Collision with terrain
Hydro One Networks Inc.
Airbus Helicopters AS 350 B2 (helicopter), C-GOHS
Tweed, Ontario, 8 NM NNE
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Executive summary
On 14 December 2017, a Hydro One Networks Inc. Airbus Helicopters AS 350 B2 helicopter (registration C-GOHS, serial number 3240) equipped with an external platform, was transporting crews of power line technicians between a staging area and transmission towers in an area located 8 nautical miles north-northeast of Tweed, Ontario.
At 1144 Eastern Standard Time, the pilot picked up a crew of 3 power line technicians near the bottom of a tower for a return flight to the staging area. It had become common practice for power line technicians to attach tool bags and other small items to the external platform for flights to and from work sites. In line with this practice, the technicians attached a few items to the platform while boarding the helicopter, and then took their seats in the aft cabin.
The practice of carrying external loads attached to the platform was not a formalized procedure at the company and, as a result, adequate controls were not in place to ensure that these objects were properly stored or secured. Consequently, an empty canvas supply bag with an attached carabiner that was being carried on the platform was not adequately secured before the helicopter departed for the return flight to the staging area.
When the helicopter was 0.26 nautical miles from the staging area, the canvas bag separated from the platform and struck the helicopter's tail rotor, causing significant damage, severe imbalance, and intense vibration.
Shortly after, while the pilot was attempting to land, the helicopter's tail rotor, tail rotor gearbox, and vertical fin separated from the helicopter. The helicopter became uncontrollable and collided with terrain. The 3 power line technicians were unrestrained and became separated from the helicopter, either slightly before or during the impact, and received fatal injuries from contact with the helicopter or the surrounding terrain. The pilot was fatally injured on impact. The helicopter was destroyed.
Each seat in the aft cabin was equipped with a safety belt that included a detachable shoulder harness; however, the harnesses had been rolled up and taped with electrical tape before the flight, preventing them from being used. Transport Canada regulations require the use of these safety belts; however, the current definition of a safety belt in the regulations was interpreted to mean that compliance with the regulations could be achieved by using the lap strap with the shoulder harness or the lap strap alone.
In addition to not being able to attach the shoulder harnesses, the technicians involved in this occurrence did not attach their lap straps either, possibly because they perceived the risk on the short flight to be low, or because they found it difficult to attach the lap straps over their cold weather gear.
From 1990 to 2018, the TSB investigated many accidents involving aircraft that were equipped with detachable shoulder harnesses where it was determined that the harnesses were not being worn at the time of the accident. Of the 62 accidents identified, 33 were fatal, resulting in 68 deaths. Of those 68 deaths, 37 were individuals who had not been wearing the available shoulder harness.
Although the survivability of these 62 accidents varied, in many cases, the use of shoulder harnesses could have improved the occupants' chances of survival and egress. While the interpretation of the regulations was not the only reason for not wearing the shoulder harness in the cases examined, in this occurrence, the ambiguity did affect their use.
Therefore, the Board recommends that
the Department of Transport amend the Canadian Aviation Regulations to remove any ambiguity associated with the definition of “safety belt.”
TSB Recommendation A19-01
1.0 Factual information
1.1 History of the flight
At 0845Footnote 1 on 14 December 2017, a Hydro One Networks Inc. (Hydro One) Airbus Helicopters AS 350 B2 helicopter (registration C-GOHS, serial number 3240) equipped with an external platform, known as an Air Stair, departed from a helipad on Industrial Park Road in Tweed, Ontario, with only the pilot on board. The helicopter was headed to a staging area about 8 nautical miles (NM) north-northeast of Tweed to transport power line technicians (PLTs)Footnote 2 between a staging area and transmission towers. The pilot landed at the staging area at 0852 and shut down the helicopter.
Shortly thereafter, a tailboard meetingFootnote 3 was held with all Hydro One employees at the staging area to discuss the work planned for the day. The pilot then held an additional tailboard meeting with all the PLTs he would be transporting to and from the transmission towers that day. A Hydro One occupational health and safety representative attended both tailboard meetings.
The pilot's tailboard meeting consisted of a standard safety briefing about the helicopter, including standard operating procedures to be followed when approaching, boarding, and exiting the helicopter. The briefing included the use of seatbelts and the location of safety equipment. It was reported that the pilot indicated where the passengers were to store their equipment.
The pilot also mentioned that, because of the cold temperature, he would not be removing the right cabin doors and using the Air StairFootnote 4 to perform aerial transfers as he had done previously. Instead, the PLTs would be dropped off at the bottom of the towers and would climb up.
When the briefing was complete, the helicopter took off at 0939 to transport the first crew to its assigned transmission tower. The pilot then transported another crew to a different transmission tower and returned to the staging area at 1116.
At 1139:13, the pilot departed the staging area to start bringing the crews back for lunch. He headed east along the transmission line to a transmission tower 2.25 NM away at 1142:09. The pilot kept the helicopter running as the PLTs boarded and stored their equipment.Footnote 5
It could not be determined which door the PLTs used to board the helicopter; however, it is common practice for the PLTs to board through the right cabin door, and in doing so climb the steps of the Air Stair.
A large pulley and 2 soft-sided tool bags with fabric straps (referred to in this report as “nose bags”) that were partially filled with various pieces of equipment, were secured to the Air Stair with carabiners. The pilot then took off at 1144:09 and headed west, back to the staging area, flying at approximately 250 feet above ground level (AGL).
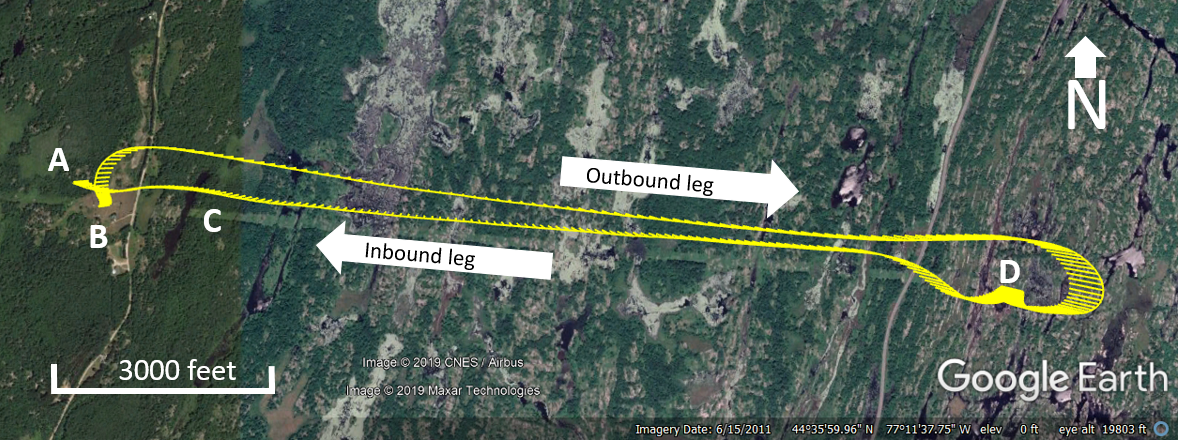
At 1145:54, the pilot started the descent to land. At 1146:09, the helicopter was about 0.26 NM from the staging area and travelling at a speed of 51 knots at 230 feet AGL when a 4‑foot‑long empty canvas supply bag (referred to in this report as a “preform bag”)Footnote 6 with an attached carabiner struck the tail rotor and broke the tip off one of the tail rotor blades, including the balance weight.
The investigation was able to determine that the preform bag and carabiner were most likely on the Air Stair itself or inside one of the nose bags attached to the Air Stair before they struck the tail rotor; however, their exact location or how or if they were attached could not be determined.
The pilot was initially able to maintain control of the helicopter and continued the approach to the staging area. He did not make any radio transmissions to the staff on the ground at the staging area.
When the helicopter was at a height of about 75 feet AGL, the tail rotor, tail rotor gearbox, and vertical fin separated from the tail boom. The helicopter departed from controlled flight, climbed, began to rotate rapidly to the left, and then rapidly descended. At 1146:42, the helicopter struck the surrounding trees and then the ground about 400 feet northwest of its intended landing site (Figure 1). All 3 passengers became separated from the helicopter before impact and were fatally injured. The pilot was also fatally injured.
- Accident site
- Staging area
- Preform bag
- Transmission tower
Hydro One employees who witnessed the crash rushed to the helicopter. A supervisor called 911 immediately after the helicopter crashed, and emergency services arrived on site shortly thereafter.
The emergency locator transmitter activated during the accident, and the signal was detected by Cospas-SarsatFootnote 7 at 1152.
1.2 Injuries to persons
The 3 passengers, who had become separated from the helicopter before impact, received fatal injuries from contact with the ground or the helicopter itself. The pilot, who had remained seated in the cockpit with his seat belt and shoulder harness fastened, also received fatal injuries.
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | 1 | 3 | – | 4 |
| Serious | 0 | 0 | – | 0 |
| Minor/None | 0 | 0 | – | 0 |
| Total | 1 | 3 | – | 4 |
1.3 Damage to aircraft
When the preform bag and carabiner struck and damaged the tail rotor, the dynamic unbalance created by the loss of the blade tip and balance weight caused intense vibration. The vibration subsequently caused a total failure of the whole tail rotor assembly, which separated from the tail boom, followed by the vertical fin.
The loss of the tail rotor and vertical fin resulted in the helicopter becoming uncontrollable, and during its uncontrolled rapid descent it struck nearby trees and then the ground. The helicopter was destroyed during the accident sequence (Figure 2).

1.4 Other damage
Not applicable.
1.5 Personnel information
1.5.1 Pilot
Records indicate that the pilot was certified and qualified for the flight in accordance with existing regulations.
The pilot had been hired by Hydro One in 2009. He had completed a recurrent training flight on 26 October 2017, which included training on tail rotor control system failures and tail rotor failures while in hover.
| Pilot licence | Commercial pilot licence - helicopter |
|---|---|
| Medical expiry date | 01 February 2018 |
| Total flying hours | 6585 |
| Flight hours on type | 5605 |
| Flight hours in the last 7 days | 15.6 |
| Flight hours in the last 30 days | 29 |
| Flight hours in the last 90 days | 112.7 |
| Flight hours on type in the last 90 days | 112.7 |
| Hours on duty prior to the occurrence | 4.3 |
| Hours off duty prior to the work period | 13 |
1.5.2 Power line technicians
The 3 passengers were employed by Hydro One as PLTs. One was an apprentice, and the other 2 were certified journeypersons. They had all completed the required training for Air Stair operations—one of them in June 2017, the other 2 in September 2017.
The transmission line work being performed in the Tweed area, which had started in September 2017, was the PLTs' first operational experience involving aerial transfer with the Air Stair. However, aerial transfers were not taking place on the day of the occurrence.
| Power line technician 1 | Power line technician 2 | Power line technician 3 | |
|---|---|---|---|
| Accreditation | Journeyperson | Journeyperson | Apprentice level 3* |
| Hours on duty prior to the occurrence | 4.5 | 4.5 | 4.5 |
| Hours off duty prior to the work period | 14 | 14 | 14 |
* The apprenticeship program consists of 4 levels, each of which takes 2000 hours to complete. Level 4 is the highest level. It takes approximately 4 years to complete the entire program. Apprentices who complete the program are eligible to achieve journeyperson certification as a power line technician.
1.5.2.1 Training
Hydro One's course on how to access transmission line structures from the helicopter's Air StairFootnote 8 consists of 8 modules that cover several topics related to the safe use of an Air Stair. The training is divided into a 2-hour classroom portion and a 6-hour field-training portion, at the end of which each PLT must complete a skills assessment. The training for aerial transfers generally consists of the procedures PLTs are to use when transferring to and from the helicopter to transmission poles or towers.
According to the training documents, when PLTs board the helicopter, they are to attach the nose bags to the Air Stair handrail and secure the preform bags to the cabin floor.Footnote 9 There is no similar guidance stating what to do with these bags when boarding the helicopter from the ground. The investigation found that when boarding from the ground, there were various practices relating to the storage and securement of the preform bags.
1.5.2.2 Equipment
To complete their work on the transmission towers, PLTs are required to wear personal protective equipment, including a full body harness with a travel restrict system (also referred to as a fall restrict tether), and clothing approved and adapted for the weather conditions at the time the work is being carried out.
On the day of the occurrence, the PLTs were wearing bulky winter clothing and would have worn their full body harness with a travel restrict system while working on the tower. However, during the return flight to the staging area, the full body harnesses with the travel restrict systems were no longer required, and the PLTs had removed them. The investigation could not determine exactly when the PLTs removed their full body harnesses.
1.6 Aircraft information
| Manufacturer | Airbus Helicopters |
|---|---|
| Type, model and registration | AS 350 B2, C-GOHS |
| Year of manufacture | 1999 |
| Serial number | 3240 |
| Certificate of airworthiness/flight permit issue date | 05 January 2000 |
| Total airframe time | 10130 |
| Engine type (number of engines) | Turboshaft (1) |
| Propeller/Rotor type (number of propellers) | Starflex Semi-rigid (3 blades) |
| Maximum allowable takeoff weight | 2250 kg |
| Recommended fuel type(s) | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A |
1.6.1 General
The AS 350 B2 is a light single-engine utility helicopter originally designed and manufactured in France by Aérospatiale in the 1970s. In January 1992, Aérospatiale merged with Daimler-Benz Aerospace AG to form Eurocopter, which later became part of Airbus. In January 2014, Airbus rebranded Eurocopter as Airbus Helicopters.
Records indicate that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. The weight and centre of gravity were within the limits prescribed by the manufacturer at the time of the occurrence.
1.6.2 Air Stair
The helicopter was equipped with a platform (known as an Air Stair) to allow PLTs to get onto and off transmission towers and poles while the helicopter is in flight, hovering next to the tower or pole.
The Air Stair mounts to the underside of the fuselage but does not extend below the skid gear (Figure 3). When the Air Stair is installed, the helicopter's front left seat is replaced with a box that the PLTs use to stow equipment, and the floor of the helicopter is fitted with anchor points where the PLTs can attach their fall restrict tethers when they are ready to transfer.

1.6.2.1 Air Stair supplemental type certificate
All commercially operated aircraft must hold a type certificate that certifies that the aircraft's design complies with the regulatory requirements. When operational equipment is going to be installed on an aircraft and the equipment was not designed by the company that holds the type certificate, a supplemental type certificate (STC) is required.
Hydro One hired JCM Aerodesign Limited to design the Air Stair. Transport Canada (TC) approved STC SH01-62 on 22 November 2001.
The STC was issued with several limitations, including the following:
Rotorcraft incorporating this modification must be operated in accordance with the Flight Manual Supplement […]
Use of this installation for the purpose of in-flight embarkation and / or disembarkation requires separate Transport Canada operational approval.Footnote 10
1.6.2.1.1 Flight manual supplement and maintenance manual supplement
As required by regulation, the designer of the Air Stair published a flight manual supplement (FMS) and a maintenance manual supplement (MMS). The STC holder (i.e., the operator) was required to keep the manuals up to date.
An FMS informs flight crews of any changes with respect to the aircraft's limitations, normal and emergency procedures, and performance described in the aircraft flight manual. The FMS must be included with the aircraft flight manual, which is available to flight crews.
An MMS contains information related to the maintenance and installation of equipment. It is generally not easily accessible by flight crews.
The Air Stair was modified in 2007 to allow for the addition of a removable seat and tool tray on the Air Stair itself, so that a PLT could work from the platform without having to get off it. JCM Aerodesign Limited amended the MMS to reflect these changes; however, although the FMS was also amended at the same time, it did not include information on the addition of the seat and tool tray.
The amendments to the manuals were approved by TC. However, there were several inconsistencies between the 2 manuals that were not identified during the approval process. For example, the required instrument panel placard published in the FMS differed from that published in the MMS (Table 5).
The investigation noted that the occurrence helicopter's instrument panel was not placarded as required following the modifications made in 2007.
| Placard information in the flight manual supplement* | Placard information in the maintenance manual supplement** |
|---|---|
“WITH AIR STAIR INSTALLED |
“WHEN AIR STAIR INSTALLED |
- * JCM Aerodesign Limited, Flight Manual Supplement No. 003063FMS (TC approved 27 September 2007), p. 4.
- ** JCM Aerodesign Limited, Maintenance Manual Supplement No. 003063MMS (TC accepted 28 September 2007), p. 7.
See Appendix A for a complete list of differences between the FMS and the MMS.
1.6.2.2 Operations specifications
In addition to STCs, depending on how the operational equipment will be used, the air operator may be required to have operational approval from TC in the form of an operations specification (OPS Spec) to its air operator certificate.
Given the type of work being carried out by Hydro One using the Air Stair, the company was required to have 2 separate OPS Specs.
OPS Spec 044—Entering or Leaving a Helicopter in Flight was required to allow PLTs to enter or leave the helicopter during airborne operations (using the Air Stair). This OPS Spec was requested by the operator and approved by TC.
OPS Spec 047—Helicopter – CAR 702.21(2)(a) Class D External LoadFootnote 11wasrequired to allow PLTs to perform work while occupying the Air Stair during airborne operations.
In August 2001, Hydro One recorded that it communicated with TC regarding this authorization and received a verbal opinion that this type of work would be covered under Class A external loads and, therefore, it would not require OPS Spec 047. However, TC did not have any record of such communication. TC indicated that it may have verbally stated that Hydro One did not need OPS Spec 047, as it believed Hydro One was using the Air Stair only for embarkation and disembarkation, in accordance with the STC.
Following the occurrence, TC reported that it was not aware that Hydro One had been using the Air Stair for purposes that would have required a Class D external load authorization (OPS Spec 047), for which Hydro One did not have TC approval.
1.6.2.3 Transporting equipment and tools during Air Stair operations
In order to carry out their work, PLTs must bring a number of hand tools with them to the top of the transmission towers. When accessing the towers from the ground, they usually work in teams of 3; with 2 PLTs carrying out the work on the tower and the 3rd staying on the ground and acting as a support person.
When the Air Stair is being used for aerial transfers, PLTs are able to embark and disembark the helicopter at the top of the transmission tower or pole. This means that the PLTs can work in teams of 2 instead of 3 because there is no need for a support person on the ground.
During ground-based operations, the PLT who stays on the ground uses a pulley system to transfer the tools and equipment to the top of the tower. During aerial transfers, the equipment and tools are transported to the top of the tower in the helicopter along with the 2 PLTs. The tools and equipment cannot be carried in the helicopter's normal exterior baggage compartments because these compartments are not accessible while airborne. To facilitate aerial transfer of the items to and from the helicopter, they are attached to the Air Stair by a carabiner.
When equipment is carried outside an aircraft's cabin or outside a compartment intended for such use, the Canadian Aviation Regulations (CARs) stipulate that
No air operator shall operate an aircraft carrying an external load unless the attachment device is authorized in a supplemental type certificate or in an airworthiness approval relating to the operational configuration of the aircraft.Footnote 12
The Air Stair was a modification to the helicopter and approved in accordance with an STC; therefore, it was not considered an external load. However, neither the original FMS issued in 2001 nor the amended version in 2007 stated whether it was permitted to have an object, such as equipment and tool bags, attached to the Air Stair when the helicopter was in flight. Any such object would be considered an external load.Footnote 13
The FMS states that “[t]he Air Stair is intended for, but not restricted to, providing aerial access to Hydro towers to qualified linemen.”Footnote 14 Because PLTs stow their tools in the external tool tray when performing work directly from the Air Stair, and connect the various equipment and tool bags to the Air Stair during transfers to and from towers, Hydro One interpreted this statement in the FMS to mean that an object could be attached to the Air Stair while the helicopter was in flight.
1.7 Meteorological information
The nearest weather reporting stations to the accident site were Canadian Forces Base Trenton, Ontario, (31 NM south-southwest of the accident site) and Kingston Airport, Ontario (35 NM southeast of the accident site).
The aerodrome routine meteorological report (METAR) issued at 1200 for Trenton indicated the following:
- winds: 280° true at 12 knots
- visibility: 15 statute miles (SM)
- clear sky
- temperature: −14.5 °C, dew point −22.3 °C
The METAR issued at 1200 for Kingston indicated the following:
- winds: 270° true at 9 knots
- visibility: 15 SM
- few clouds at 2000 feet
- temperature: −15 °C, dew point −22 °C
The graphic area forecast showed a possibility of few clouds between 3000 feet and 5000 feet, a visibility greater than 6 SM, and no significant weather.
1.7.1 Cold temperatures
At the time of the accident, the temperature was approximately −15 °C. However, on the morning of the accident, the wind chill values reported at Trenton and Kingston airports ranged from −28.4 to −23.3. Given the cold temperature, the Air Stair was not being used for the operation, and the PLTs had to climb the towers to perform their tasks. The PLTs had been working in these cold temperatures for approximately 2 hours just before boarding the helicopter.
It is well known that cold temperatures affect physical performance, including fine motor skills such as those needed for piloting or for manipulating tools to do a repair. Tasks performed by both the pilot and the PLTs also require constant vigilance and concentration to mitigate the risks associated with their respective tasks.
Cold weather can also have a negative effect on cognitive function. Several studies have shown that cold temperatures can impair cognitive performance, such as vigilance,Footnote 15 memory,Footnote 16 reaction time,Footnote 17 and decision making.Footnote 18 Consistent findings on performance decrements may be explained by the distraction theory advanced by Teichner.Footnote 19 According to this theory, cold stress is believed to cause a shift in attention from the cognitive task, resulting in performance decrements. In other words, attention is focused on feeling cold rather than accomplishing the task effectively. This theory is supported by recent findingsFootnote 20 of an experimental study in which temperatures as mild as 10 °C may have provided enough of a sensory challenge to distract participants from a set of tasks. In that study, reaction time, working memory, and executive function declined during participants' exposure to cold, and these impairments persisted 60 minutes into the recovery period after being warmed.
A study carried out in FinlandFootnote 21 demonstrated that, compared to complex tasks, simple tasks are usually performed faster but less accurately under cold conditions. A possible explanation for this performance decrement is that because the assessed tasks do not require as much attention as complex tasks do, the cold may be acting as a distraction.
Notwithstanding the fact that the temperatures were cold that day, there is no evidence that the pilot was negatively impacted during the brief period of time that the cabin door was open when the PLTs boarded or exited the helicopter.
1.8 Aids to navigation
Not applicable.
1.9 Communications
Not applicable.
1.10 Aerodrome information
Not applicable.
1.11 Flight recorders
The helicopter was not equipped with, nor was it required to carry, a cockpit voice recorder or a flight data recorder. However, data was successfully extracted from an on-board global positioning system (GPS) and a global satellite transceiver.
1.12 Wreckage and impact information
1.12.1 General
The helicopter crashed in a forested area approximately 400 feet northwest of the intended landing site (Figure 4). The tail rotor gearbox was found 67 feet north-northwest of the main wreckage site with the tail rotor blades attached, and the vertical fin was found 144 feet southwest of the main accident site with the end of the tail boom still attached.
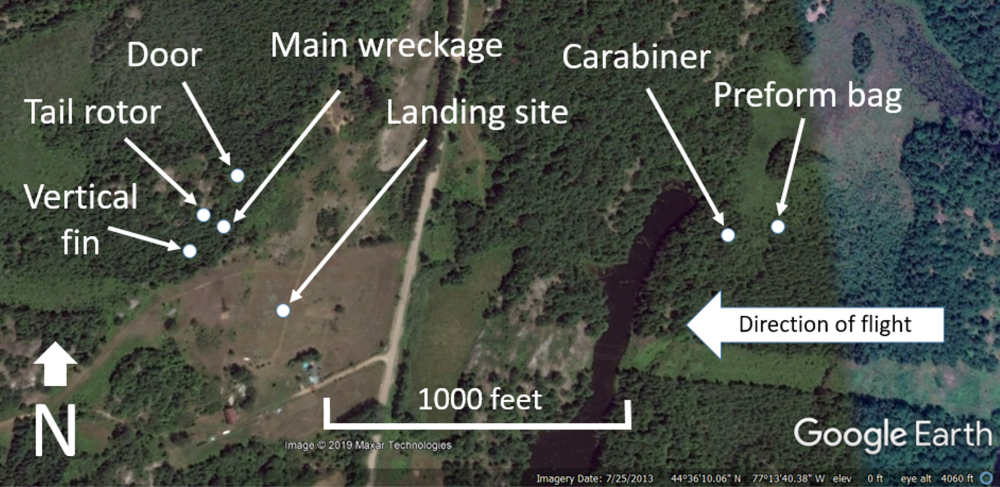
A broken carabiner with part of a preform bag attached was found about 1900 feet east of the accident site. The rest of the preform bag was found about 310 feet further to the east.
One tail rotor blade was missing approximately 10.75 inches of the outer portion, including the blade balance weights. Although most of the outer portion of the blade was recovered, the tip and balance weights were not. There were signs of damage, likely caused by the carabiner striking it, on the leading edge of the tail rotor blade where the outer portion of the blade had fractured.
The right main-cabin door was found 180 feet north of the main wreckage site and the canopy was found 40 feet north-northeast of the main wreckage site. The rest of the helicopter was contained within the impact site, and damage was consistent with a steep vertical descent.
The helicopter struck the ground on its left side in a slightly nose-down attitude and came to rest with its nose oriented to the south. The occupiable space of the passenger compartment and the cockpit area were not compromised.
It was determined that the engine was running at impact. No anomalies were identified with the engine control system that would have precluded normal control of the engine. The flight control system was intact, and no anomalies were identified that would have precluded normal operation of any of the control axes.
The main fuel tank, which was made of plastic and located beneath the engine/transmission bay deck and behind the passenger compartment, had fractured into several large pieces. No fuel remained in the tank. There was a fuel spill in and around the accident site.
All 3 main-rotor blades struck trees and the ground and were heavily damaged. The main rotor head was severely damaged; however, each of the 3 main-rotor blades remained in its respective hub and control connections were maintained. The tail boom had partially separated on the right side, near the attachment to the rear structure.
The Air Stair handrails showed no signs of pre-impact damage that would have allowed attached carabiners to come loose during flight.
1.12.2 Tool bags
1.12.2.1 Preform bag
The preform bag, which was used to carry line maintenance supplies, was approximately 43 inches long, tube-shaped and made of a light canvas-type material. The bottom of the bag was made of black plastic, and the top and bottom edges of the bag were reinforced with leather (Figure 5). The top of the bag had 2 loops made of a polypropylene-type rope attached to each side of the bag as handles. One of the loops had detached from the bag and was missing.

Attached to the rope handles of the preform bag was a large carabiner, approximately 8.5 inches long, that was designed to have a large load-carrying capability. All that remained of the carabiner was the frame; the top portion was bent, and the gate, which had a twist-lock-type locking sleeve, was fractured and missing (Figure 6).

1.12.2.2 Nose bags
Two nose bags were found at the accident site. One was attached to the handrail of the Air Stair with a large carabiner (Figure 7) and was fully intact. The other was heavily damaged and located among the debris at the accident site (Figure 8). This bag had torn from its associated carabiner, which was still attached to the handrail of the Air Stair.


1.13 Medical and pathological information
The investigation did not identify anything to indicate that the pilot's or the PLTs' performance was degraded by fatigue or medical factors.
1.14 Fire
Not applicable.
1.15 Survival aspects
1.15.1 Seat and safety belts
The pilot's seat was adjustable fore and aft, and equipped with a 4-point safety belt consisting of a lap strap and an automatic locking (inertia reel) shoulder harness. The pilot's seat attachment to the airframe was found to have failed laterally, and the right lap strap had pulled partially through the fibreglass seat pan. This is consistent with the left-side impact when the helicopter collided with terrain.
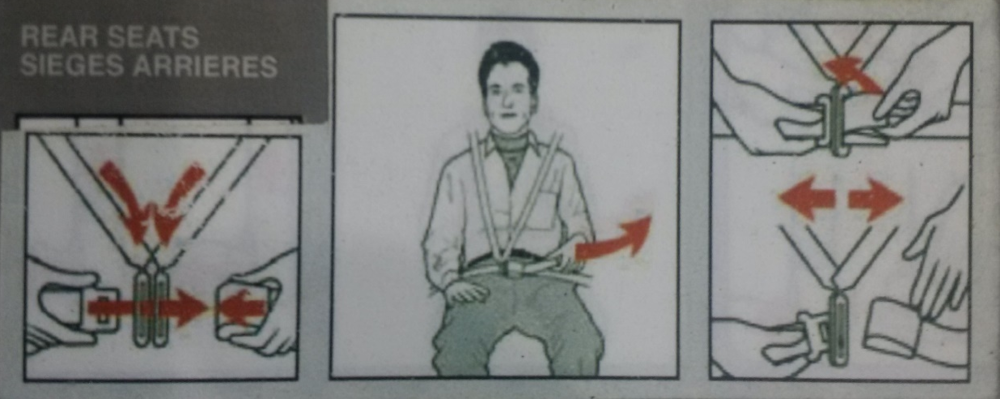
The helicopter had a 4-seat fixed-position rear bench, which was normally equipped with a 4-point safety belt for each seat. These safety belts were designed so that one half of the lap strap buckle had to be inserted through metal tongues on the shoulder harness before connecting the second half of the lap strap buckle (Figure 9). Lifting the buckle latch simultaneously released the lap strap and both shoulder harness straps. It was possible to wear the lap strap portion only, without the automatic locking shoulder harness attached.
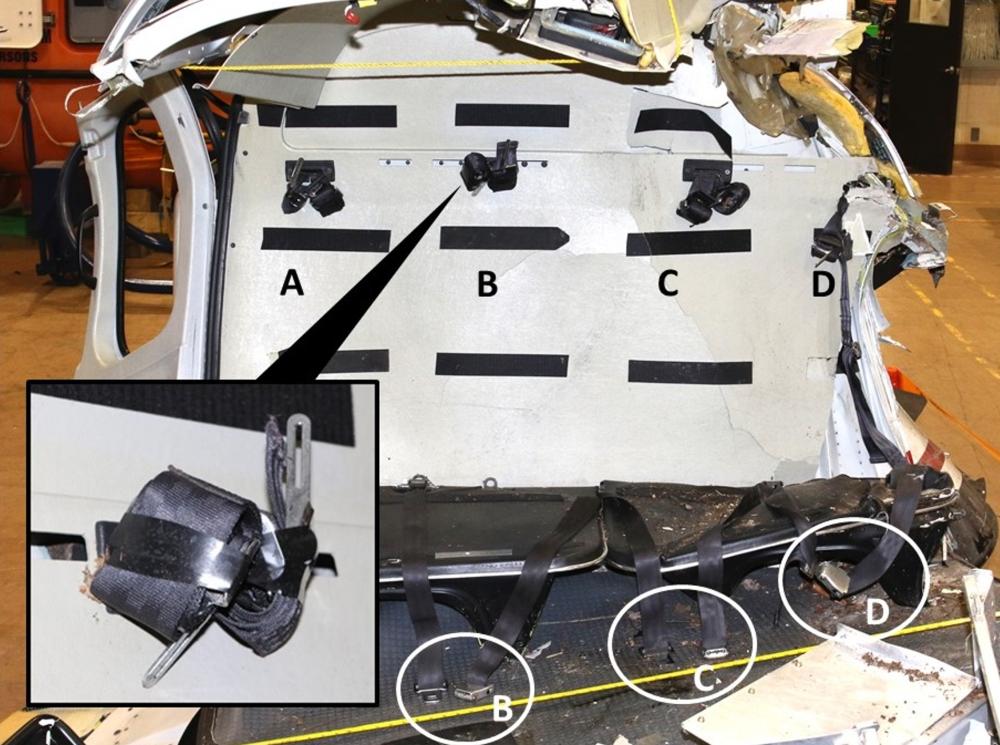
Following the accident, the entire rear bench safety belt system (Figure 10) was examined at the TSB Engineering Laboratory in Ottawa, Ontario, and the following was noted:
- The lap strap at seat A had been removed by Hydro One for operational reasons.
- The straps, buckles, and latches of the other 3 lap straps (seats B, C, and D) were in good condition.
- The lap straps at seats B and C were unlatched and adjusted to full length.
- The buckle of the lap strap at seat D was fastened and adjusted to approximately 80% of its full length.
- There were no signs that the lap strap buckle assemblies at seats B and C had been forced apart.
- The shoulder harnesses at all seats were rolled up and taped with black electrical tape in their retracted positions, which rendered them inaccessible.
1.15.1.1 Regulatory requirements
The CARs contain several requirements for aircraft to be equipped with safety belts, restraint systems, and shoulder harnesses. More specifically, the CARs stipulate the following with respect to the requirement for seats and safety belts:
605.22 (1) Subject to subsection 605.23, no person shall operate an aircraft other than a balloon unless it is equipped with a seat and safety belt for each person on board the aircraft other than an infant […]Footnote 22
605.23 An aircraft may be operated without being equipped in accordance with section 605.22 in respect of the following persons if a restraint system that is secured to the primary structure of the aircraft is provided for each person who is
- carried on a stretcher or in an incubator or other similar device;
- carried for the purpose of parachuting from the aircraft; or
- required to work in the vicinity of an opening in the aircraft structure.Footnote 23
The CARs require helicopters to be equipped with shoulder harnesses as follows:
605.24 (4) No person shall operate a helicopter manufactured after September 16, 1992, the initial type certificate of which specifies that the helicopter is certified as belonging to the normal or transport category, unless each seat is equipped with a safety belt that includes a shoulder harness […]Footnote 24
With respect to the general use of safety belts and restraint systems, the CARs state:
605.25 (1) The pilot-in-command of an aircraft shall direct all of the persons on board the aircraft to fasten safety belts
- during movement of the aircraft on the surface;
- during take-off and landing; and
- at any time during flight that the pilot-in-command considers it necessary that safety belts be fastened.
(2) The directions referred to in subsection (1) also apply to the use of the following restraint systems:
- a child restraint system;
- a restraint system used by a person who is engaged in parachute descents; and
- a restraint system used by a person when working in the vicinity of an opening in the aircraft structure […]Footnote 25
The CARs stipulate the following with respect to the use of passenger safety belts and restraint systems:
605.26 (1) Where the pilot-in-command or the in-charge flight attendant directs that safety belts be fastened, every passenger who is not an infant shall
- ensure that the passenger's safety belt or restraint system is properly adjusted and securely fastened […]Footnote 26
A safety belt is defined in the CARs as “a personal restraint system consisting of either [emphasis added] a lap strap or a lap strap combined with a shoulder harness.”Footnote 27 The CARs defines a shoulder harness as “any device that is used to restrain the upper torso of a person and that consists of a single diagonal upper torso strap or dual upper torso straps.”Footnote 28
Although the regulations are clear that all seats on the occurrence helicopter were required to be equipped with safety belts, including shoulder harnesses, the regulations are not clear with respect to when flight crews and passengers are required to use the equipped shoulder harness. However, according to correspondence received from TC, the intent of the regulations was for passengers to always use shoulder harnesses when they are available.
In contrast, a provision in the CARs for airline operators is clear and specific. It stipulates that flight crews are required to fasten their safety belts, including the shoulder harness, as indicated in subsection 705.29(1) of the CARs, which states the following:
Subject to subsection (2), flight crew members who are on flight deck duty shall remain at their duty stations with their safety belts fastened and, where the aircraft is below 10,000 feet ASL [above sea level], with their safety belts, including their shoulder harnesses [emphasis added], fastened.Footnote 29
1.15.1.2 Recent regulator guidance on the use of safety belts and shoulder harnesses
In November 2014, TC published a new issue of Advisory Circular 605-004: Use of Safety Belts and Shoulder Harnesses On Board Aircraft. The purpose of this advisory circular, which applies to all operators of Canadian-registered aircraft, is to “remind operators of the need to establish procedures regarding use of safety belts and shoulder harnesses on board aircraft and to inform air operators of the procedures for use of safety belts and shoulder harnesses recommended by [TC].”Footnote 30
The Advisory Circular defines a restraint system as
a general term for occupant safety systems such as a safety belt, shoulder harness, inflatable restraint system, child restraint system, or any other strap, webbing or similar device designed to secure a person in an aircraft.Footnote 31
With regard to safety belts specifically, the Advisory Circular states that
[t]he definition of “safety belt” recognizes that two configurations of personal restraint systems continue to exist on Canadian-registered aircraft; those fitted with only a lap strap, and those consisting of both a lap strap and shoulder harness. To provide for the safety of the user, where a shoulder harness is affixed to the aircraft, it should be worn.Footnote 32
In the Advisory Circular, the word “should,” with respect to use of shoulder harnesses, appears to be inconsistent with TC's stated intent for the regulations.
1.15.1.3 Hydro One safety belt procedures
Hydro One's Company Operations Manual (COM) uses the same safety belt definition as the CARs; however, the investigation determined that Hydro One understood the definition to mean that occupants had a choice between wearing the lap strap only or the lap strap combined with the shoulder harness.
The COM stipulates that “each passenger must occupy a seat equipped with a serviceable safety belt which shall be worn at all times while the aircraft is in flight including take off and landings.”Footnote 33 It also stipulates that the passenger briefing should include “how and when to use seat belts or safety harnesses.”Footnote 34
The COM also stipulates that “[b]efore take-off and landing, the PIC [pilot-in-command] shall visually check that all persons are seated and secured.”Footnote 35 However, when landing in remote areas or on land that has not been prepared for takeoff and landing, the surface is not always even and it may not be advisable for the pilot to completely shut down the engine. To accommodate for this, it is common practice for pilots to let PLTs embark or disembark while the engine is running.
When doing this, the pilot often needs to maintain balance of the helicopter while keeping it light on its skids. This task requires a high level of concentration, and any head movement toward the back while doing this could create a hazard. As a result, it is not always feasible for pilots to visually confirm that the PLTs have their safety belts secured during these types of embarkations.
In such situations, the standard visual-check procedure is often adapted; the investigation determined that it was common practice for one of the PLTs to give the pilot a physical thumbs-up signal on the pilot's left side to indicate that everyone was seated, secured, and ready for takeoff. The pilot had to rely on the PLTs to ensure that the safety belts were worn as prescribed in the tailboard meeting and as required by the COM.
1.15.1.4 Passenger behaviour and safety belt use
Lap straps and shoulder harnesses are called active safety systems because the user must perform certain actions, such as buckling the belt, in order to be protected.
The safety issue of passengers not wearing seat belts is not limited to aviation. For example, a survey published in 2018 by the U.S. Insurance Institute for Highway Safety found that almost a third of respondents reported being less likely to buckle up when they were sitting in the rear seat of a car.Footnote 36 Among these respondents, the majority said that short trips or travelling by taxi were times they did not fasten their seat belt. Passengers gave several reasons for not wearing a seat belt in the rear seat versus when they were sitting in the front. For example:
- Misperception of safety benefits: Passengers' subjective perception of the risk of injury and death influences their behaviour. Passengers will also accept more risk if there is a payoff: e.g., passengers are willing to take more risks when they are in a hurry. The optimism bias (‘'it can't happen to me'') and overestimating ability to avoid injury play major roles in such perceptions.
- Design and usability: Common design and usability issues with seat belts include difficulties reaching for and pulling the belt across the body, and inserting the latch into the buckle portion of the seat belt. Physical limitations from wearing winter clothing and gear may exacerbate these problems, making it difficult to locate the buckle and release the latch to unfasten the buckle.
- Lack of enforcement: Laws requiring the use of seat belts are in place to ensure the safety of passengers. However, if there is a perception that compliance with these laws is not enforced, passengers may be less likely wear a seat belt.
TSB investigations of small aircraft accidents in recent years have found that it is common for crew members and passengers to fasten the lap portion of their safety belts, but that shoulder harness use varies widely. Serious injuries and fatalities have occurred in accidents involving aircraft that were either not equipped with shoulder harnesses, or that were equipped with shoulder harnesses but the harnesses were not worn.
A search of the TSB database from 1990 to 2018 found 62 accidents in which shoulder harnesses were available but were not worn. Of those accidents, 33 involved fatalities, resulting in 68 deaths. Of those deaths, 37 involved individuals who had not been wearing available shoulder harnesses (Appendix B). Although the survivability of these accidents varied, the use of shoulder harnesses in many cases could have improved the odds of survival and egress.
1.15.1.5 Safety belt use and Air Stair operations
Air operations involving the Air Stair must comply with the FMS, which states, “Except when disembarking from the aircraft all personnel must be secured to the airframe either by a safety belt, or by a fall restrict tether.”Footnote 37 However, the restraint system mentioned in paragraph 605.25(2)(c) of the CARs, which includes the fall restrict tether, applies only when a person is working near an opening in the aircraft structure, and not when the person is being transported from one place to another. In all cases involving transportation, a safety belt is required.
The procedure documentFootnote 38 for aerial operations involving the Air Stair does not clearly indicate when PLTs are required to attach or detach the safety belt at each step. However, it does state the following:
A full body harness and a travel restrict system is used as fall protection by workers for access to/from the AirStair/cabin of the helicopter and while working from the AirStair.Footnote 39
The investigation found that there was a perception among the PLTs who had been trained to carry out air operations with the Air Stair that if they attached their personal protective equipment—full body harness and travel restrict system—to an anchor point on the floor, it would be enough to ensure their safety while in flight or in an emergency. This perception led to the belief that it was not necessary to wear the safety belt if personal protective equipment was being worn and attached to the floor. During the occurrence flight, the perception did not apply, because the PLTs were not wearing their full body harnesses.
The investigation also found that the use of the full body harness could create a new risk. When the PLTs moved from the cabin to the platform during an aerial transfer, the shoulder harness straps would sometimes get caught in a ring at the back of the full body harness. This could cause the PLTs to lose their balance, leading to a risk of their falling onto the platform or disturbing the pilot, in turn potentially causing the helicopter to move and collide with the tower. To eliminate this risk, the shoulder harnesses were often rolled up and taped with electrical tape when operations involving aerial transfers were being carried out.
On the occurrence flight, there was no plan to perform aerial transfers. Instead, the plan was to have the PLTs embark and disembark at the bottom of a structure while the helicopter was still running. Hydro One does not have step-by-step standard procedures for the pilot and the PLTs to follow in this situation. The fact that the shoulder harnesses were rolled up and taped was not consistent with this type of flight.
1.15.2 Impact forces
The Analysis of Rotorcraft Crash Dynamics for Development of Improved Crashworthiness Design Criteria published by the U.S. Federal Aviation Administration (FAA) states the following with respect to human tolerance to a crash environment:
Generally three classes of injuries are considered when discussing human tolerance in a crash environment: internal injuries due to whole-body deceleration, secondary impact injuries due to contact with surrounding structure, and fire-related injuries due to thermal exposure or inhalation of combustion products. The first two classes are directly related to the principal impact forces […].Footnote 40
The survivability of the principal impact depends on the individual's whole-body acceleration tolerance, which may vary from one person to another.
In helicopter accidents, approximately 70% of all serious and fatal injuries occur primarily in the head, spine, torso, and neck regions. Shoulder harnesses are particularly effective at limiting injury to these areas. The FAA's analysis of crash dynamics showed that, of the people who experienced a helicopter crash, only 9% of those who were wearing a shoulder harness had severe injuries, compared with 34.3% of those who wore just a lap strap.Footnote 41
Shoulder harnesses could help prevent flailing injuries, but in the case of a high-g-forceFootnote 42 lateral impact, they would not prevent a person from receiving internal injuries. When compared to not wearing a safety belt or wearing only a lap strap, wearing both a lap strap and a shoulder harness will increase the probability of remaining inside the helicopter and decrease the probability of receiving secondary flailing-related injuries.
In this accident, the helicopter was not equipped with on-board recorders capable of recording the impact forces (g). As a result, the exact direction, duration, and loading of the g forces sustained by the helicopter and its occupants at impact could not be determined. However, the investigation calculated that the impact load on the helicopter as a whole was at least 77g. This force is greater than the lateral tolerance levelsFootnote 43 of the human body; however, the deceleration forces experienced by occupants are usually lower than those sustained by a helicopter because the helicopter structure absorbs energy during the impact sequence.
1.15.3 Helmet
The occurrence pilot was wearing a helmet, which came off at impact and was found damaged a few feet away from him. The investigation could not determine why the helmet came off.
There are no requirements in the CARs for helicopter pilots to wear a protective helmet; however, the Aviation Occupational Health and Safety Regulations do require protective headgear to be worn if there is a risk of head injury.Footnote 44 Hydro One requires pilots to wear a helmet when performing Air Stair operations.Footnote 45
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP018/2018 – Estimation of Impact Loads
- LP139/2018 – Lap BeltsFootnote 46 Examination
- LP225/2018 – Wreckage Examination
1.17 Organizational and management information
1.17.1 General
In 1999, Ontario Hydro, a Crown corporation, was restructured into 4 separate entities, including Ontario Hydro Services Company Inc., which was a holding company with subsidiaries. In 2000, Ontario Hydro Services Company Inc. was renamed Hydro One Inc. One of the subsidiaries of Hydro One Inc. is Hydro One Networks Inc., the company involved in this occurrence. In November 2015, the Government of Ontario began to sell shares to the public to privatize Hydro One Inc.
Hydro One Networks Inc. is the largest electricity transmission and distribution service provider in OntarioFootnote 47. The company operates through 3 business segments: transmission, distribution, and other. The transmission segment owns, operates, and maintains its transmission system (high-voltage electricity from nuclear, hydroelectric, natural gas, wind, and solar power sources). The distribution segment consists of approximately 123 000 circuit kilometres of primary low-voltage transmission lines, which are operated by its subsidiaries. The other segment represents its telecommunications business and certain corporate activities.
Both the transmission business and the distribution business are operated mainly by Hydro One Networks Inc., which allows the 2 businesses to use common technology, equipment, and field staff, and to benefit from the resulting operating efficiencies and increased effectiveness.Footnote 48
1.17.2 Air operator
Ontario Hydro, the predecessor of Hydro One Networks Inc., began chartering or operating helicopters in early 1949. Hydro One Networks Inc. currently holds an air operator certificate to operate AS 350 B2/B3 and AS 355 NP helicopters in accordance with subparts 702 (aerial work) and 703 (air taxi operations) of the CARs.
According to the Canadian Civil Aircraft Register, Hydro One Networks Inc. operates a fleet of 8 helicopters: 7 of them are AS 350 B2/B3s and 1 is an AS 355 NP.
Hydro One Networks Inc. has a Health, Safety and Environment Management System that encompasses all its lines of business. It does not currently have an aviation safety management system, nor is one required by regulation.
1.17.3 Tailboard meetings
Standard operating procedures for employees are found in the Hydro One Document System (HODS). This corporate database provides detailed work procedures for all normal and specialized operations.
As part of Hydro One's Health, Safety and Environment Management System, a safety representative had observed the tailboard meeting between the pilot and the PLTs on the morning of the occurrence. The tailboard meeting was documented on a site visit form, and included the observer's comments regarding the briefing. These comments indicated that before boarding, the pilot:
- gave a thorough and detailed tailboard;
- explained and demonstrated the proper procedure of approaching and leaving the helicopter;
- demonstrated the proper storage of the tools, hardware and equipment;
- demonstrated how the first crew member holds the door open while the other crew members unload their tools and equipment onto the ground and safely move away from the helicopter;
- cautioned them regarding the hazards of going near the back of the helicopter;
- reviewed the proper use of the seatbelts and prepared them for use.Footnote 49
It was reported that, during the tailboard meeting, the pilot had instructed the PLTs to collapse the preform bag, place it inside the nose bag and store the nose bag in the cabin under the rear seat when their work had been completed. However, this information was not documented on the site visit form or elsewhere.
The investigation was unable to determine if the preform bag had been placed inside the nose bag, if it had been left on the Air Stair, or if it had fallen onto the Air Stair when the PLTs boarded the helicopter.
1.17.4 Mitigation of hazards created by loose objects
Procedures for air operations using the Air Stair are included in the HODS. A review of these procedures determined that there were significant gaps with respect to guidance on what can and cannot be attached to the Air Stair and what can be transported in the nose bag during flight.
The investigation found that some HODS documentsFootnote 50 include an appendix that contains a list of work steps, their associated hazards, and proposed ways to mitigate those hazards (referred to in these documents as “barriers”). However, the possibility of an object falling out of a nose bag during the flight to and from the tower was not identified as a hazard; therefore, the company had not established a barrier to mitigate that risk. In addition, the HODS documents do not mention what can and cannot be put inside the nose bag or what is and is not permitted to hang on the cross-rail.
The Hydro One Networks Inc. Air Stair tailboard meeting checklistFootnote 51 includes only 3 items that refer to the transportation of tools and equipment on the cross-rail, as follows:
- Equipment Check:
- Item 11: “Put all PLT tools from belt into nose bag.”Footnote 52
- Air Stair Standard Briefing:
- Item 3: “Bonds – park on horizontal cross-rail with safety clip.”Footnote 53
- Item 4: “Nose bags and equipment on the aft cross-rail (100lbs max).”Footnote 54
1.18 Additional information
In 2017 and 2018, 2 occurrences, involving other operators, were reported to the TSB involving improperly secured objects striking the tail rotor of a helicopter in flight.Footnote 55 In both cases, the damage to the tail rotor was minor and the pilot was able to land the helicopter. The tail rotor did not break off in either case.
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
2.1 General
The events that led to this accident began as the helicopter picked up 3 power line technicians (PLTs) at the base of a power transmission tower and departed for a nearby staging area. En route, a preform bag with an attached carabiner blew off and struck the tail rotor. The analysis will focus on understanding why the external load was not adequately secured, why the passengers’ lap straps and shoulder harnesses were unfastened, and why these hazards were not recognized or mitigated before departure.
2.2 External loads
On the occurrence flight, several items—including a large pulley and 3 separate bags (2 nose bags and 1 preform bag) each with a carabiner attached—were on the Air Stair. The pulley and 2 nose bags were attached to the Air Stair with their associated carabiners. It could not be determined with certainty how the preform bag was stowed before departure. It may have been placed inside another bag, attached to the helicopter incorrectly, or not attached at all.
During the flight, a preform bag with an attached carabiner that had been on the Air Stair struck the helicopter's tail rotor, causing significant damage, severe imbalance, and intense vibration. There was no damage to the Air Stair that would have allowed an attached carabiner to become loose and, given the post-impact condition and load-carrying capability of the carabiner, it is unlikely that the carabiner had failed.
As the pilot attempted to land the damaged helicopter near the staging area, the tail rotor assembly failed entirely and the helicopter entered an uncontrolled rotation. Shortly thereafter, the helicopter struck terrain and was destroyed.
2.2.1 Company policies, procedures, and practices
When the Air Stair was being used for aerial transfers, it was company practice to attach small external loads temporarily to the Air Stair during aerial transfer of personnel and equipment, while the helicopter hovered at the top of transmission towers. This practice is documented in company manuals and specifically outlined in training documents. However, there was no formal guidance prohibiting the carriage of small external loads during transit flights. As a result, it became common practice for PLTs to attach tool bags and other small external loads to the Air Stair for flights to and from work sites.
It was reported that, during the tailboard meeting, the pilot had instructed the PLTs to collapse the preform bag, place it inside the nose bag, and store it in the cabin under the rear seat when their work had been completed. However, these instructions were not found in any documentation.
Even though the practice of attaching tool bags as external loads was very common and was permitted by the operator, there were no written procedures or instructions with respect to what could be carried, how these loads needed to be safely secured for flights that would not be using the Air Stair, or how the pilot should verify that the loads were secured properly.
Because this practice was not formalized, adequate controls (e.g., standardized procedures, training, checklists, or peer checks) were not in place to ensure that objects were properly stored in or secured to the helicopter. In this occurrence, part of the external load was not adequately secured.
Formalized procedures, training, and controls to prevent slips of attention are particularly critical when PLTs are securing loads while the helicopter is light on its skids. In such cases, the pilot remains at the controls and cannot make the head movements required to confirm visually that all equipment is secure. On the occurrence flight, the pilot was likely unable to confirm that the load was stored inside the cabin because he was occupied with controlling the helicopter during the light-on-skids pickup and would have been unable to turn his head to see the entire Air Stair.
2.2.1.1 Cold weather
Cold weather decreases dexterity, vigilance, and concentration, which may lead to an increase in errors. Some tasks that are easy to complete in warmer weather may be more difficult in the cold. In this occurrence, the adverse effects of the cold may also have had an impact on the way in which the PLTs loaded their equipment.
If individuals working in cold temperatures are impaired by the cold, critical tasks may not be performed properly, which could increase the risk of injury to personnel and damage to equipment.
2.2.2 Operations specifications
Hydro One had approval to operate the Air Stair using OPS Spec 044—Entering or Leaving a Helicopter in Flight, which was necessary to allow PLTs to transfer from the helicopter to the towers to conduct work.
The company also routinely had PLTs perform work on towers directly from the Air Stair, although this type of work was not being performed on the day of the accident. However, to allow PLTs to perform work directly from the Air Stair, Hydro One required authorization from Transport Canada (TC) to operate with a helicopter Class D external load, which required Operations Specification (OPS Spec) 047—Helicopter – CAR 702.21(2)(a) Class D External Load to be added to its air operator certificate.
Hydro One recorded that it had been informed verbally by TC inspectors in August 2001 that this type of operation was covered under Class A, and therefore a Class D authorization was not required. As a result, no formal identification of the hazards associated with such operations had been evaluated by TC, nor had mitigation been put in place to address the potential risks of such operations. Although there may have been verbal communication between TC and Hydro One regarding OPS Spec 047, TC did not have a record of it.
If air operators do not request and TC does not provide formal approval to conduct activities for which an OPS Spec is required, there is a risk that hazards associated with these activities will not be identified and mitigated.
2.2.3 Other risks associated with Air Stair operations
The investigation found several inconsistencies between the flight manual supplement (FMS) and the maintenance manual supplement (MMS) after the latest amendment to the supplemental type certificate (STC), including flight restrictions that were to be placarded on the instrument panel.
This issue was not a factor on the occurrence flight, because the Air Stair was not being used in a manner that would be affected by the identified inconsistencies. However, if flight manuals are not kept up to date and flight crews are not aware of limitations resulting from STC amendments, there is a risk that such limitations will be exceeded, resulting in injury to personnel or damage to equipment.
2.3 Safety belts
There were 3 lap straps in the rear cabin; 2 were found undone and fully extended, and 1 was found fastened. All 3 of the shoulder harnesses were found rolled up and taped with electrical tape, and therefore were not accessible.
Wearing both a lap strap and a shoulder harness increases the chances of the occupant remaining inside the helicopter during an accident sequence and reduces the chances of secondary, flailing-related, injuries, in contrast to occupants who do not wear a safety belt or who wear only a lap strap.
In this occurrence, the 3 PLTs were unsecured and became separated from the helicopter either slightly before or during the impact, and received fatal injuries from contact with the helicopter or the surrounding terrain.
The actual forces sustained by the helicopter during the crash sequence could not be determined; however, calculations indicated that the lateral impact forces (g) on the helicopter were at least 77g at impact. The impact forces during the accident sequence were high and likely were not survivable.
However, passengers who are not adequately restrained during a survivable accident, particularly when the main passenger compartment remains relatively intact, are at greater risk of receiving serious or fatal injuries than passengers who are adequately restrained.
2.3.1 Lap strap use
A survey published in 2018 by the U.S. Insurance Institute for Highway Safety found that almost a third of respondents reported being less likely to buckle up when they were sitting in the rear seat of a car. Among those respondents, the majority said that short trips or travelling by taxi were times they did not fasten their seat belt. Passengers gave several reasons for not wearing a seat belt in these conditions, including the assessment of risk and difficulties using the seat belt. These same 2 factors may have influenced the PLT's decision to not use lap straps in this occurrence.
Passenger behaviour is also strongly influenced by the passenger's ability to assess risk. Passengers who have not been injured themselves, or have not known someone who has been injured because they were not wearing a seat belt, tend to underestimate the risk involved.
One way to modify a passenger's perception of hazards or risks is through training. Training promotes safe behaviour, warns passengers of the existence of hazards, and explains the possible consequences of not complying. PLTs do not receive specific training on the risks associated with not wearing the safety belt, including the shoulder harness, or the potential injuries that unrestrained occupants can cause to others if control of the helicopter is lost.
In this occurrence, the PLTs may not have attached their safety belts after boarding the helicopter because they perceived the risk on the short flight to be low, or because they had difficulty attaching the belts over their cold-weather gear.
The same factors that hindered the pilot's ability to verify the security of the external load also affected his ability to verify that the PLTs were properly secured. Hydro One has a procedure in place for PLTs seated in the rear to confirm that they are properly secured before departure by giving the pilot a thumbs-up signal. Because pilots may not be able to divert their focus long enough to visually confirm that the safety belts are being used, this signal is intended to let the pilot know that the passengers are secure and ready for departure.
Normally, pilots will not depart until they have received this thumbs-up signal. In this occurrence, given the pilot's level of the experience and the PLTs' recent training, it is likely that this signal was given before departure.
2.3.2 Shoulder harness usage
The occurrence helicopter was required by regulation to be equipped with safety belts that included shoulder harnesses at all seats. Accordingly, it was equipped with 4-point detachable safety belts consisting of a lap strap and automatic locking (inertia reel) shoulder harnesses in the rear cabin. However, the shoulder harnesses of these safety belts were rolled up and taped with electrical tape, which prevented them from being used.
There are many regulations that require flight crews to brief and direct passengers to wear their safety belts, and for passenger to follow these instructions. The Canadian Aviation Regulations (CARs) define a safety belt as “a personal restraint system consisting of either [emphasis added] a lap strap or a lap strap combined with a shoulder harness.” Based on the definition of “safety belt” in the CARs, Hydro One considered that it would be in compliance with the regulations if occupants wore either the lap strap, or the lap strap combined with the shoulder harnesses.
In addition, Hydro One manuals refer to the safety belt and shoulder harness separately. Referring to these items separately could contribute to or reinforce the interpretation that wearing the shoulder harness is optional, as it may appear separate and distinct from the mandatory safety belt.
Compared to the lap strap alone, the full safety belt with attached shoulder harnesses can be more difficult or inconvenient to use, especially when PLTs are wearing bulky clothing and frequently entering and exiting aircraft. The company also identified that there was a risk of PLTs snagging the shoulder harnesses during aerial transfers. For these reasons, it was decided that the lap strap alone would be sufficient in these conditions, and the harnesses could be rolled up and taped to mitigate the hazard.
In November 2014, TC published a new issue of Advisory Circular 605-004, Use of Safety Belts and Shoulder Harnesses On Board Aircraft, which provides information and guidance to operators regarding the use of safety belts and shoulder harnesses. According to TC, the intent of the regulation was for passengers to always use shoulder harnesses when they are available. Even though this may be the intent, if regulations are not clear in requiring the use of all available components of a safety belt, shoulder harnesses may not be used as intended, increasing the risk of injury or death.
The TSB has investigated many accidents involving aircraft that were equipped with detachable shoulder harnesses but the harnesses were not worn (Appendix B). Of the 62 accidents identified, 33 were fatal, resulting in 68 deaths. And of those 68 deaths, 37 were individuals who had not been wearing the available shoulder harnesses. Although the survivability of these 62 accidents varied, the use of shoulder harnesses in many cases could have improved the odds of survival and egress. The interpretation of the regulations is not the only reason for not wearing the shoulder harness in the cases examined; however, in this particular case, the ambiguity did affect the operator's use of shoulder harnesses.
3.0 Findings
3.1 Findings as to causes and contributing factors
- When the Air Stair was being used for aerial transfers, it was company practice to attach small external loads temporarily to the Air Stair during aerial transfer of personnel and equipment, while the helicopter hovered at the top of transmission towers.
- There was no formal guidance prohibiting the carriage of small external loads during flights that did not involve the Air Stair. As a result, it became common practice for power line technicians to attach tool bags and other small external loads to the Air Stair for flights to and from work sites.
- Because this practice was not formalized, adequate controls (e.g. standardized procedures, training, checklists, or peer checks) were not in place to ensure that objects were properly stored in or secured to the helicopter. In this occurrence, part of the external load was not adequately secured.
- The pilot was likely unable to confirm that the load was stored inside the cabin because he was occupied with controlling the helicopter during the light-on-skids pickup and would have been unable to turn his head to see the entire Air Stair.
- The power line technicians may not have attached their safety belts after boarding the helicopter because they perceived the risk on the short flight to be low, or because they had difficulty attaching the belts over their cold-weather gear.
- A preform bag and its attached carabiner that had been on the Air Stair struck the helicopter's tail rotor, causing significant damage, severe imbalance, and intense vibration.
- As the pilot attempted to land the damaged helicopter near the staging area, the tail rotor assembly failed entirely and the helicopter entered an uncontrolled rotation. Shortly thereafter, the helicopter struck terrain and was destroyed.
- The power line technicians were unsecured and became separated from the helicopter either slightly before or during the impact, and received fatal injuries from contact with the helicopter or the surrounding terrain.
3.2 Findings as to risk
- If air operators do not request and Transport Canada does not provide formal approval to conduct activities for which an operations specification is required, there is a risk that hazards associated with these activities may not be identified and mitigated.
- If flight manuals are not kept up to date and flight crews are not aware of limitations resulting from supplemental type certificate amendments, there is a risk that such limitations will be exceeded, resulting in injury to personnel or damage to equipment.
- If regulations are not clear in requiring the use of all available components of a safety belt, shoulder harnesses may not be used as intended, increasing the risk of injury or death.
- If individuals working in cold temperatures are impaired by the cold, critical tasks may not be performed properly, which could increase the risk of injury to personnel and damage to equipment.
- Passengers who are not adequately restrained during a survivable accident, particularly when the main passenger compartment remains relatively intact, are at greater risk of receiving serious or fatal injuries than passengers who are adequately restrained.
4.0 Safety action
4.1 Safety action taken
4.1.1 Transportation Safety Board of Canada
On 21 December 2017, the TSB issued Aviation Safety Advisory A17O0264-D1-A1 to alert organizations to the risks associated with unsecured cargo and unrestrained passengers in helicopters. The advisory included the 2 following safety messages:
Cargo must be adequately secured at all times to prevent it from shifting or departing the helicopter during flight.
and
Passengers who do not wear seat belts risk serious injury or death in the event of an emergency.
4.1.2 Transport Canada
Transport Canada (TC) published Aviation Safety Letter (ASL) 1/2018, in which an article from ASL 4/2013 was republished. The article highlighted the importance of pilots wearing both the lap strap and shoulder harness portion of the safety belt, and explained that the intent of section 101.01 of the Canadian Aviation Regulations (CARs), is that pilots wear both the lap strap and shoulder harness where installed.
On 14 March 2018, TC issued Civil Aviation Safety Alert (CASA) No. 2018-02, “to remind all operators on the correct usage of passenger seatbelts and importance of securing cargo.”Footnote 56 The CASA included the following recommended action:
In accordance with the above mentioned CAR's, [sic] operators are reminded of the requirement and importance of securing all cargo and baggage. As well, it is the pilot's responsibility to ensure all passengers are briefed on the proper use of seatbelts. As seen in this accident it is extremely important for these actions to be carried out.Footnote 57
4.1.3 Hydro One Networks Inc.
Hydro One Networks Inc. has taken the following corrective actions:
- It has suspended operations involving the Air Stair.
- It has completed a comprehensive review and revision of the Helicopter Services Operations Manual to include enhancements to training program requirements, revised job descriptions and documentation procedures.
- It has received approval from Transport Canada Civil Aviation for the new Company Operations Manual.
- It has reviewed, restructured, and reassigned multiple Hydro One Document System documents, which have been further developed into Aviation Standard Operating Procedures.
- It has expanded the Flying in the Wire Environment training beyond Hydro One aircrew and aircraft maintenance engineers to over 100 line managers, field supervisors, and contractor helicopter pilots.
- It has had all flight crew complete crew resource management (CRM) training in anticipation of the training being required under the CARs, as detailed in TC Advisory Circular No. 700-042 (Crew Resources [sic] Management).
- It has developed the training for essential persons assigned on-board duties within the CRM training module.
- It has developed and delivered a restructured training program and flight following protocol for all company flight followers.
- It has begun investigating the introduction of simulator training (Level 7 flight training device or Level D full flight simulator) to enhance emergency procedures training for all pilots.
- It has completed the reorganization of the helicopter services operation, creating a separate line of business with a director reporting to the vice president, Shared Services, and a full-time dedicated aviation safety manager.
- It has recruited a Director of Helicopter Services to develop and implement business objectives and long-term department strategy.
- It has recruited a Manager of Aviation Safety to support the development and implementation of a safety management system (SMS).
- It has engaged an independent design approval representative to review all aspects of the certification of the Air Stair, including the relevant Flight Manual Supplements.
- It has conducted comprehensive audits of all third-party helicopter contractors to ensure alignment with Hydro One expectations.
- It has completed a macro-level assessment of all flight risks common to specialized tasks conducted by Helicopter Services.
- It has repositioned Helicopter Services as a stand-alone business unit within Shared Services to improve corporate communication and integration.
- It has added the position of Fleet Analyst to support business and corporate administrative activities.
- It has added the position of Operations Coordinator to support safe and efficient job planning and line of business integration.
- It has added the term position of Occupational Health and Safety Coordinator to support the Helicopter Services safety program.
- It has implemented a tablet-based electronic flight bag program to facilitate flight crew access to current policies and procedures and reference documents in the field, detailed aircraft performance and flight planning information and real-time weather information in flight.
- It has carried out an updated training program for Distribution Operations Management Centre personnel assigned flight following duties.
- It has evaluated equipment to support the phased implementation of a flight data management program for gathering flight operations data to support proactive SMS activity.
- It has communicated with all operations employees to reinforce current work procedures, including the fact that everyone inside the helicopter is to wear a seatbelt, including a shoulder harness (when provided).
4.2 Safety action required
4.2.1 Definition of “safety belt”
All of the rear bench seats in the occurrence helicopter were equipped with 4-point detachable safety belts consisting of a lap strap and an automatic locking (inertia reel) shoulder harness. However, before the occurrence flight, the shoulder harness portions of these safety belts were rolled up and taped with electrical tape, which prevented them from being used.
Subsection 101.1(1) of the CARs defines a safety belt as “a personal restraint system consisting of either [emphasis added] a lap strap or a lap strap combined with a shoulder harness.” Based on this definition, Hydro One Networks Inc. considered that it would be in compliance with the regulations that required the use of safety belts if occupants wore either the lap strap alone, or the lap strap combined with the shoulder harness.
From 1990 to 2018, the TSB has investigated many accidents involving aircraft that were equipped with detachable shoulder harnesses where it was determined that the harnesses were not being worn at the time of the accident (Appendix B). Of the 62 accidents identified, 33 were fatal, resulting in 68 deaths. Of those 68 deaths, 37 were individuals who had not been wearing the available shoulder harness. Although the survivability of these 62 accidents varied, the use of shoulder harnesses in many cases could have improved the odds of survival and egress.
Passengers who are not adequately restrained during a survivable accident, particularly when the main passenger compartment remains relatively intact, are at greater risk of receiving serious or fatal injuries than passengers who are adequately restrained. While the interpretation of the regulations was not the only reason for not wearing the shoulder harness in the cases examined, in this case, the ambiguity did affect their use.
TC attempted to clarify the regulations in Aviation Safety Letters 4/2013 and 1/2018, and Advisory Circular 605-004 (November 2014). However, if regulations are not clear in requiring the use of all available components of a safety belt, shoulder harnesses may not be used as intended, increasing the risk of injury or death.
Therefore, the Board recommends that
the Department of Transport amend the Canadian Aviation Regulations to remove any ambiguity associated with the definition of “safety belt”
TSB Recommendation A19-01
This report concludes the Transportation Safety Board of Canada's investigation into this occurrence. The Board authorized the release of this report on . It was first released on .
Correction
Footnote 2 and section 1.5.2 (including Table 3) have been amended to show that 1 of the passengers was an apprentice power line technician, and that the other 2 passengers were journeypersons certified as power line technicians. The original version suggested that all 3 of the power line technicians were apprentices.
This correction was approved by the Board on ; the corrected version of the report was released on .
Appendices
Appendix A – Inconsistencies between the flight manual supplement and the maintenance manual supplement
| Text from the flight manual supplement* | Text from the maintenance manual supplement** |
|---|---|
Required instrument panel placard: “WITH AIR STAIR INSTALLED |
Required instrument panel placard: “WITH AIR STAIR INSTALLED |
Other required placards: On the equipment box (2 places): The Air Stair must be placarded as follows: |
Other required placards: On the equipment box (2 places): The Air Stair must be placarded as follows: The aft handle must be placarded as follows: The tether points must be placarded as follows: The counterweight brace must be placarded as follows: |
Description The Air Stair is intended for, but not restricted to, providing aerial access to Hydro towers to qualified linemen. |
Description This system is intended for embarkation and disembarkation of linemen while in flight. A tool tray and seat may be installed on the platform to allow a lineman to perform maintenance tasks from the platform. |
* JCM Aerodesign Limited, Flight Manual Supplement No. 003063FMS (TC approved 27 September 2007), p. 4.
** JCM Aerodesign Limited, Maintenance Manual Supplement No. 003063MMS (TC accepted 28 September 2007), p. 7.
*** Hydro One uses the terms “cross-rail” and “cross bar” synonymously.
Appendix B – Accidents in which at least one occupant was not wearing an available shoulder harness
| TSB occurrence number | Number of occupants by gravity of injury | Fatal injuries to individuals not wearing the available shoulder harness | |||
|---|---|---|---|---|---|
| Fatal | Serious | Minor | None | ||
| A93H0023 | 7 | 0 | 0 | 0 | 2 |
| A93W0159 | 0 | 1 | 0 | 0 | 0 |
| A94C0065 | 0 | 0 | 3 | 0 | 0 |
| A94P0215 | 0 | 0 | 0 | 1 | 0 |
| A94W0162 | 0 | 0 | 0 | 1 | 0 |
| A95C0139 | 3 | 1 | 4 | 0 | 1 |
| A95H0012 | 8 | 2 | 0 | 0 | 1 |
| A95O0150 | 1 | 0 | 0 | 0 | 1 |
| A96P0105 | 0 | 0 | 2 | 0 | 0 |
| A96P0201 | 1 | 0 | 0 | 0 | 1 |
| A96W0055 | 0 | 1 | 0 | 0 | 0 |
| A97P0303 | 0 | 2 | 0 | 0 | 0 |
| A98W0086 | 0 | 1 | 2 | 0 | 0 |
| A99C0137 | 1 | 1 | 0 | 0 | 1 |
| A99P0075 | 4 | 0 | 0 | 0 | 2 |
| A00A0071 | 1 | 0 | 3 | 0 | 1 |
| A00A0076 | 1 | 0 | 0 | 0 | 1 |
| A00P0010 | 0 | 1 | 2 | 0 | 0 |
| A00P0094 | 1 | 0 | 0 | 0 | 1 |
| A01Q0166 | 3 | 1 | 3 | 0 | 2 |
| A01W0186 | 1 | 2 | 0 | 0 | 1 |
| A01W0261 | 3 | 3 | 0 | 0 | 2 |
| A02O0287 | 0 | 2 | 0 | 0 | 0 |
| A02P0320 | 0 | 0 | 3 | 0 | 0 |
| A02W0064 | 0 | 0 | 3 | 0 | 0 |
| A02W0178 | 1 | 0 | 0 | 0 | 1 |
| A02O0295 | 2 | 0 | 0 | 0 | 2 |
| A03O0341 | 2 | 1 | 0 | 0 | 2 |
| A03Q0103 | 1 | 0 | 0 | 1 | 1 |
| A04A0079 | 1 | 0 | 0 | 0 | 1 |
| A04O0174 | 0 | 0 | 1 | 1 | 0 |
| A04W0114 | 2 | 2 | 0 | 0 | 0 |
| A04P0199 | 1 | 0 | 0 | 0 | 1 |
| A04O0256 | 0 | 0 | 1 | 0 | 0 |
| A05Q0119 | 0 | 1 | 1 | 0 | 0 |
| A05Q0178 | 1 | 0 | 4 | 0 | 1 |
| A06W0104 | 1 | 1 | 2 | 0 | 1 |
| A07A0134 | 0 | 2 | 8 | 0 | 0 |
| A07P0209 | 0 | 1 | 1 | 0 | 0 |
| A07Q0014 | 0 | 3 | 1 | 1 | 0 |
| A08A0007 | 0 | 2 | 0 | 0 | 0 |
| A08A0095 | 0 | 4 | 3 | 0 | 0 |
| A08W0197 | 0 | 2 | 3 | 0 | 0 |
| A08C0255 | 0 | 0 | 1 | 1 | 0 |
| A10Q0087 | 2 | 0 | 0 | 0 | 2 |
| A10P0147 | 4 | 0 | 0 | 0 | 2 |
| A11O0205 | 3 | 0 | 0 | 0 | 2 |
| A11C0102 | 1 | 0 | 8 | 0 | 1 |
| A11P0149 | 2 | 7 | 0 | 0 | 1 |
| A11W0070 | 1 | 0 | 0 | 0 | 0 |
| A11W0152 | 1 | 0 | 0 | 0 | 0 |
| A12O0071 | 2 | 1 | 0 | 0 | 1 |
| A12C0104 | 0 | 1 | 0 | 0 | 0 |
| A12O0182 | 1 | 0 | 1 | 0 | 0 |
| A13O0195 | 0 | 0 | 0 | 1 | 0 |
| A14O0105 | 0 | 0 | 2 | 1 | 0 |
| A14O0217 | 2 | 0 | 0 | 0 | 0 |
| A15C0005 | 0 | 1 | 0 | 0 | 0 |
| A16C0060 | 0 | 0 | 1 | 0 | 0 |
| A18O0041 | 0 | 1 | 0 | 0 | 0 |
| A18O0086 | 0 | 0 | 0 | 2 | 0 |
| A18O0153 | 2 | 0 | 0 | 0 | 1 |
| Total | 68 | 48 | 63 | 10 | 37 |