minutes.
- Select the appropriate helicopter from the rendezvous list and initiate the rendezvous.
- Terminate the rendezvous function on both the helicopter and vessel, and reset the PI to 4 hours on the vessel once helicopter operations are terminated.
However, the SOPs did not specify who was responsible for changing the PI and initiating the rendezvous function, or who monitors the CDU display for position or overdue information.
When the rendezvous function is initiated, the position reports received are used by the server to calculate bearing and distance information and then return the following rendezvous information for the paired asset:
- bearing and distance
- latitude and longitude
- time stamp of the position.
This position information is updated on the CDU after the vessel position is sent to the server, either manually or automatically. Position reports are sent to the server automatically based on the PI setting or manually via CDU selections made by the user.
By scrolling through the menus on the CDU, users have the option of displaying either the latitude and the longitude or the bearing and distance. In both cases, though, the asset tag identification and the time stamp will be displayed (Figure 11). The time stamp is displayed on the CDU to indicate the time at which the position is valid.
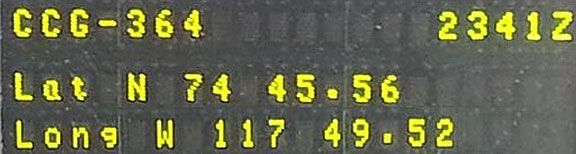
The CDU rendezvous information screen does not indicate the current PI. The user must select the appropriate system screen or compare the time stamp of the displayed position to the actual time. In this occurrence, a time stamp more than 2 minutes old would have indicated that the PI was not set to 2 minutes, and so may have remained at 4 hours.
The latitude and longitude position is meant to be displayed as degrees, minutes, and seconds on the CDU. The dot was added for display purposes only, and does not affect the position in itself: the bearing and distance information provided is accurate. However, the dot displayed between the minutes and the seconds may mislead users to interpret the position as degrees, minutes and hundredths of a minutes (Figure 11).
1.18.3.4 Flight following system notifications
There are 2 notifications provided aboard the vessel to indicate the helicopter may be in distress or overdue. Both provide visual indications only but there is no aural indication to draw the vessel crew's attention to the FFS. The 2 notifications are:
- Emergency—when triggered by the emergency switch on the helicopter CDU, the unit on the vessel will indicate the asset tag (in this case, CCG364) and the word emergency.
- Overdue / Missing Position Report —When rendezvous is engaged and a predefined number of position reports are missed, the asset tag (in this case, CCG364) will be replaced with a series of dashes. This notification may be a result of an interuption in satellite communication or the occurrence of a safety event. Since in this occurrence it was the result of a safety event, the term “overdue notification” alone will be used. The elapsed time before this notification is displayed depends on the CDU system settings on the helicopter and the vessel. The default is 3 missed position reports.
Since both the helicopter and the vessel should use a 2 minute PI, dashes should appear when position information is more than 6 minutes old. It was decided to use a dashed asset tag to indicate an overdue notification to minimize distractions created by aural or visual alarms in the helicopter.
A Web-based service (SkyWeb)Footnote 117 is available so that the stream of position reports received from helicopters and vessels can be monitored from shore. If SkyWeb detects that 5 position reports are missed, it will send a different type of overdue notification via e-mail to a pre-selected list of contacts, indicating that the helicopter missed a number of position reports or is late. These missed position reports could also be the result of a safety incident or satellite communications issues. An emergency notification e-mail will also be sent if the emergency switch on the helicopter is activated.
In this case, the Web service was initially set up to send the messages to designated recipients within the CCG Regional Operations Center, the Marine Rescue Sub-Centre and ASD. However, the FFS units were not configured to distinguish between “on ground” and “in flight” status and all position reports were considered “in flight”. As a result, several false overdue notifications were received when the helicopter was on the ground and located in the hangar. Consequently, all contacts from the overdue notifications list were removed in July 2013 until further investigation could be conducted with the manufacturer to understand what was causing these erroneous notifications and to find a way to resolve the issue. The contacts were still able to receive the emergency notifications.
1.18.3.5 Flight following system implementation and training
The new FFS had successfully completed the first 2 contract milestones (factory acceptance testing and site acceptance testing) prior to the start of the 2013 Arctic operating season. Full capability acceptance testing was due to be completed at the end of the contract.
For the 2013 operating season, only part of the CCG helicopter fleet had been equipped with the new FFS. Consequently, some vessels were equipped with both the SkyTrac FFS and the previous NavLink FFS and would use the system the helicopter assigned to the vessel was equipped with.
Given time constraints, a train-the-trainer approach was used to train pilots and vessel crews in the use of the system prior to the 2013 operating season. Training was provided to a group of CCG personnel who adapted the materials from this training and provided a briefing to supervisory pilots by webinar.
For the purposes of training vessel officers, technicians who would be travelling on vessels equipped with the new system attended the same briefing attended by the pilots. It was expected that the technicians would then use the training materials to brief the vessel's crews on the use of the system. Four navigation officers on board CCGS Amundsen were provided a demonstration of the new FFS by the technician.
The training materials provided to vessel officers, technicians and ASD pilots indicated it was necessary to set the PI to 2 minutes to ensure that each asset using the system received the most up-to-date information with respect to the other. The materials did not specifically describe the FFS's overdue notification functionality or the importance of the PI setting and the role it played in overdue notifications.
With respect to the importance of the time associated with a position report, the training materials provided by the contractor described the position as being the current distance and bearing to the asset. As such, the importance of validating the time of the position report was not emphasized.
1.18.3.6 Position interval on Canadian Coast Guard Ship Amundsen in the days preceding the occurrence
At 0745 on 05 September 2013, during helicopter operations, the FFS on the CCGS Amundsen began broadcasting regular position reports every 2 minutes, indicating that the PI had been manually set to 2 minutes as required during helicopter operations. However, the shipboard FFS continued to send position reports every 2 minutes for the next 3 days, even though no helicopter operations were taking place. At 0842 on 08 September 2013, the crew set the PI back to the default of 4 hours on the shipboard FFS.
1.18.3.7 Position interval on the day of the occurrence
On the day of the occurrence, just prior to takeoff, the rendezvous function was active on both the helicopter and the ship. However, the wheelhouse crew encountered difficulties changing the shipboard PI from 4 hours to 2 minutes. While trying to set the PI to 2 minutes, the wheelhouse crew was distracted by other duties related to the vessel operations and the shipboard PI was not changed.
Seventeen minutes after the takeoff, the crew contacted the pilot to advise that the shipboard FFS was still indicating the helicopter position at 0 miles from the vessel. This indicates that the PI on the vessel was not set to 2 minutes.
The server logs for the CCGS Amundsen confirm that it did not transmit regular position reports every 2 minutes on the day of the occurrence. However, the logs show that CCGS Amundsen position reports were received at 1703, 1755, 1805 and 6 times at irregular intervals until 1826, when regular position reports resumed every 4 hours. This indicates that the wheelhouse crew updated the CDU at these times between 1703 and 1826. When the server receives position reports, bearing distance is calculated and returned with a time stamp, and the shipboard CDU then displays helicopter position information with a time stamp.
At 1755, the time stamp for the helicopter position information was 1741, the last helicopter position received by the server. At that time, the CDU asset name tag (CCG364) was replaced by dashes to indicate an overdue notification. The crew did not notice that this position was 14 minutes old.
At 1805, the FDO waiting for the helicopter on the flight deck radioed the wheelhouse crew to query the helicopter position. The wheelhouse crew checked the FFS CDU and confirmed that the helicopter was at 3.2 nm from the vessel. The time stamp was still 1741, the time of the last helicopter position received by the server; the crew did not notice that this helicopter position was now 24 minutes old.
At 1826, while the CCGS Amundsen was heading for the last known position, the wheelhouse crew realized that the time stamp was 45 minutes old.
The server logs for CCG364 show the helicopter power-up at 1632, takeoff at 1638 and regular position reports every minute, with the last report at 1741. It could not be determined why the pilot's CDU was set to 1 minute instead of the default 2 minutes.
1.18.3.8 Standards for warnings and alerts
No specific user interface design standards were referenced by CCG for the development of systems to be installed on vessels. Many standards are available to help guide the development of user interfaces. The FAA has compiled a Human Factors Design Standard which is a compilation of relevant standards and guidance for use in the development of FAA systems. It is a useful reference for understanding user interface issues since it brings guidance material for a range of subjects into one place with citations provided to the original source.
Relevant guidance includes the following:
If equipment is not regularly monitored, an audio alarm shall be provided to indicate malfunctions or conditions that would cause personnel injury or equipment damage. [Source: Department of Defense (MIL-STD-1472F), 1999]
Alarm systems should:
- Alert the user to the fact that a problem exists,
- Inform the user of the priority and nature of the problem,
- Guide the user's initial responses, and
- Confirm in a timely manner whether the user's response corrected the problem. [Source: Nuclear Regulatory Commission (NUREG-0700), 1981]
Provide redundant visual warning. All non-verbal audio signals shall be accompanied by a visual signal that defines the condition. [Source: MIL-STD-1472F, 1999]
Avoid startle. Signals should not be so startling that they preclude appropriate responses or interfere with other functions by diverting attention away from other critical signals. [Source: MIL-STD-1472F, 1999]
Out of range indicators. When equipment has failed or is not operating within tolerance limits, an indication shall be provided. [Source: NASA-STD-3000A, 1989; MIL-STD-1472D, 1989; MIL-STD-1800A, 1990]
1.18.4 Ice probe operations
In order to provide guidance to pilots for an ice probe operation, an SOC was developed (Appendix D). The SOC indicates that, during data collection, the aircraft should be flown at no less than 20 feet above the ice surface for short periods of time, usually no more than 5 minutes, and at a speed of no less than 60 knots and no greater than 80 knots.Footnote 118 As stated earlier, the pilot conducted a total of 6 survey runs ranging from approximately 7 to 9 minutes each, except for the last run leading to the impact, which lasted about 3 minutes.
According to the SOC, only essential persons shall be on board the helicopter during survey operations. In this occurrence, the flight was combining 2 types of operations related to aerial work: ice measurement and ice reconnaissance.
Transport Canada's TP 8880Footnote 119 defines the different types of operations related to aerial work conducted by aeroplanes or helicopters. The term given to the operation of an aircraft for the purpose of conducting aerial observation and patrols for surface events, objects, and animals is aerial inspection and surveillance. This definition applies to the ice reconnaissance conducted by the master during the occurrence flight.
In TP 8880, aerial surveying is defined as “the operation of an aircraft for the purpose of surveying by use of a camera, or other measuring and recording devices.” This would apply to the ice measurement mission conducted by the scientist.
CARs paragraph 702.16(a) states, “No air operator shall allow a person who is not a flight crew member to be carried on board an aircraft unless the person's presence on board is essential during the flight.” Since they were both assigned to duty during flight—measurement duties by the scientist and observation duties by the master—they both met the criteria of crew member as defined in section 101.01 of the CARs.Footnote 120 Furthermore, the presence of the scientist and the master was essential during the flight, as per subsection 702.16(a) of the CARs.
The SOC also states that for low-level ice survey operations, the maximum gross weight of the helicopter shall not be more than 4850 poundsFootnote 121 to allow single-engine climb performance. However, this maximum weight limit did not take into consideration the reduction of the rate of climb when the engine anti-icing system is selected ON.
The helicopter was refuelled on 08 September to a total of 125 U.S. gallons and had not been flown again until the occurrence flight. Based on the actual occupants' weight and the equipment on board, it was determined that the helicopter took off at a weight of 5268 pounds. Considering the flight time of approximately 65 minutes with a fuel consumption of about 45 U.S. gallons per hour,Footnote 122 the weight at the time of the crash would have been approximately 4942 pounds. At that weight, and considering the actual outside air temperature of −1.4 °C and sea level as pressure altitude at the time of the occurrence, the single-engine rate of climbFootnote 123 would have been approximately 140 feet per minute compared with 180 feet per minute at 4850 pounds with the engine anti-ice OFF and the maximum continuous power applied.Footnote 124 The rate of climb would have been similar with the use of emergency power.Footnote 125 However, the BO 105 RFM states that the rate of climb is reduced by 200 feet per minute if engine anti-ice is selected ON.Footnote 126 The engine anti-ice switches were found in the ON position during the initial wreckage examination, and the engine examination revealed that the engine anti-ice valves were open at the time of the occurrence.
According to the SOC, pilot initial and recurrent training records must be kept. However, there was no record indicating that the pilot had undergone initial and recurrent training related to the ice probe operations. It could not be determined if the pilot had reviewed the SOC as part of the recurrent training before the occurrence flight.
1.18.5 In-flight emergencies
Section 3 of the BO 105 approved RFM contains the recommended procedures for coping with various types of emergencies, malfunctions, and critical situations. ASD pilots also refer to the BO 105 Pilot Checklist. The checklist includes the normal operations checklist, the malfunctions checklist, and the emergency procedures.
Most in-flight emergency situations will be indicated by either a red warning light on the warning panel or an amber caution light on the instrument panel. The illumination of any of the red warning lights indicates an emergency condition requiring immediate corrective action. However, the primary consideration is to maintain control of the helicopter before taking any corrective action specified in the emergency checklist. Amber caution lights on the instrument panel indicate a malfunction or a failure condition. None of them require immediate crew action, but indicate the possible need for future corrective action.
The RFM states that it is always possible that a warning/caution light will come on unnecessarily. In such cases, whenever possible, the pilot should check the light against its associated instrument to verify that an emergency condition actually exists. Based on the emergency encountered, the associated checklist provides the following options for landing:
- Land immediately;Footnote 127
- Land as soon as possible;Footnote 128
- Land as soon as practical.Footnote 129
According to the RFM and the BO 105 Pilot Checklist, there are 2 conditions that would require the aircraft to land immediately:
- The main rotor transmission oil pressure is below 0.5 bars and/or the transmission temperature is above 105 °C.
- The main transmission chip light illuminates combined with the illumination of the transmission oil warning light and transmission temperature and pressure are abnormal.
According to the RFM and the BO 105 Pilot Checklist, the following conditions would require the aircraft to land as soon as possible:
- Engine fire in flight;
- Electrical fire;
- Main rotor transmission oil pressure is normal and temperature is above 105 °C;
- Main transmission chip light stays ON;
- Single engine failure;
- Severe pedal vibration;
- Battery over temperature;
- Electrical short circuit;
- Dual fuel filters clogged;
- Oil cool light illumination with engine or transmission temperature nears limit; and
- Obstructed baffle assembly.
1.18.6 Bird hazard
The following information is a summary of TC publication TP 13549, Sharing The Skies - An Aviation Industry Guide to the Management of Wildlife Hazard.
According to this document, helicopter operations are constantly exposed to the risk of bird strikes since the majority of helicopter flight operations are conducted at very low altitudes, typically below 500 feet agl. The pilot's concentration is focused on maintaining terrain clearance while completing the assigned task; there is little or no time available to watch for birds.Footnote 130
Helicopters are more of a disturbance to bird colonies than fixed-wing airplanes; strike risk is therefore increased when birds are flushed into the air. There is significant risk of birds penetrating the windshield and causing serious injury and incapacitation.
The majority of day-to-day bird movements occur between 30 and 300 feet above ground level (agl). Little regular activity occurs above 1000 feet agl, so it is not surprising that over 80% of reported bird strikes occur when aircraft are below that level; the vast majority of strikes happen below 300 feet agl.
Most North American bird species (60 to 80%, or more than 5 billion birds) migrate each fall to the southern U.S., Mexico—and as far as Central and South America—only to make the journey back in the spring. During these migration periods, enormous numbers of birds move across the entire North American continent. There is no question that migration periods (September to October and April to May) are times when there is great risk of a serious bird strike.
The greatest immediate danger to helicopter pilots following windshield penetrations is loss of vision from flying debris. This is why TP 13549 suggests, among other operating techniques, that helicopter pilots always wear a helmet with the visor in order to help reduce the severity of bird strikes. In this occurrence, the pilot was wearing a helmet, but it could not be determined if its visor was down prior to the crash. The helmet examination did not reveal any sign of bird impact that could have interfered with the pilot's vision.
The bird activity level in the vicinity of the crash the day of the occurrence is unknown. Pictures taken that day and videos taken during the occurrence flight did not show evidence of bird activity. The wreckage examination did not reveal any signs of a bird strike. Therefore, the probability that the pilot had been distracted by the presence of birds or had to take evasive action to avoid a flock of birds is remote. However, it cannot be completely ruled out.
1.18.7 Visual cues
In addition to a discernible horizon, which is essential to judging aircraft attitude during visual flight, the visual cuesFootnote 131 that are relevant to the task of judging altitude during low-level flight include:
- Linear perspective: the degree of convergence between parallel lines reduces with increased height above the surface (splay);
- Interposition: the space between objects appears to decrease as one approaches the surface (compression);
- Light and shadow: the relative position of shadows will change with increase in height above the surface;
- Relative (familiar) size: objects will appear smaller as height above the surface increases;
- Textural gradient: surface texture appears finer (less detail) as height above the surface increases; and
- Optical flow: the rate at which objects appear to flow outwards from a central point decreases with increased height above the surface.
Figure 12 illustrates examples of the visual cues available for height keeping during an ice measurement flight. The pilot needs to maintain a continual scan in 3 areas: the near visual field, the distant visual field and the aircraft instruments—particularly, the ice probe radar altimeter and the airspeed indicator. The relative importance of each area depends on cues available and the pilot would need to adjust the scan to focus more attention on the instruments in areas where there are fewer visual cues available outside the aircraft.
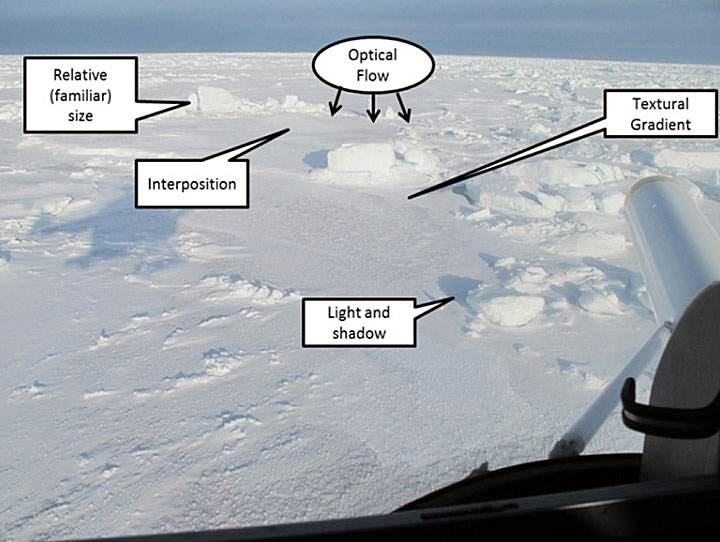
1.18.8 Controlled flight into terrain
Controlled flight into terrain (CFIT) is an occurrence in which an aircraft, under the control of the crew, is flown into terrain, water or an obstacle with no prior awareness on the part of the crew of the impending disaster.Footnote 132
In the 3 videos examined, the helicopter passed over small patches of open water. The largest patch of open water was crossed in approximately 5 seconds. The texture of the water surface varied; some patches had ripples on the surface and others were flat and shiny and appeared to have a thin layer of ice.
At the time of the occurrence, the winds were reported as light. Under such wind conditions, the smooth water surface presents a uniform appearance from above, somewhat like a mirror. This situation affects visual references for the pilot and can be extremely dangerous, especially when flying close to the surface. If clouds or ice floes are reflected from the water surface, the resulting perception of being at a higher altitude may lead even experienced pilots to descend, resulting in a CFIT accident.
1.19 Useful or effective investigation techniques
1.19.1 Recovery vessel
The recovery of the helicopter from the M'Clure Strait in September presented some significant challenges. The CCGS Amundsen, the CCGS Henry Larsen and their crews, with the support of the ROV operators made available by ArcticNet, allowed the recovery team to overcome these challenges.
1.19.2 Wreckage location
The TSB and ROV team boarded the CCGS Amundsen in Resolute Bay on 19 September 2013, and arrived in the accident area on 21 September 2013. Vast floes in the search area precluded the use of a grid search pattern. The initial search was planned with the use of a hydrophone to listen for the signal transmitted from the onboard ULB. Since a steady and consistent beacon signal could not be detected, the search for the wreckage was planned to be performed with the ROV, based on a calculated point of impact. An unusual radio transmission was heard at 1742:59 on the vessel's VDR. It was hypothesized that the CCG364 might have been the source and the time was used as the time of impact.
The shipboard FSS CDU displayed the last position of the helicopter as N 74 45.56, W 117 49.52Footnote 133 at 1741, but it did not keep a record of previous positions. Therefore, the track leading to this last position was not available to calculate a position line for the search. However, positions recorded every minute on the Web server (SkyWeb) were provided to the TSB team before boarding the CCGS Amundsen. The last recorded position on the Web server was N 74 45.95, W 117 49.88 at 1741:42.
The difference between the last interpreted position from the shipboard FFS CDU and the last position retrieved from the SkyWeb server log was 743 m, nearly perpendicular to the helicopter trajectory. In order to verify the accuracy of the positions recorded on the SkyWeb server, the position of the helicopter while on the flight deck just prior to takeoff was used. It was established that the positions of the vessel and the helicopter matched exactly just prior to takeoff at 1637. Therefore, the SkyWeb log positions, the derived ground speeds, and tracks were used to estimate the position of the helicopter at the hypothesized time of impact of 1742:59, resulting in position of N 74 45.8080 W 117 44.2850.
At 0805 on 23 September 2013, the ROV reached the sea floor for the first time, 458 m below the surface, to commence searching for the wreckage of CCG364. At 0822, the first piece from the helicopter was found and the main wreckage was found approximately 170 m further along the calculated trajectory 5 hours later, at 1322.
1.19.3 Wreckage recovery
On 24 September 2013, vast floes over the wreckage location precluded recovery operations. With the presence of sustained strong southeasterly winds, the ice continued to drift to the north, leaving larger areas of open water between ice floes. The CCGS Henry Larsenwas tasked with diverting the ice pack and breaking larger floes in the vicinity of the recovery operation. The CCGS Amundsen was able to maintain the desired position above the wreckage and commence the recovery operations on 25 September 2013. The mooring kit was lowered to the sea floor approximately 40 m from the helicopter wreckage.
At 0858, the ROV reached the mooring kit, wrapped the lanyards around the helicopter landing gear mounts and attached it to a Kevlar rope that was used to raise the wreckage to the surface and place it on the front deck of the CCGS Amundsen at 1430 (Photo 8).

The wreckage was transferred to the CCGS Henry Larsen for the voyage back to St. John's, Newfoundland and Labrador, and then transported by truck to the TSB laboratory in Ottawa, where it arrived on 22 October 2013.
2.0 Analysis
2.1 Introduction
There was no radar information for the accident flight, no witnesses to the accident, and no survivors. Some information was available from the helicopter on-board SkyTrac system. The aircraft was not fitted with a flight data recorder (FDR) or a cockpit voice recorder (CVR), nor was it required to be by regulation. Had the aircraft been fitted with at least a lightweight flight recording system that could record cockpit image, cockpit audio, aircraft parametric data, and/or data-link messages, investigators would have been able to better understand the circumstances and events that led to the accident. The data from a lightweight flight recording system would have become a primary tool in the investigation. If cockpit or data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
The pilot was certified and qualified for the flight in accordance with existing regulations. The investigation determined that there was nothing to indicate that the pilot's performance was degraded by fatigue or physiological factors.
This flight was a combined ice measurement and reconnaissance mission and was conducted at very low altitude above the ice surface before the aircraft struck an area of open water. All occupants survived the impact and managed to evacuate, but none of them survived.
The following suggest that the onset of the accident was sudden:
- The pilot did not make a distress call.
- The pilot did not activate the flotation system to execute a ditching.
- The pilot did not activate the emergency switch on the flight following system (FFS).
- The pilot did not activate the emergency locator transmitter (ELT) via the cockpit switch.
The following suggest that there were no anomalies with the helicopter that could have forced the pilot to land immediately or could have caused a loss of control and crash:
- There were no technical defects reported before or during the flight.
- Images taken in flight showing the engine instruments did not indicate an impending mechanical malfunction.
- After the pilot's last call to report the estimated time of arrival (ETA), there was no indication that the pilot climbed to a safe altitude above 200 feet to assess any abnormal or emergency condition as required in the Speciality Operations Catalogue (SOC).
- The pilot did not make a distress call.
- There was no indication that the flotation system was activated to carry out a ditching.
- The examination of the engines revealed they were operating during the impact sequence.
- The examination of the flight control continuity and integrity revealed no anomalies.
- The calculated average rate of descent was not consistent with a loss of control.
- The impact damage signature did not support a loss of control.
The task of controlling aircraft altitude in low-level flight requires adequate visual cues to accurately judge the height of the aircraft over the ground or water. Difficulties can arise from either a lack of visual cues or misleading visual cues, which result in visual illusions. A lack of visual reference as the aircraft was flying over an area of open water is consistent with the facts of the occurrence and cannot be ruled out.
This analysis will focus on the following:
- The ice probe operation and installation.
- Visual cues.
- The FFS and its implementation.
- Survivability.
- Regulatory oversight.
2.2 Ice probe operation
Despite the risk associated with low-level flying, there are some legitimate reasons for flying at low level, including aerial work such as ice measurement operations. Based on a risk assessment made by the operator in 2009, the risk level associated with a controlled flight into terrain (CFIT) was determined as high due to the following possible scenarios:
- distraction caused by any mechanical malfunction, such as a single engine failure, a master caution indication, or a warning tone, which can cause a lapse in concentration and result in a loss of altitude and ground contact;
- lapse in concentration for any other reason, resulting in a loss of altitude and ground contact;
- loss of situational awareness due to lack of, or loss of, suitable visual cues needed to determine aircraft attitude, which can cause a loss of altitude and result in ground contact; and
- failure to recognize a pressure ridge in the ice due to less-than-ideal visual cues or momentary distraction causing collision with the pressure ridge.
In order for the pilot to relax his concentration level and manage the onset of fatigue and distraction, the SOC limited low flying to short periods of time, usually no more than 5 minutes. This was increased to 15 minutes in June 2010, following discussions with Aircraft Services Directorate (ASD) pilots and human factors specialists. However, no new risk assessment was done to determine the level of risk associated with this increased time limit. Since 66% of the 65 minute flight was spent at low altitude, it is possible that the pilot's concentration was reduced to a point that the shallow descent was not recognized in a timely manner to prevent the impact.
The aircraft examination did not reveal any anomalies that could have played a role in this occurrence. The examination of the bulb filaments from the annunciator panel showed no sign of elongation or stretching. Although this could indicate that all bulbs were OFF at the time of impact, this could also indicate that the impact forces to the annunciators were insufficient to cause the deformation that would normally be associated with an ON indication for an incandescent bulb. Therefore, the possibility of pilot distraction caused by the illumination of a warning light, even momentarily, cannot be ruled out. Furthermore, a brief distraction caused by other crew members on board or the presence of birds in the vicinity could also have caused a lapse in the pilot's concentration, resulting in the loss of altitude and water contact.
The fact that the helicopter departed at a weight above 4850 pounds, the maximum gross weight stated in the SOC, did not play a role in this occurrence. This maximum weight limitation is to allow single-engine climb performance when doing ice survey operation. The investigation determined that both engines were operating at the time of the occurrence.
With the engine anti-ice system selected ON, climb performance would be compromised. This could be mitigated by use of the fuel dump system to reduce the weight of the aircraft. However, this would take some time depending on the amount of fuel to be dumped to lower the weight to 4850 pounds. Depending on altitude this may not be achievable in the time available. If an aircraft is operated outside the weight limit allowing a single-engine climb, as published by the manufacturer, then there is an increased risk that climb performance will not be achievable when unexpected conditions are encountered.
According to the BO 105 RFM, the engine anti-icing system must be ON when the ambient temperature is below +4 °C and visible moisture is present, except for takeoff and landing.Footnote 134 In this occurrence, the outside air temperature (OAT) was −1.4 °C, but nothing indicated the presence of visible moisture even though the graphic area forecast (GFA) indicated that local (25% or less of the area covered) visibilities could be reduced to 2 statute miles in snow and 1 statute mile in light freezing drizzle and mist in any onshore flows. Nothing in the SOC precludes ice probe operations in such weather conditions, except if there is a threat of whiteout conditions. Therefore, it is possible that the pilot selected the engine anti-icing system ON in case unexpected visible moisture was encountered. This way, the pilot would not have been distracted by the task of selecting it ON, while flying at low altitude.
The reason the pilot took off at a weight that was above the maximum gross weight stated in the SOC is unknown, but any of the following could have been a factor in that decision:
- The pilot found out that the master would be on board only after the aircraft had been refuelled the previous day.
- Since the pilot's last ice measurement mission with the ice-probe was carried out in 2010, the pilot may have forgotten about the weight limitation.
- There was no evidence that the pilot had undergone initial or recurrent training as per the SOC, which would have served as a reminder of all the limitations.
- There was no indication that the pilot had reviewed the SOC before the mission.
There was no ice service specialist on the vessel to carry out an ice reconnaissance flight; this would explain why the master decided to get on this flight. This type of aerial work is usually conducted at higher altitude in order to have a better view of the intended path to follow. The Canadian Coast Guard Ship (CCGS) Amundsen crew had access to daily ice charts and satellite image analyses of the Parry Channel and M'Clure Strait. However, ice charts and satellite imagery might not reflect what is actually experienced in a certain area at a specific time since ice movements are dynamic.
2.2.1 Ice probe installation
On the occurrence aircraft, the cables were routed along the right side, contrary to all of the supporting data for the supplemental type certificate (STC), which showed the cables to be routed along the left side of the helicopter. As a result, the cable bundle was routed above the right side static port and Pitot tube. This had caused erroneous airspeed readings during a previous flight, forcing the pilot to return earlier than planned to fix the problem. In this occurrence, the ice probe cable bundle was routed in a similar way, about 6 cm above the static port and secured in place by multiple layers of heavy grey tape instead of going through Adel clamps. Nothing indicates that the occurrence pilot experienced an erroneous airspeed reading, but it cannot be completely ruled out. Therefore, if operators deviate from an approved design/installation without considering the potential adverse consequences, then there is a risk that the change may jeopardize the safety of flight.
Neither the occurrence pilot nor the aircraft maintenance engineer (AME) who reinstalled the cables and the ice probe could have been aware of the previous occurrence since it was not recorded in the aircraft journey log or reported through ASD's safety management system (SMS). If hazards identified during flight operations are not reported or recorded, then there is an increased risk that mitigation measures will not be developed and implemented to prevent future re-occurrence.
There was no record made for the change in cable routing or the erroneous airspeed indications experienced during a previous flight. Additionally, ASD had no record of a modification proposal for the change in cable routing. If operators do not record work that has been carried out or discrepancies that have been noted during operation in the aircraft's technical records, then there is a risk that the overall condition of the aircraft will not be accurately known, which could jeopardize the safety of flight.
2.3 Visual cues in low level flight
As demonstrated in the review of the video and still images recovered from the wreckage, the availability of visual cues and light levels varied considerably during the flight. The aircraft crossed an area of open water estimated to be approximately 2.3 nm wide, based on the RADARSAT-2 imagery. This is larger than any of the other areas observed in the videos. Transitioning to flying over open water would have resulted in a sudden and significant reduction in visual cues available to judge height. This would have been particularly true in calm wind or if a skim coat of ice was present on the water.
The loss of references in the near visual field would have required the pilot to increase the scan of other available cues (distant visual field and instruments) in order to detect any change in altitude. Given the low altitude of the flight, this transition would have needed to be very quick, as a momentary loss of orientation could have resulted in contact with the surface. In addition, the dark overcast sky ahead would no longer have provided the distinct line of horizon against the water that would have been present when flying over the ice surface. Therefore, a pitch attitude change would have been difficult to recognize.
In this case, the helicopter levelled off at 36 feet at 1739:19, 3.71 minutes before impact. Considering an average speed of 67 knots up to the time of impact, the helicopter would have been approximately 4.1 nm from the impact point at that time. Since the open water area was approximately 2.3 nm wide and the helicopter crashed about 0.7 nm from the next ice edge, the helicopter was over the ice surface and approximately 2.5 nm from the open water when it levelled off at 36 feet. Using the same average speed, the helicopter would have reached the ice edge at approximately 1741:33 and then flown above the open water for approximately 89 seconds before impact. According to data from the onboard FFS, the descent leading to the impact lasted about 13 seconds, which indicates that the pilot maintained control for 76 seconds following the loss of references in the near visual field. The 13-second descent corresponds to an average rate of descent of about 166 feet per minute with a slight increase in speed. This is consistent with a shallow descent path, which would have been difficult to recognize in the absence of adequate visual cues. A lack of adequate visual reference as the aircraft was flying over an area of open water is consistent with the facts of the occurrence and cannot be ruled out. There is a strong probability that while over the open water, the pilot experienced a lack of the visual cues required to judge altitude, which led to controlled flight into terrain (CFIT).
2.4 Flight following system
The timely initiation of search and rescue (SAR) activities can greatly reduce the severity of the consequences following a survivable aircraft accident. In this occurrence, all 3 occupants initially survived the impact but, despite the proximity of the accident site to the vessel, they succumbed to the effects of cold water exposure before they were rescued.
FFSs are implemented as a means to minimize delays in initiating SAR efforts by monitoring the position and status of an aircraft in flight and providing the operators with timely information as soon as possible after a loss of contact or crash. The previous FFS used for shipboard operations was no longer viable and the implementation of a new FFS began in 2013. For the crew on the CCGS Amundsen, this was their first season using the new FFS to track the helicopter. For various reasons, the new FFS did not fulfill its objective of initiating timely SAR efforts the day of the occurrence. Therefore, this part of the analysis will focus on why this occurred.
2.4.1 Flight following system setup and monitoring
According to the Canadian Coast Guard (CCG) FFS standard operating procedures (SOPs) issued on 14 June 2013,Footnote 135 prior to commencing helicopter operations, the vessel crew must perform the following on the FFS control display unit (CDU):
- Change its position interval (PI) from 4 hours to 2 minutes to ensure that the vessel and the helicopter receive position information every 2 minutes.
- Select the appropriate helicopter from the rendezvous list and initiate the rendezvous.
The PI determines the frequency at which the vessel's position is sent to the server. When the rendezvous function is initiated, the helicopter position, bearing, distance, and overdue status are returned to the vessel and displayed on the FFS CDU. This information is updated after the vessel position is sent to the server, either manually or automatically. Position reports are sent to the server automatically based on the PI setting or manually via FFS CDU selections made by the user. If the server detects 3 missed helicopter position reports, it returns an overdue notification that is displayed on the FFS CDU by replacing the asset tag with dashes.
The last helicopter position on the server logs was at 1741; therefore, with the PI set at 2 minutes, the server would have returned an overdue notification after 1747. However, since the helicopter PI was set to 1 minute that day, the server would have returned the overdue notification after 1744. Therefore, any vessel position report sent to the server (automatically or manually) after 1744 would have resulted in the vessel receiving an overdue notification. This would have been indicated on the vessel's FFS CDU by replacing the asset tag (CCG364) by dashes on the CDU, if the rendezvous function had been active.
The vessel crew was not familiar with the new FFS CDU and had difficulties using it. For example, during previous helicopter operations, the PI remained at 2 minutes for 3 days before it was changed again to 4 hours. On the day of the occurrence, the PI on the vessel's CDU was not changed from 4 hours to 2 minutes. Since the last automatic vessel position was sent at 1617, the overdue notification would not have been received automatically until 2023, 2 hours and 40 minutes after the crash. The only vessel positions sent to the server were manual position reports as a result of user manipulations on the CDU that were made at 1755, 1805, and 1826.
At 1805, 17 minutes after the helicopter's ETA and 22 minutes after the helicopter crashed, the wheelhouse crew checked the position of the helicopter on the vessel's CDU, which displayed the helicopter's distance at 3.2 nm. This information led the crew to believe that, although the helicopter was late, it would arrive in approximately 3 minutes. The crew did not realize that the helicopter position displayed on the CDU was time stamped at 1741, which meant that it was 24 minutes old.
At 1826, while the vessel was en route to the last known position (LKP), a crewmember questioned the time of this position. It was only then that the crew noticed the time stamp and realized that the helicopter position displayed on the CDU was 45 minutes old. According to the Web server logs, it was determined that the asset tag (CCG364) had been replaced by dashes at 1755.
The FFS SOPs do not specify who monitors the vessel's CDU for an overdue notification or at what frequency it is monitored. To notice the overdue notification in a timely manner, a designated crew member would have to monitor the vessel's CDU continuously to observe the replacement of the asset tag (CCG364) with dashes. This was not practical in the context of the operational demands in the wheelhouse on the day of the accident, especially given its physical location on the bridge. If SOPs do not provide specific guidance as to who is to perform specific tasks, such as monitoring an FFS, then there is an increased risk that time-critical tasks will not be performed as intended.
One of the assumptions implicit in the statement of requirements (SOR) is that the FFS CDU would be monitored by the vessel's crew. Consultations between the groups responsible for system development and end users did not challenge this assumption. As a result, the SOR did not contain a requirement for an aural alarm to accompany the emergency or overdue messages generated by the system. The decision to rely solely on discrete visual indications in these circumstances was based on this assumption; no human factors design guidelines or standards were used to determine whether an aural alarm was warranted.
2.4.2 Aural warnings
The previous FFS generated an aural warning when the signal to the helicopter was lost. The crew was familiar with these warnings and relied on them during busier shipboard operations. The new FFS did not provide aural warnings, as they were not part of the design requirements. Given the vessel crew's level of multi-tasking and workload during scientific operations, their attention was most likely focussed on the primary tasks related to shipboard operations. It is possible that during this time, the wheelhouse crew expected that, if the helicopter signal was lost, an FFS aural warning would have been generated.Footnote 136
Had the crew been alerted immediately of the overdue status of the helicopter, which was available on the server after 1744, occupants could have been rescued at approximately 1813, instead of 1854. This is assuming the same 6 minutes for the communications search before initiating the SAR measures, plus 23 minutes for the vessel to reach the debris field. There was no aural warning to alert the vessel's crew immediately that a helicopter was no longer transmitting position reports or had crashed. Therefore, the initiation of SAR efforts was delayed. It was not possible to determine the impact of this delay on the survival of the occupants because even if they had been rescued at 1813, they would have been in the water for approximately 30 minutes before they were rescued.
2.4.3 Flight following system training
The SOR for the FFS specified that the system should not require extensive training to be operated. The approach to training the vessel's officers in the use of the system consisted of a webinar briefing and training material provided to the vessel's technicians who would then brief the vessel's wheelhouse crew.
The training materials and procedures described the need to adjust the PI during helicopter operations. However, the role of the PI for overdue notifications, the importance of the time stamp, and the workings and display of the overdue notification were not fully understood by the vessel's crew.
Therefore, despite attempts by the crew to set up the FFS as per the SOPs, the PI was not set correctly for helicopter operations; this explains why the vessel's crew could not receive the helicopter's position information 17 minutes after takeoff. When the CDU position information was eventually displayed, it was interpreted as current and the crew did not initially determine from the CDU that the helicopter was overdue.
Therefore, the training did not bring the vessel's crew to the required level of competence to set up the FFS and later interpret the information displayed on the CDU. This reduced the effectiveness of the FFS and delayed the initiation of the SAR efforts.
2.4.4 Control display unit position
When the SAR effort was initiated, the crew proceeded to the position displayed on the FFS CDU. Since this position is presented with a dot placed between the minutes and the seconds, the crew read the position as degrees, minutes and decimal minutes. In reality, the position displayed on the CDU is meant to be degrees, minutes and seconds, resulting in the crew proceeding to an incorrect LKP.
The position error in this case was 743 m and did not affect the SAR efforts, as the floating debris and occupants were located visually before the vessel arrived at the target coordinates. However, in different circumstances, the SAR efforts could have been hindered by this position error. Therefore, it is essential that the FFS CDU display asset position information to the crews in a format that is normally expected for latitude and longitude.
Human factor design standards were not specifically defined in the requirements. If systems are developed without the benefit of appropriate end-user input and the use of relevant human factors design standards, then there is an increased risk that display systems will not be suited for their end purpose and that users will not use them correctly.
2.5 Survivability
2.5.1 General
Helicopter crash survivability on land is usually dependent on tolerable deceleration forces, an uncompromised occupant space, and the absence of post-crash fire. A water impact adds a significantly different dimension to occupant survivability—the possibility of rapid submersion. In this occurrence, all 3 occupants survived the impact, but succumbed to the effects of cold water exposure and drowned before they were rescued.
In this occurrence, the occupants were immediately exposed to cold shock as the helicopter sank in the −0.6 °C water. It has not been determined if the individuals managed to unbuckle their seat belts by themselves or if they were helped by one of the other occupants. Considering that neither the master nor the scientist had taken helicopter underwater egress training (HUET), it is possible that it was more difficult for them to exit the helicopter than it would have been for the pilot, who had taken HUET in the past. Therefore, it is possible that the pilot managed to escape more rapidly and inflate the PFD before being incapacitated.
At the time of the occurrence, it had been almost 2 years since the pilot had taken HUET. Although an optimal interval for recurrent HUET training has not been established, studies have demonstrated significant skill decay in as little as 6 months post training. Therefore, if crews are not provided with any additional training to mitigate procedural skill decay occurring in the 3 years between recurrent HUET sessions, then there is an increased risk that they will not be able to combat the serious hazards associated with ditching.
Even with the protection of an immersion suit, the sudden exposure to the cold water causes a gasp reflex and hyperventilation, which can lead to involuntary water intake. The occupants would have had little time to evacuate, since in near-freezing water, breath-holding time drops dramatically to about 10 to 15 seconds.Footnote 137 Further, in 0 °C water, complete incapacitation can be expected within 10 to 20 minutes, making it impossible for victims to maintain their airway above the water line without adequate flotation.
2.5.2 Personal flotation device
In March 2013, ASD's Chief, Maintenance Quality Assurance, was advised by one of ASD's base personnel that an improperly folded life vest had been found, and that the vest overhaul manual did not contain a referenced drawing that illustrated the instructions for folding the life vest. In response, the ASD updated its manual.Footnote 138
Following the occurrence, on 2 occasions, in September 2013 and in March 2014, ASD identified additional incorrectly folded PFDs and in response, fleet-wide inspection campaigns were carried out by issuing Campaign Notice 010-25-60-027 and the revised Campaign Notice 010-25-60-027 Rev A. The 4 spare PFDs on board the helicopter at the time of the occurrence were found to be incorrectly folded. Given that the 3 occupants' PFDs had been overhauled at the same time in July 2013, it is likely that they were all packed the same way. This is supported by the similarity in the manner the master's PFD inflated when the TSB tested it and compared it with tests conducted in a swimming pool.
When the first improperly packed PFD was reported to Maintenance Quality Assurance in March 2013, the corrective actions taken were limited to the maintenance base where the issue had been reported. System-wide corrective actions were not taken until the identification of additional improperly packed PFDs in September 2013. Despite the issuance of Campaign Notice 010-25-60-027 on 25 September 2013, 7 other improperly folded PFDs were found in March 2014. A revised campaign notice was issued on 15 May 2014. If identified hazards are not fully investigated through quality assurance programs to determine the extent of their seriousness, then there is a risk that mitigation measures will not fully eliminate all instances of the hazard.
Although the investigation confirmed that the pilot was wearing a PFD on departure, the pilot was not wearing it when recovered from the water; it was found floating nearby, completely inflated. Based on the suit and life vest examination, it is unlikely that a zipped PFD detached from the pilot's suit during the accident sequence. It is therefore most likely that the pilot removed the PFD after exiting the aircraft, possibly for one or more of the following reasons:
- to zip up the immersion suit to prevent further water ingress;
- to dive in order to help one or both of the other occupants unbuckle their seat belts;
- to dive to get the life raft; or
- to reduce pressure felt on the neck and/or rib cage caused by the inflated life vest.
The master was found with a PFD on, but not inflated. Post-occurrence testing confirmed that the PFD worn by the master inflated when both lanyards were pulled. Therefore, it is probable that the master was unable to activate the PFD before being incapacitated by the effects of cold water immersion.
The scientist was recovered wearing a partially inflated PFD; only the left side was inflated. When the TSB examined the vest, it was noted that both cylinders had been activated. It could not be clearly demonstrated if an improperly packed PFD would have caused the partial inflation of the scientist's PFD considering that the pilot's PFD, which was likely improperly packed, inflated completely. However, if PFDs are improperly packed, then there is a possibility that they will not inflate as designed when only 1 cartridge is activated, thereby increasing the risk that the user's mouth and nose will not be held clear of the water line and increasing the risk of drowning.
In this occurrence, none of the 3 occupants was supported in a manner to keep their mouth and nose above the water line. It is likely that they drowned as a result of cold incapacitation.
2.5.3 Personal locator beacons
All of the occupants' PFDs were equipped with a waterproof personal locator beacon (PLB) stored in the right side pocket. The PLB is designed to be manually deployed and activated. However, the process to deploy and activate the PLB requires fine tactility that could be difficult to achieve with the use of the 3-fingered lobster-claw-style gloves. Therefore, the user would have to complete the PLB activation without wearing the gloves, which would extend the period of time that their hands and fingers would be exposed to the cold. Furthermore, to ensure proper operation, the antenna needs to be unobstructed with a clear view of the sky and kept dry and away from the water. It could be difficult for users to hold the PLB out of the water if they are in the water for a long period of time before being rescued.
In this occurrence, none of the PLBs had been deployed or activated. This could be explained by the following:
- the occupants had lost consciousness shortly after the crash; or
- the PLB could not be deployed or activated due to the cold water exposure of the occupants' hands since none of them were wearing gloves.
If occupants face cold water exposure of their hands, then it could be difficult to use personal emergency equipment requiring fine tactility, thereby increasing the risk of not being able to use it and not being located in a timely manner.
2.5.4 Cold water immersion
It is highly unlikely that the victims' immersion time was long enough to induce severe hypothermia and cold-induced ventricular fibrillation. However, the victims were definitely immersed long enough to cause considerable, if not complete, cold incapacitation which would have made it impossible for them to maintain their airway above the water line while not wearing a PFD, or while wearing one that was improperly inflated.
Based on the sea temperature (−0.6 °C) and conditions (calm), as well as the clothing worn, the core temperature of all victims was predicted to be no lower than 34 °C when recovered; this is considerably higher than the core temperature at which hypothermia would cause ventricular fibrillation (generally <28 °C); therefore, hypothermia per se was not a primary cause of death.
It is likely that the occupants were completely submerged during impact and egress since it is probable that the helicopter sank quickly. Complete submersion in ice water would initiate the gasp reflex and decrease breath-holding ability; thus, drowning could have occurred as early as during egress. This may explain why none of the master's PFD's cartridges had been activated.
If the drowning did not occur during egress, the question of how the occupants could have been incapacitated enough to drown is an important one, as the predictions indicate that the core temperature of the 3 occupants would not have been lower than 34 °C. Although there are no standards in Canada for pilot suit insulation criteria, the pilot's suit clo value was above the standards established by the European Technical Standard Orders ETSO-2C502 and ETSO-2C503. The pilot's incapacitation could be explained by the fact that the insulation value of the thermal liner is virtually eliminated when the suit is flooded. Furthermore, the limited buoyancy of the pilot suit likely required more effort and movement to maintain the airway above the water line, particularly since at one point the pilot was not wearing a PFD. Consequently, this activity would increase heat loss, especially with a suit full of ice-cold water. Although the helmet itself provides some buoyancy, the pilot drowned at some point because the airway was not maintained above the water line and the pilot did not have the energy and strength to keep the airway continuously above the water line.
Neither the master nor the scientist was wearing any head insulation; if they had been, it may have reduced the core cooling rate to some extent when the back of the head was immersed in cold water. Furthermore, they both wore suits designed with reduced buoyancy, which would have contributed to their core cooling rate being faster than predicted due to the increased effort required to keep their airway above the water line because their PFDs were not properly inflated. The low insulation values of the suits worn by the 3 occupants, combined with mild hypothermia and significant cold incapacitation, likely contributed to their inability to keep their airways above the water on their own, and led to their drowning.
Cold water can delay the effect of oxygen deprivation on the brain. Cold-water-immersion survival times have typically ranged from 10 to 30 minutes, with the length of time being dependent on the extent of brain cooling. The extent of brain cooling could not be determined for this occurrence. However, because neither their bodies nor their airways were completely or continuously submerged beneath the water surface, brain cooling would have been less extensive than what is normally seen in cold-water drowning.
Table 8 provides the best-case scenario based on this occurrence and taking into account the expected times of cold incapacitation and cold water protection presented above. Using the latest expected time of complete incapacitation due to cold water immersion, the time of drowning was likely 20 minutes after the occurrence; however, it is possible—although far from certain—that the victims may have survived up to 50 minutes post-accident. The victims were recovered from the water 73 and 92 minutes after the accident, which is significantly beyond this window of possible survival.
| Lapsed time (minutes) | Event timeline |
|---|---|
| 90 | Third victim recovered |
| 80 | Most extreme example of noted cold-water survival (66 minutes after drowning; 86 minutes after the accident) |
| 70 | First 2 victims recovered (73 minutes after the accident) |
| 60 | |
| 50 | Period of likely protection due to brain cooling (10–30 minutes after drowning; 30–50 minutes after the accident) |
| 40 | |
| 30 | |
| 20 | Conservative estimate of time to complete incapacitation (20 minutes). Latest time of likely drowning. |
| 10 | |
| 0 | Accident |
2.5.5 Emergency locator transmitters
If an aircraft crashes over land, an emergency locator transmitter (ELT) that survives the crash will normally transmit at full strength after the required 50-second delay. However, when an aircraft crashes in water, there is a strong possibility that a fixed ELT antenna will end up below the surface of the water before the 50-second delay has elapsed. If that is the case, it is possible that the ELT signal will be greatly attenuated and will not be detected by the COSPAS-SARSAT satellite system. If an ELT fails to transmit at full strength from a submerged aircraft, then rescue may be significantly delayed, increasing the risk of serious injury or death.
2.5.6 Life raft
The life raft was installed inside the helicopter and sank with the aircraft; therefore, it was not available to aid the survivors after the accident. Without a life raft, the 3 occupants' only option was to stay in the water until being rescued. Life rafts attached inside the helicopter may be appropriate in the event of a successful controlled ditching, but they do not ensure protection during an unexpected crash into water.
2.5.7 Immersion suits
The Operations Manual, Canadian Coast Guard Helicopters requirements for immersion suit use are more stringent than those in the Canadian Aviation Regulations (CARs); however, the criteria for distance from shore, vessel, or continuous ice capable of supporting the helicopter are inadequate to ensure proper protection. Survivors may be injured or suffering from cold shock, which can severely limit mobility. The immediate concern for survivors who are immersed in frigid water is to survive long enough to inflate and get into the life raft, or to stay alive in an immersion suit until help arrives. Even when helicopter operations occur near shore, vessel, or continuous ice capable of supporting the helicopter, pilots and passengers can be exposed to periods of operations over sometimes frigid water without appropriate protection, since life raft requirements are based on time and distance criteria.
Significant risk arising from cold water immersion usually begins in water colder than 25 °C. That being the case, the risk of immersion hypothermia exists throughout most of the year in North America. However, managing the risk of heat exhaustion, dehydration, and fatigue from wearing a flight crew immersion suit is a competing goal that must be considered when determining the most appropriate protective equipment. If flight crews and passengers do not wear suitable immersion suits when flying over cold water, then there is a greater risk that they may experience hypothermia once in the water.
In this occurrence, all occupants were wearing anti-exposure suits even though neither the CARs nor CCG and ASD policies required it. However, the passenger transportation suit systems (PTSS) provided to the master and the scientist did not meet the requirements contained in CARs Standard 551.407; their suits had an insulation value of 0.4 clo in still water, while the CAN/CGSB-65.17-99 standard indicates that the PTSS must provide thermal protection of at least 0.75 clo. Furthermore, the master was found completely face down, while the scientist's face was half submerged. This indicates that their suits did not meet the righting performance requirement contained in CAN/CGBS-65.17-99, which states, “the suit system shall turn the wearer from a face-down position to a face-up position within 5 [seconds] or allow the wearer without assistance to turn himself or herself from a face-down position to a face-up position within 5 [seconds].” If the PTSS worn does not meet standard requirements, then there is an increased risk that the wearer will be exposed to the onset of hypothermia more quickly during cold water immersion and might not be adequately protected from drowning.
Furthermore, it is common practice for pilots not to zip their suit all the way up. This practice is supported by TC's memo issued in May 2011, which implies that the suit may be partially unzipped during some flight conditions. However, these conditions are not defined. If guidance pertaining to the proper usage and wearing of immersion suits is not clear, then pilots may not wear immersion suits in a way that ensures maximum protection when required.
In order to achieve maximum protection, it is of critical importance that an immersion suit be fully zipped up and closed to the top of the neck seal prior to entering the water. However, zipping up the suit during flight in an emergency situation would be virtually impossible. It is extremely unlikely that a pilot who is wearing a helmet and seated in the helicopter with the life vest attached and the safety harness done up during flight would be able to completely do up the zipper from the mid-sternum position, even in the case of a planned ditching. The helmet and seat back would limit the pilot's ability to bend their head back and to the right; access to the zipper would be limited due to the life vest and the seat belt assembly; and the pilot would need both hands to fly the aircraft.
2.5.8 First aid and medical services
Once on board the vessel, the 3 victims were brought to the hangar. Since the 3 victims had experienced cold water immersion, it was initially planned to treat them for hypothermia. The main vital signs were checked, except for body core temperature. They all showed signs of drowning, and the cause of death was most likely from exposure to cold water. There is no indication that further CPR efforts on the 3 victims or attempts to warm them up as specified in the International Medical Guide for Ships could have prevented their deaths. Considering the amount of experience the health officer had, it is reasonable to believe that the declaration of death for the 3 victims was well-founded.
However, in case of hypothermia, the International Medical Guide for Ships indicates that people suffering from hypothermia may appear dead even though they are still alive and it can be very difficult to take their pulse due to the fact that the heart rate may be extremely slow and shallow. That is why taking the body temperature is a key vital sign to be measured. A checklist detailing the steps for treating people suffering from cold water immersion posted and available would likely assist people providing first aid treatment to ensure that all steps are followed.
Vital signs determine which treatment protocols to follow, provide critical information needed to make life-saving decisions, and confirm feedback on treatments performed. Therefore, if vital signs are not all considered or measured during the preliminary assessment of a patient once recovered, then there is an increased risk that critical information needed to save their life will be missed or that inappropriate treatment protocols will be followed.
2.6 Organizational and management information
2.6.1 Regulatory oversight
Transport Canada has moved toward a systems approach to surveillance. For operators who are not required to have an SMS, this is intended to ensure sufficient processes are in place to provide for operational control and compliance with regulations. Further, follow-up procedures are in place which, when followed, should provide the regulator with timely proof that operators have fully analyzed the underlying causes of findings and put corrective actions in place to address them and prevent recurrence.
Transport Canada Civil Aviation identified critical and major findings related to operational control 2 years prior to the occurrence flight. Although TCCA worked with ASD to ensure adequate corrective action plans (CAP) were developed and implemented, progress was slow. It took 6 months before a revised set of CAPs was found acceptable by TCCA and at the time of the occurrence, 18 months later, TCCA had not yet been provided sufficient assurance that the CAPs had been successfully implemented.
There were a number of issues that contributed to the extended time taken to close the 2011 program validation inspection (PVI). First, the move toward a systems approach to oversight meant that both TCCA and ASD were on a significant learning curve. During the time the 2011 PVI was open, documentation provided to TCCA inspectors was substantially updated with additional guidance material, including additional worksheets to provide greater understanding of expectations when validating specific systems. Similarly, this was the first surveillance activity where ASD was expected to provide a systems level analysis of the underlying issues to support its planned corrective action. The rejection of the first set of CAPs was largely due to a lack of underlying analysis; TCCA saw an improvement in the scope of the analysis provided in the revised CAPs.
Second, some of the findings included in the 2011 PVI were broadly stated and non-specific. This included the critical finding related to operational control, which simply stated that 2 separate incidents involving CCG helicopters were indicative of a loss of operational control. The finding used outcome measures to point to a weak operational control system in general, rather than identifying weaknesses in one or more aspects of the operational control system. In a mature SMS, the operator should be able to use its internal investigation to identify the underlying causes of the incidents and corrective actions taken. If findings are overly general, it increases the scope of possible corrective actions and makes it more difficult for the regulator to assess whether the underlying deficiency is addressed through the corrective action plan, increasing the risk that safety deficiencies will remain unaddressed.
Third, and likely related to the general nature of some of the findings, is that the corrective actions proposed by ASD were extremely broad in scope. Revising the Company Operations Manual (COM), implementing a flight operations quality assurance program, and reviewing all shipboard procedures were long-term initiatives that could not be reasonably expected to be accomplished in the 90-day timeframe in which most corrective actions were expected to be implemented—or even in the 6-month timeframe in which all corrective action were expected to be completed. However, the expansive corrective actions proposed by ASD were accepted by TCCA.
Finally, TCCA elected to work with the operator to encourage the implementation of the corrective action plans, rather than pursuing certificate action. A lack of progress in implementing the CAPs was identified by TCCA inspectors in June 2012 and a meeting was held between TCCA and ASD to discuss requirements. Revised timeframes were agreed upon and by the end of September 2012, a revised COM was submitted, while the implementation of flight operations quality assurance and the review of shipboard operations were still outstanding. Although progress continued to be monitored within TCCA, more than a year had passed since ASD had been informed that its operational control system did not conform to minimum regulatory requirements. Continuing to work with the operator in the face of repeated delays in CAP implementation, permitted this situation to continue. If Transport Canada does not take action to require operators to respect CAP implementation timeframes, there is a risk that safety deficiencies will not be corrected in a timely manner.
The extended time allowed to implement corrective action had an additional impact on TCCA's ability to ensure that ASD had the processes in place to operate safely, since TCCA elected to postpone any additional PVIs until the CAPs had been effectively implemented. The rationale behind this decision was that additional surveillance, conducted before corrective action could be effectively implemented, would identify the same deficiencies and not represent an effective use of resources. However, it created a situation where an operator, identified as necessitating annual system-level oversight and which had previously been found to have had critical deficiencies in operational control, was actually receiving less frequent regulatory oversight than TCCA directives dictated as a result of a lack of progress in implementing corrective actions. Therefore, TC was not providing an effective oversight of ASD as a company transitioning to SMS.
Following the accident, TCCA identified deficiencies in the communication of procedures and training related to the ice probe operation, of which TCCA was previously unaware. While it cannot be stated with any certainty that further system-level surveillance would have identified these deficiencies prior to the accident, the absence of such surveillance certainly reduces the regulator's effectiveness in proactively identifying practices that could lead to safety deficiencies. If identified regulatory surveillance intervals are not respected, then there is an increased likelihood that systemic deficiencies that could increase risk will go unidentified and unaddressed.
2.7 Wreckage search
Locating underwater aircraft wreckage expeditiously is important for humane reasons and is essential for investigative purposes. Examination of aircraft wreckage is a fundamental part of an accident investigation and is particularly important in those accidents where a recorder has not been installed on the aircraft and/or the occupants do not survive. An underwater locating device, installed and operating as designed, would likely have led to the wreckage being located more quickly.
Fortunately, the CCGS Amundsen was fitted with a voyage data recorder (VDR), even though it was not required to be by regulation. The saved data provided valuable information to the investigation and allowed investigators to determine the time of impact, which, combined with the SkyWeb last known position and track, helped to locate the wreckage and recover it for examination.
3.0 Findings
3.1 Findings as to causes and contributing factors
- There is a strong probability that while over the open water, the pilot experienced a lack of the visual cues required to judge altitude.
- The possibility of pilot distraction could have caused a lapse in the pilot's concentration, resulting in the loss of altitude and water contact.
- None of the 3 occupants was supported in a manner to keep their mouth and nose above the water line. It is likely that they drowned as a result of cold incapacitation before they were rescued.
- The life raft was installed inside the helicopter and sank with the aircraft; therefore, it was not available to aid the survivors after the accident.
- The training did not bring the vessel's crew to the required level of competence to set up the flight following system and later interpret the information displayed on the control display unit. This reduced the effectiveness of the flight following system and delayed the initiation of the search and rescue.
- There was no aural warning to alert the vessel's crew immediately that the helicopter was no longer transmitting position reports. Therefore, the initiation of search and rescue was delayed.
3.2 Findings as to risk
- If cockpit or data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
- If an aircraft is operated outside the weight limit allowing single-engine climb, as published by the manufacturer, then there is an increased risk that climb performance will not be achievable when unexpected conditions are encountered.
- If operators deviate from an approved design/installation without considering the potential adverse consequence, then there is a risk that the change may jeopardize the safety of flight.
- If hazards identified during flight operations are not reported or recorded, then there is an increased risk that mitigation measures will not be developed and implemented to prevent future re-occurrence.
- If operators do not record work that has been carried out or discrepancies that have been noted during operation in the aircraft's technical records, then there is a risk that the overall condition of the aircraft will not be accurately known, which could jeopardize the safety of flight.
- If standard operating procedures do not provide specific guidance as to who is to perform specific tasks, such as monitoring a flight following system, then there is an increased risk that time-critical tasks will not be performed as intended.
- If systems are developed without the benefit of appropriate end user input and the use of relevant human factors design standards, then there is an increased risk that display systems will not be suited for their end purpose and that users will not use them correctly.
- If crews are not provided with any additional training to mitigate procedural skill decay occurring in the 3 years between recurrent helicopter underwater egress training sessions, then there is an increased risk that they will not be able to combat the serious hazards associated with ditching.
- If identified hazards are not fully investigated through quality assurance programs to determine the extent of their seriousness, then there is a risk that mitigation measures will not fully eliminate all instances of the hazard.
- If personal flotation devices are improperly packed, then there is a possibility that they will not inflate as designed when only 1 cartridge is activated, thereby increasing the risk that the user's mouth and nose will not be held clear of the water line and increasing the risk of drowning.
- If occupants face cold water exposure of their hands, then it could be difficult to use personal emergency equipment requiring fine tactility, thereby increasing the risk of not being able to use it and not being located in a timely manner.
- If an emergency locator transmitter fails to transmit at full strength from a submerged aircraft, then rescue may be significantly delayed, increasing the risk of serious injury or death.
- If flight crews and passengers do not wear suitable immersion suits when flying over cold water, then there is a greater risk that they may experience hypothermia once in the water.
- If the passenger transportation suit system worn does not meet standard requirements, then there is an increased risk that the wearer will be exposed to the onset of hypothermia more quickly during cold water immersion and might not be adequately protected from drowning.
- If guidance pertaining to the proper usage and wearing of immersion suits is not clear, then pilots may not wear immersion suits in a way that ensures maximum protection when required.
- If vital signs are not all considered or measured during the preliminary assessment of a patient once recovered, then there is an increased risk that critical information needed to save their life will be missed or that inappropriate treatment protocols will be followed.
- If identified regulatory surveillance intervals are not respected, then there is an increased likelihood that systemic deficiencies that could increase risk will go unidentified and unaddressed.
- If findings are overly general, it increases the scope of possible corrective actions and makes it more difficult for the regulator to assess whether the underlying deficiency is addressed through the corrective action plan increasing the risk that safety deficiencies will remain unaddressed,
- If Transport Canada does not take action to require operators to respect corrective action plan implementation timeframes, there is a risk that safety deficiencies will not be corrected in a timely manner.
3.3 Other findings
- The Canadian Coast Guard Ship Amundsen was fitted with a voyage data recorder, even though it was not required to be by regulation. The saved data provided valuable information to the investigation and allowed investigators to determine the time of impact, which, combined with the SkyWeb last known position and track, helped to locate the wreckage and recover it for examination.
- The underwater locator beacon did not transmit a detectable acoustic signal. An underwater locating device, installed and operating, would likely have led to the wreckage being located more quickly.
- Life rafts attached inside the helicopter may be appropriate in the event of a successful controlled ditching, but they do not ensure protection during an unexpected crash into water.
4.0 Safety action
4.1 Safety action taken
4.1.1 Aircraft Services Directorate
On 01 November 2013, the Aircraft Services Directorate (ASD) issued Pilot Information File (PIF) RW 2013-08-HQ to all Canadian Coast Guard (CCG) helicopter pilots to remind them of the hazards, and the ASD Company Operations Manual directions related to low-level flight operations. A minimum operating altitude of 200 feet agl was established for all flights, except when landing or taking off or during external load sling operations. In addition, ice probe operations were suspended and all similar work was identified as aerial work. The minimum operating altitude for aerial work operations was raised to 300 feet agl in March 2015 following the issuing of a new edition of the Operations Manual Helicopters. If it is identified that as part of a specific planned operation that it is necessary to fly lower than 300 feet agl, the Regional Supervisory Helicopter Pilot, the Chief Pilot, and the Director, Flight Operations shall be notified and a risk assessment shall be completed prior to the commencement of that task. Those flights should not be contemplated unless the risk assessment supports the activities and the Regional Supervisory Helicopter Pilot, the Chief Pilot, and the Director, Flight Operations support the activities in question.
On 25 February 2014, ASD issued PIF-RW 2014-09-HQ to all CCG helicopter pilots, including an excerpt from the CCG Helicopter Operations Manual related to shipboard operations. According to the PIF, all pilots were to meet with the master and first officer to review the shipboard operating procedures as described in the CCG Helicopter Operations Manual upon commencing their next deployment to shipboard duties.
On 15 May 2014, ASD issued a second campaign notice (010-25-60-027 Rev A) to clarify the procedure for folding Switlik life preservers and to check all life vests at the first opportunity to ensure they were folded correctly. A video demonstrating the proper folding technique was produced and is available to personnel responsible for inspecting and folding life vests.
On 16 September 2014, a team of ASD and CCG personnel completed a review of the 2008 risk assessment related to immersion suits for the rotary wing operations to verify the assumptions and update the document to ensure it remained valid. The recommendations from that risk assessment have resulted in a policy change proposal that will increase the frequency for wearing immersion suits in operations over water. The risk assessment team also recommended an immersion suit trial program to identify better options for flight crew, given advancements in suit technology since the previous procurement of the Viking 4089 in 2011. Following the immersion suit trial, new suits (Survitec 1000-300 or Viking 4043) were provided to flight crew identified in the urgent replacement category.
On 01 April 2015, ASD started to acquire a new fleet of helicopters to replace the BO 105. The new fleet is equipped with automatic float deployment and life rafts that are externally mounted and integral to the flotation system. These new helicopters also have enhanced one-engine-inoperative performance.
The new helicopters are equipped with state of the art CVFDR data acquisition flight recorders (cockpit voice recorders and flight data recorders). As well, the new helicopters are equipped with a health and usage monitoring system which can identify premature failures proactively.
A new immersion suit—wearing policy was implemented in April 2015, which significantly increased the requirement to wear suits and the procurement of a new type of immersion suit has begun.
The evaluation and selection of emergency breathing apparatus are completed and the procurement will begin in October 2015.
New and improved life jackets were obtained for the new helicopter fleet.
New personal locator beacons with simpler activation system were obtained for the new helicopter fleet.
An Operations Quality Assurance and Control system was implemented as of 01 April 2014.
Corrective actions related to PVI and PI were accepted by TCCA in July 2014 and implemented as per the corrective action plans.
4.1.2 Canadian Coast Guard
On 11 October 2013, the CCG instructed all personnel involved in shipboard operations to ensure that all vessels engaged in helicopter operations activate the rendezvous feature on the FFS and that the vessel's reporting rate has been switched to 2 minutes while the helicopter is in flight. Further to this, the vessel's crew is to verify the helicopter's position every 5 minutes using the FFS CDU and record the bearing and distance from the ship in the helicopter log. If the helicopter's call sign is replaced with dashed lines on the FFS CDU, the vessel's crew is to use voice communications to confirm the helicopter's position.
On 20 December 2013, the CCG issued an Operations Circular (OC 10-2013) regarding the discrepancy in the display of GPS coordinates on the FFS in order to inform CCG Fleet personnel of the possible misinterpretation of the GPS coordinates. This circular was created to inform ships fitted with an FFS that the display of GPS coordinates associated with tracking of a helicopter can be easily misinterpreted by the user community and that it is important that the user community understand how the information is currently displayed since incorrect reading of the display will result in the user incorrectly tracking a helicopter.
CCG implemented an on-site familiarization safety briefing in addition to the video briefing already in place for all Central and Arctic operational units.
In July 2014, prior to Arctic operations, CCG implemented a revised Helicopter Immersion Suit Policy for Arctic Operation. According to the policy, all passengers aboard CCG helicopters are to wear a CCG-authorized “dry-type” immersion suit with appropriate thermal protection.
During the 2014 Arctic operations, an evaluation of immersion suits was conducted in the field. The immersion suit policy was promulgated in December 2014 and fully implemented by 01 April 2015. The policy states:
All persons aboard CCG helicopters and all CCG personnel aboard non-CCG helicopters chartered for CCG operations shall wear a “dry-type” immersion suit with appropriate thermal protection underneath that is authorized by CCG, where the helicopter:
- is expected to fly over water, and:
- the water temperature is 13 °C or below, or
- the sum of air and water temperature is less than 31 °C.
In addition, an operations safety bulletin (OSB 06-2015) outlining roles and responsibilities with respect to the suit policy and application has also been issued. This bulletin was created to clarify the roles and responsibilities regarding the application of the Operations Circular 07-2015 – CCG Operations – Helicopter Immersion Suit Policy for all personnel who will be a passenger aboard any CCG helicopter, or a helicopter chartered for CCG Operations.
This report concludes the Transportation Safety Board's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – GFA clouds and weather charts
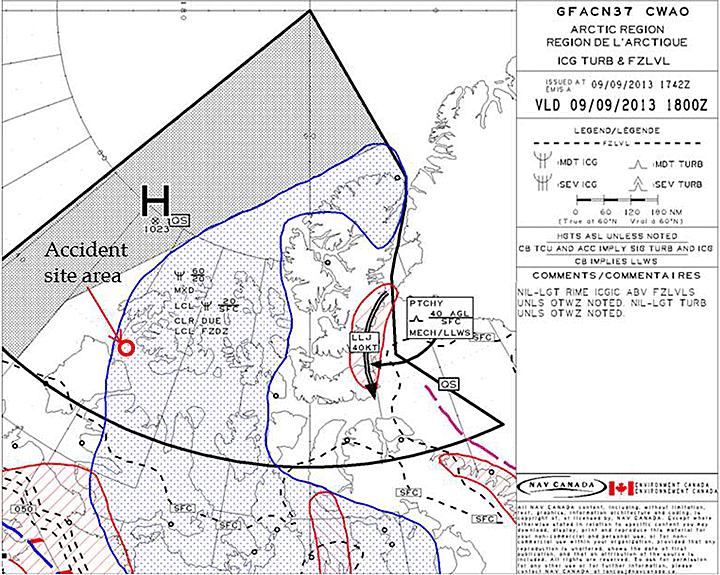
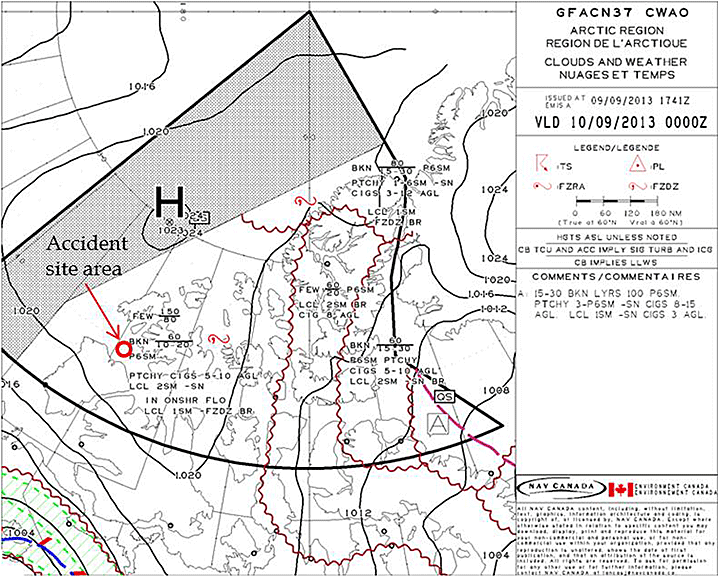
Source: NAV CANADA and Environment Canada, with TSB annotations
Appendix B – GFA icing, turbulence and freezing level
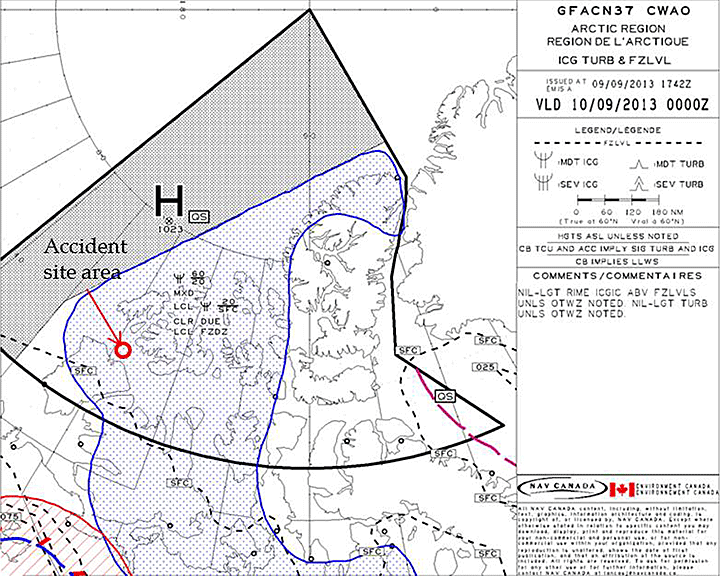
Source: NAV CANADA and Environment Canada, with TSB annotations
Appendix C – Ice daily chart valid at 1800Z on 09 September 2013
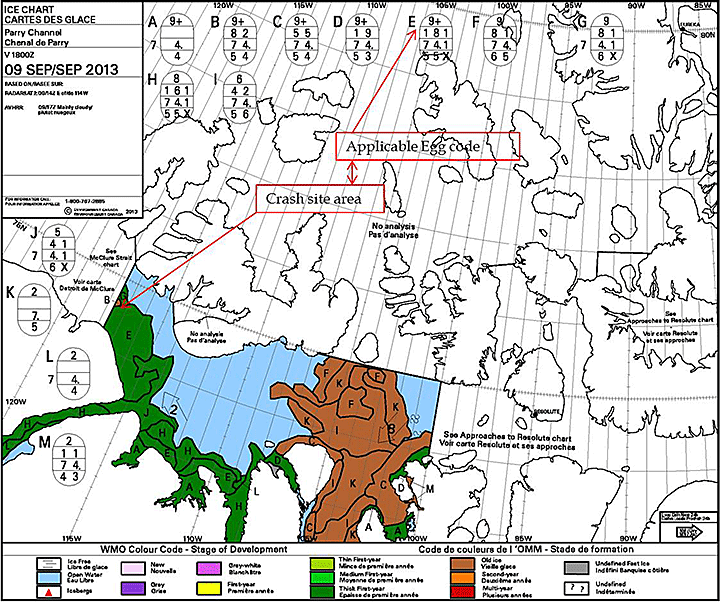
Source: Environment Canada, Canadian Ice Service, with TSB annotations
Appendix D – Specialty operations catalogue
Source: Transport Canada, Aircraft Services Directorate
Appendix E – Risk analysis matrix
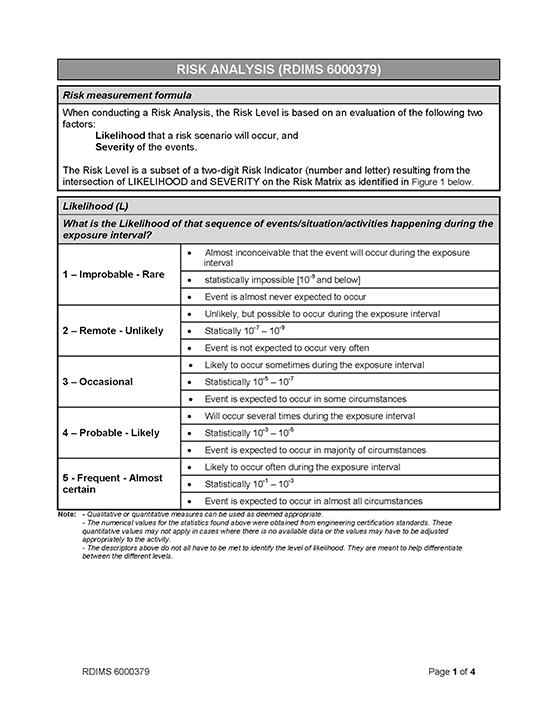
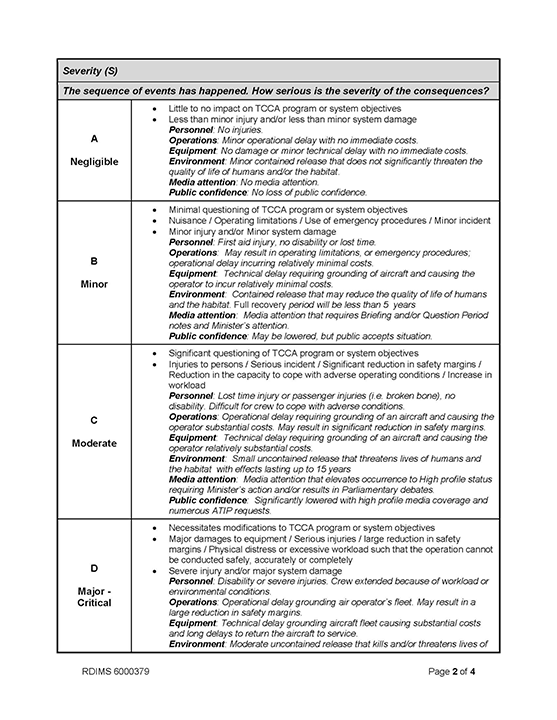
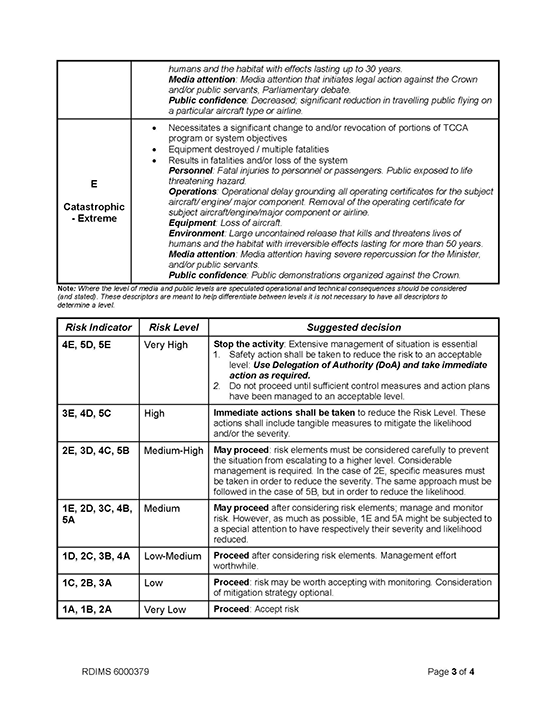
Source: Transport Canada
Appendix F – List of acronyms and abbreviations
- ADF
- automatic direction finder
- agl
- above ground level
- AME
- aircraft maintenance engineer
- ASD
- Transport Canada Aircraft Services Directorate
- ASIS
- Aviation Safety Information System
- asl
- above sea level
- ASSB
- Aircraft Services Service Bulletin
- BREA
- ArcticNet Beaufort Regional Environmental Assessment
- °C
- degrees centigrade
- CAD
- Civil Aviation Directive
- CAP
- corrective action plan
- CARs
- Canadian Aviation Regulations
- CCG
- Canadian Coast Guard
- CCGS
- Canadian Coast Guard Ship
- CDU
- control display unit
- CFIT
- controlled flight into terrain
- CO
- chief officer
- COM
- company operations manual
- CPR
- cardiopulmonary resuscitation
- CVR
- cockpit voice recorder
- CYSY
- Sachs Harbour
- DME
- distance measuring equipment
- EASA
- European Aviation Safety Agency
- ECS
- electronic chart systems
- ELT
- emergency locator transmitter
- ETA
- estimated time of arrival
- ETSO
- European Technical Standard Order
- FAA
- United States Federal Aviation Administration
- FDM
- fight data monitoring
- FDO
- flight deck officer
- FDR
- flight data recorder
- FFS
- flight following system
- FMS
- flight manual supplement
- FOQA
- flight operational quality assurance
- FRC
- fast rescue craft
- GFA
- Graphic area forecasts
- GPS
- global positioning system
- HO
- health officer
- HPTSS
- helicopter passenger transportation suit system
- HUET
- helicopter underwater egress training
- ICAO
- International Civil Aviation Organization
- IFAP
- Industrial Foundation for Accident Prevention
- ITS
- Integrated Technical Services
- JRCC
- joint rescue coordination centre
- LKP
- last known position
- LPN
- licensed practical nurses
- °M
- degrees magnetic
- MBB
- Messerschmitt-Bölkow-Blohm
- ME
- medical examiner
- METAR
- aerodrome routine meteorological reports
- MMS
- Maintenance Manual Supplement
- NDB
- non-directional beacon
- nm
- nautical miles
- NMEA
- National Marine Electronics Association
- OAT
- outside air temperature
- OIL PRESS
- oil pressure
- OIL TEMP
- oil temperature
- OPS 4
- major airframe inspection
- PFD
- Personal flotation device
- PI
- position interval
- PIC
- pilot-in-command
- PIF
- Pilot Information File
- PLB
- Personal locator beacons
- PTSS
- passenger transportation suit system
- PVI
- program validation inspections
- RCMP
- Royal Canadian Mounted Police
- RFM
- rotorcraft flight manual
- RN
- Registered Nurse
- ROV
- remotely operated vehicle
- RPN
- registered psychiatric nurse
- RS
- rescue specialist
- SAR
- search and rescue
- SHP
- shaft horsepower
- SI
- Transport Canada Staff Instruction
- sm
- statute miles
- SMS
- safety management system
- SOC
- Speciality Operations Catalogue
- SOPs
- standard operating procedures
- SOR
- statement of requirements
- STC
- supplemental type certificate
- TC
- Transport Canada
- TCCA
- Transport Canada Civil Aviation
- TSB
- Transportation Safety Board
- TSO
- Technical Standard Order
- ULB
- underwater locator beacon
- VDR
- voyage data recorder
- VFR
- visual flight rules
- VHF
- very high frequency