Risk of collision
Canadian North Inc. Boeing 737-36Q, C-GICN
and
Jazz Aviation LP (dba Air Canada Express)
de Havilland DHC-8-402, C-GGDU
Fort McMurray, Alberta
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Canadian North Inc. B737-36Q (registration C-GICN, serial number 29405) was operating as flight MPE9131 from Winnipeg, Manitoba, to Fort McMurray, Alberta. At the top of the descent, the flight crew briefed for a visual approach to Runway 25. When MPE9131 was at approximately 4 nautical miles on final, the airport environment was visually acquired and the flight crew inadvertently lined up with Taxiway J. At 1838:23 Mountain Daylight Time, in daylight, MPE9131 was abeam the threshold of Runway 25 and at 46 feet above ground level, while a Jazz Aviation LP de Havilland DHC-8-402, operating as flight JZA391, was proceeding eastbound on Taxiway J for departure on Runway 25. MPE9131 conducted a missed approach and returned for landing on Runway 25. Separation between the aircraft was 230 feet vertically and 46 feet laterally.
Factual information
History of the flight
On 04 August 2014 at 0730 Mountain Daylight Time,Footnote 1 MPE9131 departed Hamilton, Ontario, for Sydney, Nova Scotia, followed by several other legs westbound to terminate in Fort McMurray (CYMM), Alberta.
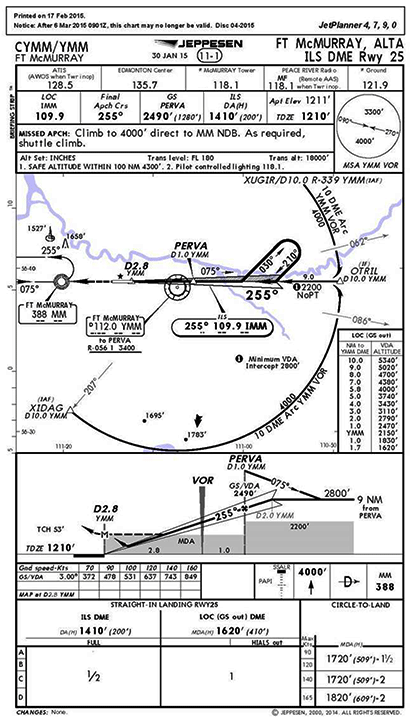
Prior to descent into CYMM, the flight crew obtained the automatic terminal information service (ATIS),Footnote 2 information Mike,Footnote 3 which stated that the visibility was 4 statute miles (sm) in haze; clouds were scattered at 4100 feet above ground level (agl); and the active runway was Runway 25. The flight crew briefed for a visual approach for Runway 25 with the approach aids set for the instrument landing system / distance measuring equipment (ILS/DME) (Appendix A). Landing performance was calculated based on a reference speed (Vref) of 134 knots at a landing weight of 114 558 pounds with flaps selected at 40°. The Canadian North Inc. standard operating procedures (SOPs) require that an instrument approach and instrument approach briefing be conducted whenever reported visibility is less than 5 sm.
At 1816, while descending out of 29 000 feet above sea level (asl), the flight crew of MPE9131 checked in with the Edmonton Area Control Centre (ACC). The Edmonton ACC controller acknowledged the call, advised the MPE9131 flight crew that the current ATIS for CYMM was information November, and instructed the aircraft to descend to and maintain 10 000 feet asl. The MPE9131 flight crew read back the altitude clearance but did not obtain or acknowledge ATIS information November. ATIS information November stated that visibility at CYMM was 2.5 sm in haze. The haze was due to forest fire smoke in the CYMM control zone.
At 1823, the ACC controller asked MPE9131 which approach they were planning, and the crew responded that they were set up for the ILS/DME approach for Runway 25. The ACC controller acknowledged, requested that MPE9131 reduce speed, and told them to expect vectors for spacing; MPE9131 was number 2 for the approach and cleared to descend to 8000 feet asl. At 1825, the ACC controller began giving vectors to MPE9131.
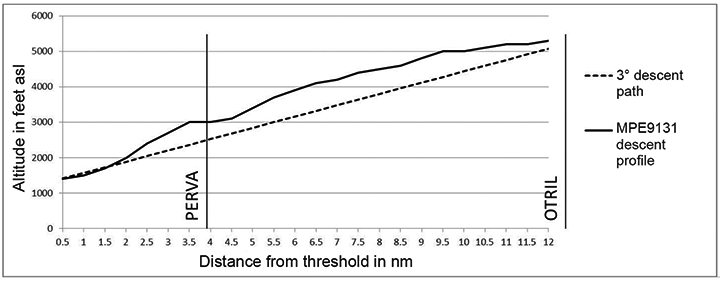
At 1830, MPE9131 was cleared direct to the intermediate fix OTRIL, 12.8 nm from the runway threshold, and to descend to 6000 feet asl. Over the next 5 minutes, MPE9131 was further cleared to 5000, 4000, and 3000 feet asl, and instructed to reduce its speed to 180 knots indicated airspeed.
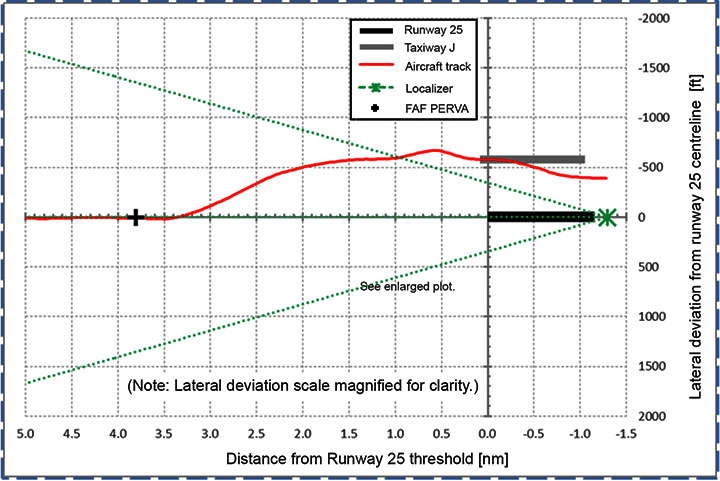
At 1835:46, the CYMM tower controller instructed a Cessna 172, which was orbiting to allow a regional jet to approach and land, to proceed direct to the threshold of Runway 25. At 1835:52, the Edmonton ACC controller cleared MPE9131 for the ILS/DME Runway 25 approach and instructed it to switch over to the CYMM tower frequency; MPE9131 was descending through 4000 feet at the time (Figure 1).
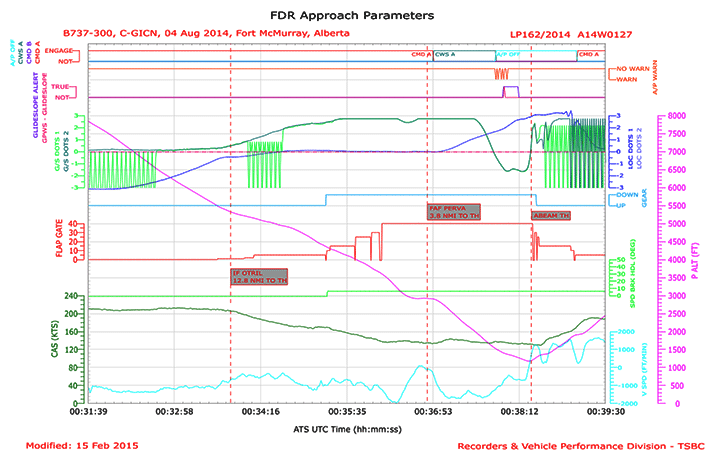
At 1836, the CYMM tower controller instructed the MPE9131 crew to reduce to their lowest speed and informed them that they were following a Cessna 172 that was at ½ mile on final. The MPE9131 crew advised that they were at their minimum safe speed. Flight data recorder airspeed showed the aircraft at 135 knots calibrated airspeed (CAS) at the time (Appendix B).
At approximately the same time, the pilot of a regional jet that had landed on Runway 25 and was taxiing for the main apron asked the ground controller why aircraft were landing directly into the sun, and reported that the smoke was making it difficult to see the runway environment. The controller responded that Runway 25 was in use because it was the calm wind runway as per the tower operations manual, but that the comment would be considered.Footnote 4
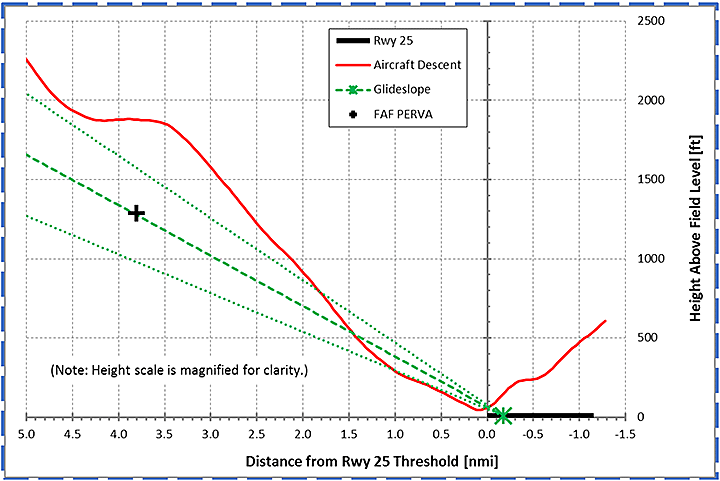
Approaching 3000 feet asl, MPE9131 was 2.5 dots above the glide slope as indicated on the glide slope deviation bar at 140 knots indicated airspeed . The autopilot was engaged and the mode control panelFootnote 5 for the aircraft had been configured for “altitude acquire” and the altitude select set to 3000 feet. The approach mode was armed with the localizer captured and the autothrottle set in speed mode on the mode control panel. At 1836:28, given the autopilot settings, MPE9131 levelled off at 3000 feet asl just prior to the final approach fix PERVA, which was not planned for by the flight crew. The autothrottle increased thrust to maintain the selected speed (Appendix B).
At 1836:45, JZA391 called the ground controller for instructions to taxi from the main apron to Runway 25. JZA391 was cleared to taxi to Runway 25 via the main apron and Taxiway J, and instructed to hold short of Runway 25.
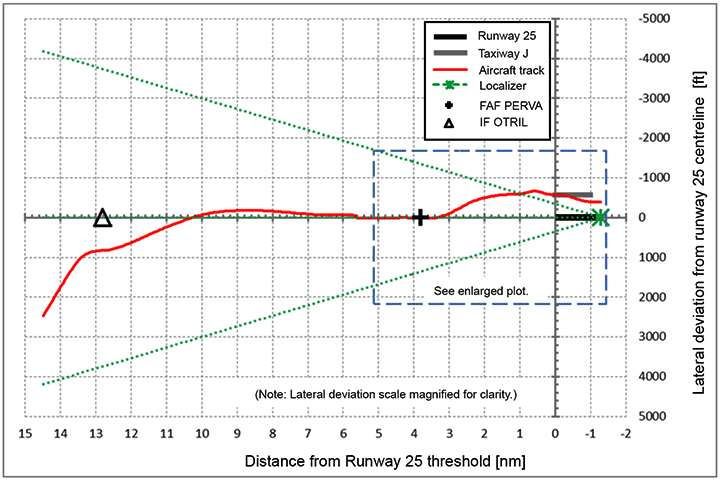
At 1836:54, while MPE9131 still had the autopilot engaged, the crew acquired visual contact with what they believed to be the runway environment. The crew used control wheel steering to manoeuvre the aircraft to the left and increase the rate of descent. The intent was to line up with what was believed to be Runway 25; however, the aircraft was in fact lining up with Taxiway J (Figure 2).

Runway 25 is equipped with a high-intensity simplified short approach lighting system with runway alignment indicator lights, which includes runway threshold and runway end lights. Runway 25 is also equipped with a 2-unit precision approach path indicator (P2) system.Footnote 6 The system was on, but the approach lighting was not selected on. NAV CANADA's Air Traffic Control Manual of Operations (ATC MANOPS)Footnote 7 states that airports equipped with approach lighting with variable-intensity setting shall set the approach lights at intensity level 4 during daylight hours when visibility is less than 3 sm.
At 1837:40, the CYMM tower controller called MPE9131 to advise that the Cessna 172 was clearing Runway 25 and MPE9131 was cleared to land. At that time, MPE9131 was approximately 690 feet agl with a descent rate of 1600 feet per minute, 136 knots CAS, 1.4 dots to the left of the localizer and 1.7 dots above the glide slope.
At 1837:51, both the autopilot and autothrottle were selected off and the pilot flying was in manual control of the aircraft's flight path and airspeed. The aircraft was descending through 400 feet agl at about 1200 feet per minute and 137 knots CAS.
At 1837:57, the aircraft position was descending through 1.4 dots below the nominal glide slope, and the enhanced ground proximity warning system initiated a glide slope alert. Lateral deviation was 1.9 dots to the left and still increasing, as the aircraft was now on a track toward Taxiway J rather than the centreline of Runway 25. The glide slope alert ended at 1838:11, with the aircraft still 1.6 dots below the nominal glide slope, and lateral deviation 2.6 dots to the left, approaching full deflection. The crew requested that the CYMM tower controller confirm that the runway was clear at this time. The tower controller responded that it was.
Shortly after, at 1838:17, JZA391 broadcast over the tower frequency that MPE9131 was lined up with the taxiway; MPE9131 was at approximately 85 feet agl.
At 1838:21, when it became clear to the crew of MPE9131 that the aircraft was lined up with Taxiway J, the crew initiated a go-around when the aircraft was at 46 feet agl (Figure 2), and, 2 seconds later, the aircraft crossed abeam the threshold of Runway 25, 2800 feet away from JZA391. When MPE9131 overflew JZA391, it was 230 feet above JZA391, and climbing.
Weather and visibility observations
Fort McMurray control tower weather and visibility data are determined by an automatic weather observation system (AWOS), which was fully operational and serviceable on the day of the occurrence. The visibility indicated by the AWOS, when available, is the primary source for tower operations. In addition, a controller may also provide tower-observed visibility. However, when ground visibility is reported, tower-observed visibility is considered advisory only. When AWOS visibility is not available, visibility can be determined by using a local area visibility chart produced by Environment Canada.Footnote 8 The Fort McMurray tower visibility chart depicts a 360° view of the area surrounding the control tower in ¾-, 6- and 30-sm ranges. For the 6-sm range, there are 4 communication towers depicted at just over 5 sm and one at 6 sm to the west. The visibility chart was last updated on 15 October 2001.
At the time of the occurrence, the tower controller, who was using a geographic feature not depicted on the visibility chart, estimated the visibility to be at least 3 sm. However, the visibility was variable depending on the position of the observer relative to the sun and because of haze from forest fire smoke.
During the controller's 8 years of experience as a flight service specialist and controller in Fort McMurray (see the section entitled “Fort McMurray tower controller below), he tended to seek visual confirmation of AWOS visibility with geographic features.
The AWOS hourly weather report for Fort McMurray airport that had been taken 38 minutes before the occurrence indicated that the winds were 5 knots, visibility was 4 sm in haze, and there was a scattered layer of clouds at 4100 feet agl. The temperature was 30 °C and the dew point was 9°C. The altimeter setting was 30.01 inches of mercury.
At 1808, 30 minutes before the occurrence, a special weather observation was issued at the Fort McMurray airport, indicating that the winds were 7 knots, visibility was 2½ sm in haze, and there was a broken layer of clouds at 3900 feet agl. The temperature was 30 °C and the dew point was 9°C. The altimeter setting was 30.01 inches of mercury.
At the time of the occurrence, the position of the sun was at an elevation of 21.42° and azimuth of 268.65° True, which was nearly aligned with the orientation of Runway 25 (270° True).
Fort McMurray tower controller
The tower controller was certified and licensed in accordance with the regulations at the time of the occurrence. The controller had 14 months of experience at the Fort McMurray tower as a qualified controller, and previously had 7 years of experience as a flight service specialist. In the 3 weeks leading up to the occurrence, the controller had worked 11 days and had had 10 days off. In the 3 days prior to the occurrence, the controller had worked 2 days and was off the day before the occurrence. On the day of the occurrence, the controller's shift began at 1435, and included a 1-hour break at 1630. Fatigue was not considered a factor at the time of the occurrence.
Flight crew
Records indicate that the flight crew were certified and qualified for the flight in accordance with existing regulations.
The captain had approximately 10 000 hours total flight time, with 500 hours on type. The captain was the pilot flying (PF) during the occurrence.
The first officer had approximately 3800 hours total flight time, with about 600 hours on type. The first officer was the pilot monitoring (PM) during the occurrence.
The day of the occurrence was the second day of a 4-day pairing. The previous day was a scheduled positioning flight to position the crew in Hamilton, Ontario. The captain arrived in Hamilton earlier in the day than the rest of the crew. The investigation determined that there was nothing to indicate that the captain's or first officer's performance was degraded by fatigue.
Both crew members had flown into the Fort McMurray airport since the new taxiway had been built. They both had significantly more experience at the airport prior to the construction of the new taxiway and were more familiar with the airport when the runway was the southernmost strip of asphalt.
Fort McMurray International Airport
Fort McMurray International Airport has a single runway (07/25), which is 7503 feet long and 150 feet wide (Appendix C). The runway is flanked by 2 parallel taxiways (G and J). Taxiway G is located north of the runway and runs east–west. It is connected to the runway thresholds via taxiways A and F, which are at 45° angles to the runway. Taxiway J lies south of the runway. It is 75 feet wide and joins the runway via Taxiway B (east of the threshold of Runway 07), Taxiway D (located at the midpoint of Runway 25), and Taxiway F ( located at the threshold of Runway 25). Both Taxiways B and F are perpendicular to the runway and have square corners.
Taxiway J was opened in April 2014, along with a new terminal building on the south side of the airport. It was designed in accordance with the requirements set out in Transport Canada TP 312, 4th edition, Aerodrome Standards and Recommended Practices. The standard does not discuss geometry of taxiway end designs.
Two aircraft had landed on Taxiway J while it was still under construction. The first occurrence was on 26 June 2012, involving a Cessna 182. The second occurrence was on 18 March 2014, involving a Cessna 185. No damage or injury had resulted from either incident.
As a countermeasure following those occurrences, a NAV CANADA operations directive was issued to Fort McMurray tower staff on 21 March 2014, instructing them to leave the runway edge lights and approach lighting for the runway in use on low setting during daylight hours. This practice was discontinued when a further operations directive was issued on 11 June 2014 that stated:
In consultation with local pilots and the Fort McMurray Airport Authority it has been decided that the risk of aircraft landing on Juliet has decreased to point where controller's [sic] are no longer required to leave the approach and runway edge lights on all day. The lights should only be used as required by MANOPS or as requested from pilots.
Please continue to monitor the approach path for arriving aircraft and if it appears that they may be lined up with Twy J instead of the runway, take appropriate action to advise the aircraft and intervene if necessary.Footnote 9
Aids to navigation
Navigational aids serving CYMM include the Fort McMurray non-directional beacon (MM NDB), the Fort McMurray very high frequency omnidirectional range (YMM VOR) with associated DME, and the IMMFootnote 10 ILS with associated DME. Runway 25 is served by ILS/DME, and area navigation and global navigation satellite system approaches.
The ILS for Runway 25 was operational, and there were no reported outages of navigation aids at the time of approach and landing.
Confusion between taxiways and adjacent runways
The TSB has previously investigated occurrences in which aircraft have mistakenly landed in areas adjacent to a runway: In 2001, a DHC-8 landed in a grass-covered area beside the runway in Peace River, Alberta (Aviation Investigation Report A01H0004). In that case, recent snowfall had obscured the runway, leaving uncovered a rectangular patch of darker grass that was parallel with, and adjacent to, the runway surface. The investigation found that, upon acquiring visual contact with the airport environment, the crew had seen a runway-shaped surface where they had expected the runway to be, and continued the approach to that area. Available cues that might have alerted the crew to the error prior to touchdown either had not been sufficiently compelling to cause them to question their belief that they were aligned with the runway, or had not been part of the crew's scan, since the focus of their attention had been directed outside the cockpit after transitioning to visual reference. The runway lights were on at the time of the occurrence. The runway was not equipped with runway-end identification lights or an omnidirectional approach lighting system.
While not an everyday occurrence, confusing taxiways for runways occurs often enough to warrant further study: according to a 2007 Federal Aviation Administration report,Footnote 11 there were 267 instances of pilots mistakenly landing on a taxiway parallel to a runway in the United States between 1962 and August 2007. These events, identified through U.S. National Transportation Safety Board and Aviation Safety Reporting System databases, occurred at 110 different airports and involved aircraft from the spectrum of operator types. There were multiple occurrences at 44 of the airports, with single occurrences at the remaining 66. It should be noted that these data included only aircraft that had actually landed on the taxiway; the number of instances of runway/taxiway confusion that were detected prior to landing is likely much higher.
The report examined the factors that contributed to runway/taxiway confusion at the airports with the greatest frequency of occurrences; among them were approaches into the sun that obscured runway and taxiway markings, and taxiway geometry (such as a squared-off end) that made the taxiway resemble a runway.
At one airport studied, the majority of the pilots involved were local to the airport and, as such, were familiar with the problem and the potential for confusion. The fact that pilots who had been forewarned of the problem nonetheless mistakenly landed on the taxiway demonstrates how compelling the visual cues leading to this error can be. In other instances, aircraft involved in taxiway landing incidents were conducting ILS approaches at the time. However, once the crew acquired visual contact with the landing surface, their attention was directed outside at the surface that they believed to be the runway, localizer deviations were not monitored, and the crew were not alerted to their error.
Effective countermeasures mentioned in the study included:
- Constructing taxiways to look less like runways (e.g., angle the end of the taxiway at the threshold of the runway)
- Covering portions of the taxiway, particularly a squared-off end, with material such as artificial turf to make the taxiway look less like a runway
- Providing warnings to pilots as a first line of defence (e.g., on ATIS and aeronautical charts)
- Using lights to make the runway more conspicuous (omnidirectional runway-end identification lights were found to be particularly helpful)
- Using lights that warn against landing on the taxiway (e.g., a raised lighted X at the end of the taxiway, or an in-pavement lighted X on the taxiway).Footnote 12
Transitioning to flight by visual reference and runway identification
The visual cues necessary for a pilot to transition to the visual segment for landing are described in the TC AIM:
The visual references required by the pilot to continue the approach to a safe landing should include at least one of the following references for the intended runway, and should be distinctly visible and identifiable to the pilot by:
- the runway or runway markings;
- the runway threshold or threshold markings;
- the touchdown zone or touchdown zone markings;
- the approach lights;
- the approach slope indicator system;
- the runway identification lights;
- the threshold and runway end lights;
- the touchdown zone light;
- the parallel runway edge lights; or
- the runway centreline lights.Footnote 13
The task of transitioning between the instrument segment and the visual segment of the approach involves the PF acquiring adequate visual references as described above, while the PM monitors the progress of the flight. The timing of seeking external cues will depend on the pilots' expectation of when they anticipate acquiring visual references, based largely on knowledge of the weather conditions. During daytime visual conditions, the runway itself will be the most obvious and compelling visual cue available. By regulation, only one visual reference is required to continue with an approach; once pilots have acquired what they believe to be the runway environment, they are less likely to actively seek additional visual cues to confirm their earlier perception.
During highly routine tasks, perceptual confusion can occur when an observer sees something that closely resembles what they expected to see. Believing they have correctly identified an object, they may initiate a sequence of actions associated with it. In the absence of compelling cues that might cause the observer to question their original perception, no further cognitive effort will be made to confirm that the object has been correctly identified.
The characteristics of these fairly common errors suggest that they occur because the recognition schemata accept as a match for the proper object something that looks like it, is in the expected location or does a similar job. These slips could arise because, in a highly routinized set of actions, it is unnecessary to invest the same amount of attention in the matching process. … With oft-repeated tasks, it is likely that the recognition schemata, as well as the action schemata, become automatized to the point that they accept rough rather than precise approximations to the expected inputs. This degradation of the acceptance criteria is in keeping with ‘cognitive economics' and its attendant liberation of attentional capacity.Footnote 14
Countering potential illusions during the visual segment of the approach
A number of well-known visual illusions can affect a pilot's perception of height on approach. Aspects of the visual scene, including unfamiliar runway size and width, sloping terrain before the runway, the slope and texture of the runway itself, and a lack of lights leading up to the runway at night (“black hole effect”) can lead to misperceptions of height on approach.Footnote 15 These illusions reduce the reliability of visual estimations of height on approach and reinforce the importance of using all available cues to confirm the crew's perception of the situation.
In developing its approach and landing accident reduction (ALAR) tool kit, the Flight Safety Foundation identified frequently cited causal factors in approach and landing accidents. Those most relevant to this occurrence were: inadequate reference to instruments during the visual segment of the approach, failure to detect the deterioration of visual references, and the involvement of both pilots in the identification of visual references contributing to inadequate monitoring of the flight instruments.Footnote 16
The Flight Safety Foundation identifies best practices for avoiding these pitfalls, including: maintaining an instrument scan to touchdown, consistent use of the most precise instrument approach guidance available, consistent use of visual approach aids during the visual segment, and the use of effective crew coordination techniques in both visual and instrument conditions.
Altitude calls and excessive-parameter-deviation calls should be the same for instrument approaches and for visual approaches, and should be continued during the visual portion of the [approach] (including glideslope deviation during an ILS approach or vertical-speed deviation during a nonprecision approach).Footnote 17
Unstable approaches
General
Research has shown that unstable approaches present a high risk to safe flight operations. As shown in previous investigations by the TSB and foreign agencies, negative outcomes include tail strikes, runway overruns, and controlled flight into terrain (CFIT). While there are some defences in place to mitigate the risk of unstable approaches, not all defences are employed by all operators. Defences are available to air carriers to mitigate the risks associated with unstable approaches and their consequences. These mainly administrative defences include:
- a company stabilized-approach policy, including a no-fault go-around policy;
- operationalized stable approach criteria and SOPs, including crew phraseology;
- effective crew resource management, including empowering of first officers to take control in an unsafe situation;
- use of flight data monitoring programs to monitor SOP compliance with stabilized approach criteria;
- use of line-oriented safety audits or other means, such as proficiency and line checks, to assess crew resource management practices and identify crew adaptations of SOPs;
- non-punitive reporting systems (to report occurrences or unsafe practices); and
- use of terrain awareness and warning systems.Footnote 18
Unstable approach and go-around study
The results of a study of pilots' experiences conducting unstable approaches and go-arounds were reported in the April 2013 issue of Aero Safety World.Footnote 19 More than 2000 pilots were asked to provide detailed accounts of recent experiences with approaches that were unstable below the stabilized approach height and that either resulted in a go-around or were continued to a landing. The study found that the decision to continue with an unstable approach was associated with lower levels of perceived risks associated with such an approach.
The study stated, in part:
So why do pilots forgo the GA [go-around] decision in 97 percent of UAs [unstable approaches]? We have discovered that continuing to fly a UA is associated with much lower levels of perceived risk about the unmanageability of instabilities experienced at and below SAH [stable approach height] … With lowered risk assessment comes the decision to continue to fly a UA rather than execute a GA. And because most of the time we “get away with it,” managing the aircraft's energy to a successful landing, this reinforces the belief that the risks of instability are manageable and perpetuates the cycle of chronically forgoing the GA.Footnote 20
In particular, the study found that pilots were more likely to continue with unstable approaches in visual meteorological conditions and where environmental factors that might increase operational complexity—such as wind shear, turbulence, and contaminated runways—were absent. The authors suggest that these factors increase the pilot's perception that an approach can be salvaged, reducing the perceived risk associated with continuing the approach.
The study also found a lower incidence of unstable approaches being continued to landing in cockpit environments that were described as being more supportive, less judgmental, and more accepting of challenge, and where there were more frequent conversations with respect to operational and flight risks.
Other TSB investigationsFootnote 21 have shown that non-adherence to company SOPs related to stabilized approaches is not unique to Canadian North Inc.
Canadian North Inc. stable approach criteria
Canadian North Inc. stable approach criteria are published in the 737-300 SOPs manual. The SOPs incorporate standard calls that must be made by crews to coordinate the duties of the PF and PM and to identify any deviations from the standard. These SOPs are consistent with the recommendations from the Flight Safety Foundation study.Footnote 22 The SOPs recommend the following:
Maintaining a stable speed, descent rate and vertical/lateral flight path in landing configuration is commonly referred to as the stabilized approach concept.
Any significant deviation from planned flight path, airspeed or descent rate should be announced. The decision to execute a go-around is no indication of poor performance.
Note: Do not attempt to land from an unstable approach.Footnote 23
The SOPs further state that an approach that becomes unstable below 1000 feet above field elevation (AFE) in instrument meteorological conditions or below 500 feet AFE in visual meteorological conditions requires an immediate go-around.
The SOPs also state:
The conditions should be maintained throughout the rest of the approach for it to be considered a stabilized approach. If the above criteria cannot be established and maintained at and below 500 feet AFE, initiate a go-around.
At 100 feet HAT [height above threshold] for all visual approaches, the airplane should be positioned so the flight deck is within, and tracking to remain within, the lateral confines of the runway edges extended.
As the airplane crosses the runway threshold it should be:
- Stabilized on approach airspeed to within + 10 knots until arresting descent rate at flare.
- On a stabilized flight path using normal maneuvering.
- Positioned to make a normal landing in the touchdown zone (the first 3,000 feet or first third of the runway, whichever is less).
Initiate a go-around if the above criteria cannot be maintained.Footnote 24
Go-arounds conducted by Canadian North Inc. flight crews during training were in the flight regime close to approach minimums or as part of the low-energy awareness training,Footnote 25 where more aggressive pitch and power inputs are required. There are no specific training scenarios dealing with go-arounds conducted earlier in the approach or from unstable conditions, nor are they specifically required by regulation.Footnote 26
Canadian North Inc. standard call-outs
The Canadian North Inc. SOPs outline the expected call-outs by the PM during the approach and the expected response by the PF. These include excessive sink rate and excessive deviation from the approach profile. The PM is expected to call out the deviation (e.g. “sink rate” or “glide slope”) and the expected response from the PF is “correcting.”
There is no difference in standard call-outs in instrument flight rules (IFR) or visual flight rules (VFR) conditions and the SOPs clearly state, “the standard call-outs required during CLIMB, DESCENT and FINAL APPROACH for either IFR or VFR conditions,” and that “the [PM] shall accomplish these call-outs for every flight.”Footnote 27
The investigation could not determine what call-outs were made during the approach, because the cockpit voice recorder (CVR) had been overwritten.
Transportation Safety Board of Canada Recommendation A14-01—Unstable approaches
On 25 March 2014, the TSB released Aviation Investigation Report A11H0002 on the CFIT accident involving First Air flight 6560 in Resolute Bay, Nunavut, that occurred on 20 August 2011. The investigation concluded that a combination of factors contributed to the accident. The aircraft did not intercept the runway localizer (alignment) beam and instead diverged to the right and ultimately hit a hill. Fundamental to the Board's findings was the fact that an unstable approach was continued.
Therefore, the TSB recommended that:
Transport Canada require CARs Subpart 705 operators to monitor and reduce the incidence of unstable approaches that continue to a landing.
Transportation Safety Recommendation A14-01
Transport Canada determined that this hazard could be mitigated through an air operator's existing safety management system (SMS). On 27 June 2014, Transport Canada issued Civil Aviation Safety Alert (CASA) No. 2014-03—Using SMS to Address Hazards and Risks Associated with Unstable Approaches to all subpart 705 operators. The purpose of this CASA was threefold:
- To request Canadian air operators operating under subpart 705 of the Canadian Aviation Regulations (CARs) that they use—on a voluntary basis—their existing Safety Management System (SMS) to address and mitigate hazards and risks associated with unstable approaches;
- To advise 705 operators that beginning approximately one year after publication of this CASA, Transport Canada Civil Aviation (TCCA) plans to direct specific surveillance activities to evaluate the effectiveness of voluntary compliance with this document and will begin looking for evidence of effective mitigations of this hazard; and,
- As the hazards and risks associated with unstable approaches are not limited to 705 operators, this CASA also serves to raise the concern to 703 and 704 operators who are not yet required to have a SMS, and encourage them to address the issue voluntarily.
CASA No. 2014-03 included the following recommended action:
TCCA [Transport Canada Civil Aviation] requests that this hazard be assessed and mitigated through appropriate use of the following (but not limited to) SMS components:
- safety oversight (reactive and proactive processes);
- training and awareness (promotions);
- voluntary use of Flight Data Monitoring (in order to gain a greater understanding of unstable approaches and the causes.)Footnote 28
Until the results of this surveillance are analyzed, it is difficult to determine what measures airlines have implemented and whether they are effective in addressing the underlying safety deficiency. It will be some time before the impact of CASA 2014-03 can be validated. Therefore, the response to Recommendation A14-01 was assessed as “Satisfactory in Part.”
TSB Watchlist
Approach-and-landing accidents are a 2014 Watchlist issue
The Watchlist is a list of issues posing the greatest risk to Canada's transportation system; the TSB publishes it to focus the attention of industry and regulators on the problems that need addressing today.
Approach-and-landing accidents are an issue included on the TSB's 2014 Watchlist and, as this occurrence demonstrates, landing accidents and incidents continue to occur at Canadian airports.
The TSB calls on TC and operators to do more to reduce the number of unstable approaches that are continued to a landing.
Occurrence reporting
Aviation occurrences are reported to the TSB from various sources, including safety notifications from government agencies and aviation companies, and confidential reports obtained from the TSB's confidential SECURITAS program.
In this occurrence, the TSB received an aviation occurrence report (AOR) from NAV CANADA. The summary of the occurrence provided on the AOR stated, “Aircraft conducted a missed approach due to being lined up for Taxiway J. Two IFR departures received minimal delays.”Footnote 29
Based on the information provided in the AOR, the occurrence was assessed as not meeting the mandatory reporting criteria in the Transportation Safety Board Regulations,Footnote 30 and was not followed up. Additionally, the SMS report submitted by the flight crew to Canadian North Inc. did not prompt the company to notify the TSB.
Two days after the occurrence, the TSB was made aware of the seriousness of the situation when it was contacted by the Jazz LP SMS department. The TSB then initiated an investigation, but the cockpit voice recorder data had already been overwritten.
TSB laboratory reports
The TSB completed the following laboratory report in support of this investigation:
- LP162/2014–FDR [flight data recorder] Analysis
Analysis
Taxiway confusion
One of the key tasks involved in transitioning from an approach to a landing is visually identifying the runway or runway environment. The potential for confusion exists where an object with the approximate size and shape of the runway is identified in the expected location of the runway. This confusion has been known to result in a taxiway parallel to the intended runway being misidentified as the runway.
A number of factors prevail in instances where aircraft have mistakenly landed on a taxiway, including environmental factors that obscure details of the runway and airport geometry that makes the taxiway look more like a runway.
Environmental factors
In this occurrence, the flight crew encountered lower visibility than they had anticipated. Their ability to identify the runway environment was compromised by haze from forest fire smoke, compounded by the aircraft's approach into the setting sun.
Once the taxiway had been identified as the runway, both pilots focussed their attention outside the aircraft, and cues that could have alerted the crew to their error were not assimilated. Such actions have been observed in previous instances of aircraft landing on taxiways and are consistent with errors of perceptual confusion: once an object is believed to have been identified, little cognitive effort is invested in confirming that it is the correct item.
A visual approach was conducted in weather conditions below visual flight rules (VFR) limits, which resulted in the flight crew experiencing visual illusions and inadvertently identifying Taxiway J as Runway 25.
Airport geometry
Several factors consistent with other instances of taxiway/runway confusion were present in this occurrence. Perceptual confusion occurred during the routine task of identifying the runway. In the low visibility and sun, the position of the taxiway south of Runway 25 and its squared-off end (which resembles the end of a runway) contributed to the flight crew identifying Taxiway J as Runway 25.
Taxiway J had been in service for approximately 4 months prior to the occurrence. Although both crew members had flown into Fort McMurray (CYMM) since the new taxiway had been built, they both had significantly more experience at the airport prior to the construction of the new taxiway and were more familiar with the airport when the runway was the southernmost strip of asphalt.
If standards do not provide detailed guidance on the geometry to be used in taxiway-end design, taxiways with squared-off ends risk looking like runways, which can contribute to perceptual confusion in flight crews.
Approach lighting
Several factors resulted in the controller not turning on the approach lighting as required by NAV CANADA's Air Traffic Control Manual of Operations (ATC MANOPS) for the visibility that prevailed. The controller estimated the visibility to be greater than that reported by the automatic weather observation system (AWOS). The visual cues that supported the controller's assessment that visibility was greater than 3 statute miles (sm) included:
- cloud ceiling of 3900 feet above ground level (agl);
- viewing the approach end of the runway facing away from the sun, which resulted in the perception of better-than-actual visibility; and
- using a ridgeline that is not identified on the 13-year-old Environment Canada visibility chart, given its lack of markers between 1 and 4 sm.
The controller had assessed the visibility as higher than reported and, therefore, did not turn on the approach lighting. This contributed to the flight crew not identifying Runway 25.
Approach stability
Just prior to the final approach fix, the autopilot levelled the aircraft off at 3000 feet above sea level; the flight crew did not plan for this. At the time, the pilot flying saw what was believed to be the runway, and selected control wheel steering mode to manoeuvre the aircraft toward the apparent runway. The approach was not stable at 1000 feet agl and below, and the flight crew never identified the need to initiate a go-around. The aircraft was initially high on the glide slope and continued past 1000 feet agl with a significant rate of descent. The aircraft was lined up with Taxiway J, which was half the width of the runway; this led to the perception of being high on approach. In the absence of additional references, the flight crew continued below the glide slope in an attempt to recreate the expected visual scene.
Factors that have been shown to increase the likelihood of a continued unstable approach were present. For example, there were no issues—such as wind shear or a contaminated runway—complicating the approachand both flight crew members had focussed their attention on visual cues outside the aircraft. To overcome these factors, the Flight Safety Foundation has identified best practices, which encourage the use of all available cues while implementing procedures that focus the crew's attention on those cues, such as the continuation of standard calls throughout the visual segment.
Canadian North Inc. standard operating procedures (SOPs) require the PM to call excessive deviations in sink rate or approach profile in both visual and instrument conditions. In this occurrence, the focus of both crew members was outside the cockpit during the late stages of the approach and, therefore, these deviations were not noted by the PM. As a result, the degree of instability of the approach was not appreciated and a go-around was not initiated.
While Canadian North Inc. had a stabilized approach policy and criteria, a no-fault go-around policy, and SMS hazard and occurrence reporting policy, the unstable approach was continued.
The flight crew did not adhere to standard procedures, which required the monitoring of all available cues during the approach and landing. With both flight crew members looking out the window during the late stages of the approach, the instability of the approach was not identified and a go-around was not conducted.
Current defences against continuing unstable approaches have proven less than adequate. Unless further action is taken to reduce the incidence of unstable approaches that continue to a landing, the risk of CFIT and of approach and landing accidents will persist.
Go-around training
The go-around procedure in the Canadian North Inc. SOPs is designed for scenarios close to approach minimums, and near obstacles and terrain where aircraft climb performance is critical. A go-around conducted at this point is required to be more aggressive in pitch and power application than one conducted earlier in the approach. Training scenarios that include go-arounds following an unstable approach may increase the likelihood that pilots will do so during active flight operations.
Visual approaches conducted during instrument conditions
Prior to descent, the flight crew obtained the automatic terminal information service (ATIS) information Mike, which stated that the visibility was 4 sm in haze; clouds were scattered at 4100 feet above ground; and the active runway was Runway 25. The flight crew briefed for a visual approach for Runway 25 with the approach aids set for the ILS/DME Runway 25 approach.
ATIS information Mike was issued at 1809. As the weather at CYMM continued to change, an updated automatic weather briefing, ATIS information November, was issued 5 minutes later, stating that visibility at CYMM was 2.5 sm in haze. The haze was due to forest fire smoke in the CYMM control zone.
The weather conditions at CYMM during the arrival of MPE9131 were such that a visual approach was not appropriate as per the Canadian North Inc. SOPs and a full instrument meteorological conditions approach briefing should have been carried out. Furthermore, MPE9131 was cleared for an ILS/DME approach to Runway 25 as the airfield was below VFR limits.
Even though the flight crew did not get ATIS information November, in review of both ATIS weather briefings, the visibility at all times was below what was appropriate to conduct a visual approach.
If crews do not rigorously adhere to procedures that facilitate the monitoring of all available cues during the approach and landing, there is an increased likelihood of over-reliance on visual cues in the late stages of the approach, which increases the risks associated with visual illusions and unstable approaches.
Occurrence reporting
Expeditious and accurate reporting is required in order to fully understand the flight crew interaction and crew resource management within the cockpit environment, and for the TSB investigators to assess why incidents happen and what the contributing safety deficiencies may be. In the event that an accident does occur, recordings from flight and voice recording systems provide information essential to the identification of safety deficiencies.
MPE9131 was equipped with a flight data recorder (FDR) and a cockpit voice recorder (CVR), as required by regulation. Since the occurrence was not accurately and promptly reported to the TSB, several days elapsed before the TSB acquired sufficient data to fully understand the severity of the occurrence. During that time, the aircraft continued daily operations, and critical data recorded on the CVR was overwritten. The FDR data was retrieved and was essential to the investigation.
If occurrences are not reported as per the Transportation Safety Board Regulations, there is a risk that data (e.g., cockpit voice recorder data) may be lost, and, with it, the opportunity to identify safety deficiencies.
Findings
Findings as to causes and contributing factors
- A visual approach was conducted in weather conditions below visual flight rules limits, which resulted in the flight crew experiencing visual illusions and inadvertently identifying Taxiway J as Runway 25.
- Perceptual confusion occurred during the routine task of identifying the runway. The position of the taxiway south of Runway 25 and its squared-off end, which resembles the end of a runway, contributed to the flight crew identifying Taxiway J as Runway 25.
- The controller had assessed the visibility as higher than reported by the automatic weather observation system and, therefore, did not turn on the approach lighting. This contributed to the flight crew not identifying Runway 25.
- The flight crew did not adhere to standard operating procedures, which required the monitoring of all available cues during the approach and landing. With both flight crew members looking out the window during the late stages of the approach, the instability of the approach was not identified, and a go-around was not conducted.
Findings as to risk
- If crews do not rigorously adhere to procedures that facilitate the monitoring of all available cues during the approach and landing, there is an increased likelihood of over-reliance on visual cues in the late stages of the approach, which increases the risks associated with visual illusions and unstable approaches.
- If standards do not provide detailed guidance on the geometry to be used in taxiway-end design, taxiways with squared-off ends risk looking like runways, which can contribute to perceptual confusion in flight crews.
- If occurrences are not reported as per the Transportation Safety Board Regulations, there is a risk that data (e.g., cockpit voice recorder data) may be lost, and, with it, the opportunity to identify safety deficiencies.
Safety action
Safety action taken
Fort McMurray Airport Authority
Following the occurrence, the Fort McMurray Airport Authority issued a Notice to Airmen (NOTAM) stating: “Caution: Do not confuse Txy J with Rwy 07/25.” In addition to the NOTAM being issued, the cautionary note will also be included in the Fort McMurray (CYMM) automatic terminal information service (ATIS) broadcast until the caution is published in the April 2015 revision of NAV CANADA's Canada Flight Supplement (CFS). The caution has been incorporated in the 13 November 2014 revision of NAV CANADA's Canada Air Pilot [CAP 3].
NAV CANADA
NAV CANADA worked with the CYMM Airport Authority to ensure caution notes were added to the CFS and CAP.
- On 20 August 2014 an AMEND PUB NOTAM was issued to add a caution to the CFS and CAP about the danger of confusing Taxiway J with the runway. This submission to Aeronautical Information Services was done by the NAV CANADA Manager with approval and cooperation from the Airport Authority. In addition to this NOTAM being added to the NOTAM database, it was also included on the CYMM ATIS until it was subsequently published in the CAP in November.
- On 13 November 2014 a CAUTION was added to the CAP Aerodrome Chart for CYMM to warn IFR pilots: “Do not confuse Twy J with Rwy 07/25.”
- On 25 June 2015 the following was added to the CAUTION section of the CFS for Fort McMurray: “Do not confuse Twy J with Rwy 07/25.”
Representatives of NAV CANADA and the Meteorological Service of Canada communicated regarding the Fort McMurray Tower Visibility Chart. The Meteorological Service has advised NAV CANADA that a high priority would be placed on the production of an updated visibility chart, expected to be ready in the summer or early fall of 2015.
Canadian North Inc.
Following the occurrence, Canadian North Inc. issued a memorandum to all pilots on 12 August 2014, to raise awareness of mistaking CYMM Taxiway J for Runway 25. In September 2014, the captain and first officer underwent additional simulator and classroom training related to go-around procedures at various points on the approach.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .
Appendices