Controlled flight into terrain
North Star Air Ltd.
Douglas DC3C Basler Turbo Conversions TP67, C-FKAL
Sachigo Lake Airport, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Executive summary
On 03 December 2019, a captain and first officer from North Star Air Ltd. (North Star Air) were scheduled to conduct a daytime cargo flight on board the Douglas DC3C Basler Turbo Conversions TP67 (DC3-TP67) aircraft (registration C-FKAL, serial number 25285) from Red Lake Airport (CYRL), Ontario, to Sachigo Lake Airport (CZPB), Ontario. During flight planning, the captain checked the weather: at 0700 Central Standard Time (CST), CYRL reported an overcast ceiling at 700 feet above ground level (AGL). Muskrat Dam Airport (CZMD), Ontario, located 30 NM southeast of CZPB, reported instrument meteorological conditions (IMC) with an overcast ceiling at 500 feet AGL. The forecast at CZMD was to improve to 1500 feet AGL with a possible fluctuation to 700 feet AGL and decreased visibility by 0900 CST, i.e., the aircraft’s estimated time of arrival into CZPB. The flight departed CYRL under visual flight rules (VFR) at 0800 CST. The reported weather at the time was broken ceiling at 1200 feet AGL and an overcast layer based at 2000 feet AGL.
Shortly after takeoff, the aircraft entered, and climbed above, the cloud layers before reaching the planned cruising altitude, which was not in accordance with the applicable regulations for VFR flights. Before commencing the descent to CZPB, the pilots obtained the 0800 CST hourly weather report at CZMD, which had remained generally unchanged from the 0700 CST report, and elected to carry out a visual approach to Runway 10. The captain initiated a descent through the cloud layers by reference to the flight instruments.
Once the aircraft broke out of cloud at very low level, the aircraft was not in a position to continue with the planned visual approach. The captain made low-level manoeuvres in an attempt to land, flying a large 360° turn, as low as 100 feet AGL (i.e. about 400 feet below the required minimum altitude), and then flew a manoeuvre similar to a left-hand circuit, which brought the aircraft within close proximity to a significant obstacle (a 150-foot tall tower), in meteorological conditions below the VFR minimum requirements. Given that the captain had not briefed the first officer, the latter was unaware of the captain’s intentions and began calling out airspeed and altitudes. On the last attempt, during the low-level downwind leg, when the aircraft passed abeam the threshold of Runway 10, the captain initiated a left-hand turn and began descending. About 10 seconds later, the aircraft collided with terrain, in a near wings-level attitude, approximately 650 feet southwest of the threshold of Runway 10. The aircraft slid 350 feet southward along the ground before it came to a rest on a southwesterly heading.
The captain likely experienced attentional narrowing while carrying out a high-workload visual approach at very low altitude in IMC. This most likely resulted in an inadvertent but controlled descent that was not detected until the aircraft collided with terrain.
The uninjured pilots evacuated the aircraft via the right-hand cockpit window. The aircraft sustained substantial damage; however, there was no post-impact fire.
The 406-MHz emergency locator transmitter (ELT) activated; however, the whip antenna had been ripped off during the impact sequence and no signal was detected by the search and rescue satellite system. The TSB had previously recommended that Transport Canada (TC) establish more rigorous ELT system crash survivability requirements, and TC has since implemented updated regulations for new ELT design approvals; however, those requirements do not apply to legacy ELTs like the one the occurrence aircraft was equipped with. If aircraft operate with ELTs approved under legacy design standards, there remains a risk that potentially life-saving distress signals will not be detected because of damage caused to the ELT system during an accident.
Although the regulations did not require the occurrence aircraft to be equipped with a flight data recorder or a cockpit voice recorder (CVR), North Star Air had installed a CVR. However, following repairs, a paperwork error resulted in the CVR being placed in inventory instead of being re-installed in the occurrence aircraft. At the time of occurrence, it had been 329 days since the CVR had been removed, i.e., over 200 days beyond the maximum permissible time defined in the minimum equipment list. Without the CVR, valuable information was not available to assist the investigation. If cockpit voice and flight data recordings are not available, it is more difficult to accurately assess crew resource management, standard operating procedure execution and effectiveness, and workload management. As a result, the absence of on-board flight recordings can limit the identification of safety deficiencies and the advancement of safety.
The investigation revealed that the result-oriented subculture of some North Star Air’s DC3-TP67 pilots, which emphasized mission completion over regulatory compliance, resulted in VFR flights, such as the occurrence flight, being conducted in IMC. The investigation also determined the captain had a history of conducting VFR flights in IMC. The decision to depart on, and continue, a VFR flight in IMC was influenced by a distorted perception of risk resulting from successful past experience in similar situations. In addition, the company structure was such that there was no operational management presence and no day-to-day direct pilot supervision of DC3-TP67 flight operations and flights crews at the company’s remote bases, nor is it required by regulation. The absence of direct supervision meant that company pilots had considerable latitude when it came to making operational weather-related decisions. Over time, a culture of non-compliance developed that went undetected by the company management team. If minimal supervision of flight crews occurs within a company’s flight operation, there is a risk that previously identified unsafe or non-compliant practices will persist.
In December 2017, TC informed North Star Air that it had received allegations related to company DC3-TP67 aircraft operated on multiple occasions under VFR in IMC. TC provided the information about the allegations to the company for its internal investigation. In response, the operations manager contacted all the DC3-TP67 captains verbally and via email reminding them of the requirement to abide by the regulations, but the company did not outline any additional measures to monitor North Star Air’s DC3-TP67 operation for reoccurrence. Additionally, in February 2018, TC initiated a reactive process inspection (PI) that included 3 flight inspections, which were deemed uneventful.
North Star Air had a safety management system (SMS), even though at the time of the allegations it was not required by regulations. An SMS hazard report was created and entered into North Star Air’s SMS database. However, the SMS did not identify the underlying factors that led to the reported instances of company aircraft operating VFR flights into IMC and the company did not take any additional measures to monitor its DC3-TP67 operation to ensure flights were being conducted in accordance with regulations. Additionally, TC’s November 2018 PI did not include a review of the 2017 allegations. As a result, previously identified unsafe practices persisted, and played a direct role in this occurrence. If TC relies on operators to investigate allegations of regulatory non-compliance without monitoring them, there is an increased risk that the unsafe practices that are being investigated will persist.
Safety management is on the TSB Watchlist and will remain on it until transportation operators that do have an SMS demonstrate to TC that it is working—that hazards are being identified and effective risk-mitigation measures are being implemented.
The investigation revealed that TC’s approach to surveillance resulted in North Star Air’s SMS being approved even though several elements were not fully implemented. If TC approves a company’s SMS without first conducting an in-depth review to ensure that all required elements are present and effective, SMS enterprises may not have the ability to effectively manage safety.
The TSB previously recommended that TC conduct regular SMS assessments to evaluate the capability of operators to effectively manage safety. In its latest response, in September 2021, TC indicated that it was taking measures to update and improve its surveillance methodology.
Regulatory surveillance is also on the TSB Watchlist and will remain on it until TC demonstrates through surveillance activity assessments that the new surveillance methodology is identifying non-compliances, and that TC is ensuring that a company returns to compliance in a timely fashion and is able to manage the safety of its operations.
Following the occurrence, North Star Air implemented a flight operations quality assurance program. Additionally, in December 2020, TC conducted a PI focused on the evaluation and effectiveness of the long-term corrective action plan related to the flight operations findings from the December 2019 PI. TC concluded that the long-term corrective actions taken by North Star Air were effective.
1.0 Factual information
1.1 History of the flight
At approximately 0715Footnote 1 on 03 December 2019, the captain and the first officer (FO) arrived at the North Star Air Ltd. (North Star Air) hangar at Red Lake Airport (CYRL), Ontario. The pilots were scheduled to conduct a daytime cargo flight on board the Douglas DC3C Basler Turbo Conversions TP67 (DC3-TP67) aircraft (registration C-FKAL, serial number 25285) to Sachigo Lake Airport (CZPB), Ontario, approximately 180 nautical miles (NM) north-northeast of CYRL.
The captain checked the weather and completed the flight planning while the FO fuelled the aircraft and ground personnel loaded the aircraft. The reported weather at CYRL at 0700 was an overcast ceiling at 700 feet above ground level (AGL) and visibility was 10 statute miles (SM). Given that CZPB does not have a weather reporting station, the captain also checked the weather at Muskrat Dam Airport (CZMD), Ontario, located 30 NM southeast of CZPB. The reported weather at 0700 for CZMD was an overcast ceiling at 500 feet AGL, with a visibility of 9 SM; however, the forecast ceiling was to improve to 1500 feet AGL with a possible fluctuation to 700 feet AGL and decreased visibility by 0900, the aircraft’s estimated time of arrival into CZPB.
At 0800, the aircraft departed CYRL under visual flight rules (VFR); however, a flight plan or flight itinerary was not filed. The captain was seated in the left seat and was the pilot flying (PF); the FO was seated in the right seat, performing the pilot not flying (PNF) duties. The reported weather at the time was a broken ceiling based at 1200 feet AGL, an overcast layer based at 2000 feet AGL, and a visibility of 10 SM. Shortly after takeoff, the aircraft entered cloud. During the climb to the planned cruising altitude of 5500 feet above sea level (ASL), the aircraft exited, and then remained above the cloud layers for the en-route portion of the flight.
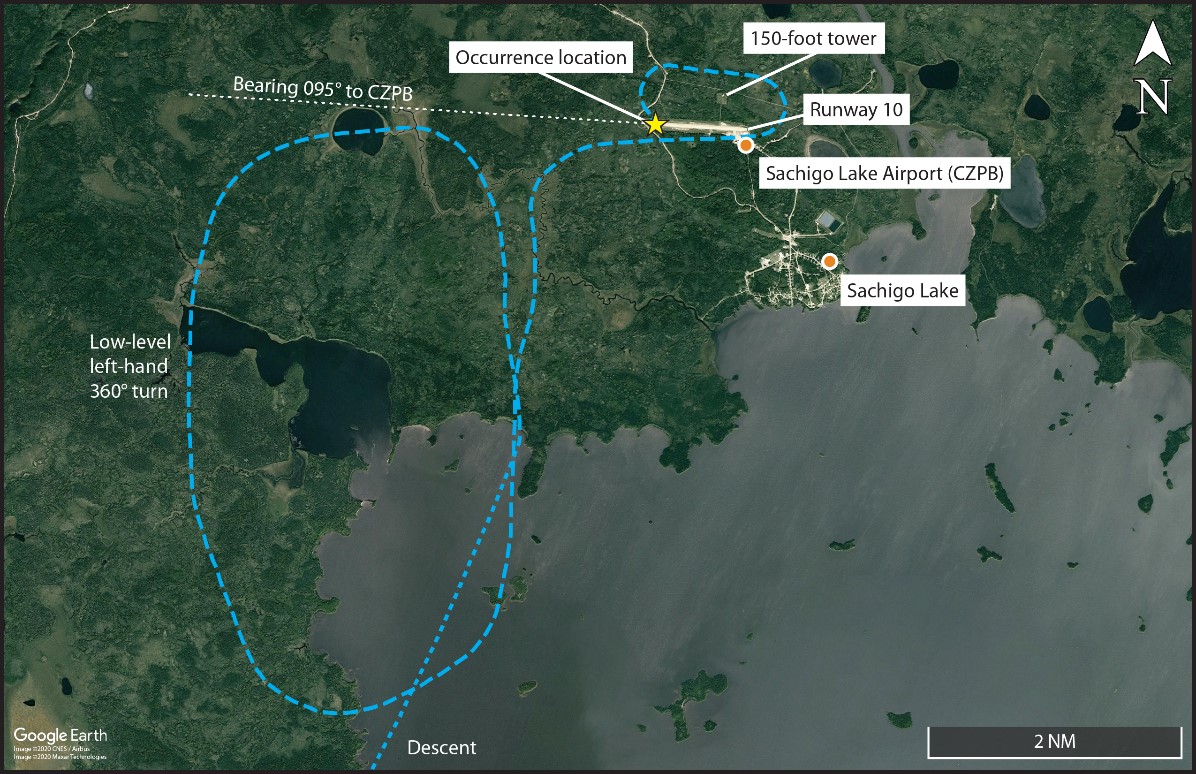
Before commencing the descent to CZPB, the pilots obtained the 0800 hourly weather report at CZMD, which had remained generally unchanged from the 0700 report. Anticipating that the weather would improve, the pilots elected to carry out a visual approach to Runway 10, and to enter the area navigation (RNAV) global navigation satellite system (GNSS) Runway 10 approachFootnote 2 into the Garmin 530W GPS (global positioning system) for additional guidance for the visual approach. At 0857, approximately 16 NM south of CZPB, the captain initiated a descent. Shortly after, the aircraft entered cloud, and the captain reverted to flight by reference to the flight instruments. During this time, the captain observed rime ice accumulating on the wings and selected the aircraft’s ice protection systems on.Footnote 3 To assist with alignment for the approach, the FO selected, at the captain’s request, an omni-bearing selector (OBS)Footnote 4 bearing of 095° to CZPB. At 3 NM from CZPB, the captain levelled off at 350 feet AGL, then continued the descent to 200 feet AGL and turned approximately 30° left to position the aircraft to join the right base leg before intercepting the final approach for Runway 10. However, t approximately 1.5 NM from the threshold of Runway 10, and 0.5 NM south of the planned final track, once the aircraft broke out of cloud, the captain realized that the aircraft was not in a position to continue with the planned visual approach. The captain then commenced a wide, low-level left-hand 360°-turn, at heights ranging between 100 and 350 feet AGL, in order to reposition the aircraft for landing on Runway 10 (Figure 1).
At some point after commencing the 360°-turn, the captain turned off the ice protection system as required by the aircraft flight manual.Footnote 5 During this low-level manoeuvre, the ragged cloud bases were between 350 feet and 500 feet AGL, with reduced horizontal visibility below 3 SM, in snow and mist. Given that the captain had not briefed the FO, the latter was unaware of the captain’s intentions and began calling out airspeed and altitudes.
Upon completion of the wide left-hand 360°-turn, the aircraft rolled out approximately 1.25 NM southwest of the airport and 0.5 NM south of the planned final approach track. Again, the captain realized that the aircraft was not in a position to intercept the final approach course to Runway 10. The captain then turned right and flew parallel to, and just south of, Runway 10, passing overhead of the terminal, at approximately 200 feet AGL. Once past the departure end of Runway 10, the captain turned left and flew a left downwind leg to Runway 10, with a cross track distance of approximately 0.4 NM. On the downwind leg, the aircraft’s altitude varied from 150 feet to 225 feet AGL, and the aircraft passed within 0.12 NM of a tower that was 150 feet tall and located between the aircraft’s track and Runway 10.
As the aircraft passed abeam the threshold of Runway 10, the captain initiated a left-hand turn and began descending. At 0911, approximately 10 seconds after initiating the turn to final, the aircraft collided with terrain, in a near wings-level attitude, approximately 650 feet southwest of the threshold of Runway 10. The aircraft slid 350 feet southward along the ground before it came to a rest on a southwesterly heading.
The captain and FO evacuated the aircraft through the FO’s cockpit window. A local hunter, who heard the crash, was the first to arrive on the accident site. Nishnawbe Aski Police Service arrived shortly after and transported the uninjured pilots to the Sachigo Lake nursing station for evaluation. The emergency locator transmitter (ELT) activated; however, no signal was detected by the search and rescue (SAR) satellite system.
1.2 Injuries to persons
There were no injuries to either of the 2 pilots.
1.3 Damage to aircraft
The aircraft was substantially damaged by impact forces, but remained largely in 1 piece.
1.4 Other damage
A swath of trees and undergrowth (70 feet wide by 240 feet long) was damaged. Several litres of hydraulic fluid and engine oil were dispersed along the wreckage trail.
1.5 Personnel information
| Captain | First officer | |
|---|---|---|
| Pilot licence | Airline transport pilot licence (ATPL) | Commercial pilot licence (CPL) |
| Medical expiry date | 01 April 2020 | 01 July 2020 |
| Total flying hours | Approximately 14 000 | Approximately 1100 |
| Flight hours on type DC3-TP67 | Approximately 2900 | Approximately 850 |
| Flight hours on type DC3 equipped with radial engines | Approximately 9000 | 0 |
| Flight hours in the 7 days before the occurrence | 29.6 | 27.6 |
| Flight hours in the 30 days before the occurrence | 116 | 56 |
| Flight hours in the 90 days before the occurrence | 269 | 189 |
| Flight hours on type in the 90 days before the occurrence | 269 | 189 |
| Hours on duty before the occurrence | 2 | 2 |
| Hours off duty before the work period | 8.5 | 8.5 |
1.5.1 Captain
The captain was hired by North Star Air in 2017 as a captain on the DC3-TP67. Before joining North Star Air, he had worked for another Canadian operator where he had flown DC3 aircraft equipped with radial engines. He had extensive experience conducting cargo flights to remote airports and winter operations in icing conditions.
The captain held a Category 1 medical certificate with no restrictions. His most recent DC3-TP67 pilot proficiency check was successfully completed on 01 March 2019. He was on his 2nd week of a 3-week rotation. Records indicate that the captain was certified and qualified for the flight in accordance with existing regulations. Based on a review of the captain’s work and rest schedules, he had an 8.5-hour rest period before the occurrence flight duty period, which complied with the minimum required by regulation.Footnote 6 Fatigue was not considered to be a factor in this occurrence.
The captain completed North Star Air’s initial 1-day crew resource management (CRM) course on 15 September 2019. The training was taught by the company’s operations manager (OM). North Star Air uses an electronic tracking program for currency requirements. For CRM training, the program will issue a certificate of completion on the date that the pilot acknowledges having completed the training, rather than the actual training date. The captain’s certificate of completion, from the tracking software, was dated 02 November 2019. According to the company, some pilots would not electronically sign off their training until the company training administrator contacted them personally to acknowledge the training had been completed.
1.5.2 First officer
The FO was initially hired by North Star Air in 2017 as a ramp worker. In September 2018, he was promoted to FO on the DC3-TP67. This was the FO’s first commercial flying position. The FO held a Category 1 medical certificate with no restrictions. His most recent DC3-TP67 pilot proficiency check was successfully completed on 01 October 2019. The FO was on his last day of a 2-week rotation. Records indicate that he was certified and qualified for the flight in accordance with existing regulations. Based on a review of the FO’s work and rest schedules, he had an 8.5-hour rest period before the occurrence flight duty period, which complied with the minimum required by regulation. Fatigue was not considered to be a factor in this occurrence.
The FO completed North Star Air’s initial 1-day CRM course on 29 September 2019. The training was taught by one of the company’s designated CRM trainers. Based on the currency tracking software, the FO’s certificate of completion was dated 11 October 2019.
1.6 Aircraft information
1.6.1 General
The occurrence aircraft was built in the U.S. by the Douglas Aircraft Company in 1943 and was originally equipped with 2 Pratt & Whitney Twin Wasp R-1830 piston radial engines. It is a low-wing aircraft with a retractable main landing gear and a non-retractable tailwheel.
In 2012, the aircraft was converted to a DC3-TP67 by Basler Turbo Conversions Inc., in accordance with Supplemental Type Certificate SA4840NM.Footnote 7 The Basler conversion included Pratt & Whitney PT6A-67R engines, updated avionics suite, and modification to the fuselage and the wing tip leading edge. The DC3-TP67 is certified for day, night, and instrument conditions, and approved for flight into known or forecast icing conditions.Footnote 8
During the conversion, the aircraft was also equipped with the following pieces of equipment that were relevant to the occurrence:
- Two Garmin GNS 530W all-in-one GPS, Navigation and Communication units, approved for VFR and instrument flight rules (IFR) operations, including IFR GPS approaches. The system includes a moving map and colour display, which depicts traffic, weather, and terrain.
- A Honeywell KMH980 traffic alert and collision avoidance system/multi-hazard awareness system. The system includes a KMH920 multi-hazard awareness unit. Traffic and terrain are displayed on a Garmin GMS200 multi-function display.
| Manufacturer | Douglas Air Company |
|---|---|
| Type, model, and registration | DC3-TP67, C-FKAL |
| Year of manufacture | 1943 |
| Serial number | 25285 |
| Certificate of airworthiness/flight permit issue date | 13 December 2012 |
| Total airframe time | 36 496.1 (02 December 2019) |
| Engine type (number of engines) | Pratt & Whitney Canada PT6A-67R (2) |
| Propeller type (number of propellers) | Hartzell HC-B5MA-3M (2) |
| Maximum allowable take-off weight | 30 000 pounds |
| Recommended fuel types | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A-1 |
The aircraft had been owned and operated by North Star Air since 03 May 2017. North Star Air had completed a 150-hour maintenance inspection on the occurrence aircraft on 20 November 2019, and the most recent maintenance daily inspection had been completed on 02 December 2019. Records indicate that there were no outstanding defects at the time of the occurrence. There was no indication that a component or system malfunction played a role in this occurrence.
The aircraft weight and centre of gravity were within the prescribed limits at the time of the occurrence.
1.6.2 Aerodynamic stall
According to Basler, the stall characteristics of the DC3-TP67 when straight and level or in a coordinated 30-degree bank turn, and with the landing gear down and flaps set to 1 (one quarter), are as follows:
- Controls become softer as airspeed decreases
- Audible stall warning sounds
- Buffet in airframe
- Nose pitches downward in spite of elevator control aft
- No tendency to roll
1.6.3 Stall warning system
The stall warning system installed on the occurrence aircraft consisted of an angle-of-attack vane and a computer. The electrically heated angle-of-attack vane was mounted on the right side of the fuselage below the right-hand pilot’s sliding window.Footnote 9 The angle-of-attack sensing vane rotates to detect the angle between the relative wind and the longitudinal axis of the fuselage. The stability augmentation computer senses the position of the angle-of-attack vane, and when appropriate, sends a signal to the tone generator. The tone generator creates a distinct audio tone to warn the flight crew of an impending stall.
The investigation found no indication that the stall warning system activated during the occurrence flight.
1.6.4 Ice protection systems
The occurrence aircraft was equipped with ice protection systems, which included heated pitot-static tubes, propeller electric de-ice boots, electrically heated windshields, wing and tail surface pneumatic de-ice boots, engine electrically heated inlet-lip boots, and engine inertial particle separators (snow deflectors). Aircraft ice protection systems were selected ON during the descent through clouds, as the aircraft was approaching CZPB.
1.7 Meteorological information
1.7.1 General
According to the graphic area forecast (GFA) valid during the occurrence flight,Footnote 10 the weather along the route was forecast to be as follows:
- Visibility 2 SM in light snow
- Patchy ceiling at 700 feet AGL
- LocalFootnote 11 visibility of 1 SM in light snow
During the duration of the occurrence flight, patchy moderate mixed icing in cloud was forecast between 3000 and 9000 feet ASL.
According to the aerodrome forecast (TAF)Footnote 12 for CZMD valid at the time,Footnote 13 the weather was forecast to be as follows:
| Condition | Before 0900 | After 0900 |
|---|---|---|
| Winds | Variable at 3 knots | 270° True (T) at 10 knots |
| Visibility | 4 SM in light snow | 6 SM in light snow; temporarily from 0900-1700, 4 SM in light snow |
| Overcast ceiling | 500 feet AGL | 1500 feet AGL; temporarily from 0900-1700, 700 feet AGL |
At 0800, at the time of takeoff, the reported weather at CYRL was a broken ceiling based at 1200 feet AGL, an overcast layer based at 2000 feet AGL, and a visibility of 10 SM.
At 0911, at the time of the accident, CZMD issued an aerodrome special meteorological report (SPECI)Footnote 14 indicating the following weather:
- Wind 240°T at 6 knots
- Visibility 6 SM in light snow showers
- Overcast ceiling at 300 feet AGL
- Temperature −8 °C, dew point −9 °C
- Altimeter setting 29.34 inches of mercury
According to the reported weather, instrument meteorological conditions (IMC) existed in the vicinity of CZPB during flight planning and for the entire flight.Footnote 15
The investigation determined that, at the time of the occurrence, personnel located near CZPB’s main terminal were unable to see the 150-foot tall tower, which was approximately 0.4 NM away from where they were.
At the time of the occurrence, the combination of snow-covered terrain, with an overcast sky and falling snow, created dull lighting conditions in the vicinity of CZPB.
1.8 Aids to navigation
Not applicable.
1.9 Communications
Not applicable.
1.10 Aerodrome information
The CZPB airport reference elevation is 876 feet ASL. There is 1 runway, Runway 10/28, which runs east-west, has a gravel-surface, and is 3506 feet long and 100 feet wide. At the time of the occurrence, 2 RNAV approaches were available, RNAV Runway 10 and RNAV Runway 28, with decision altitudes of 1363 feet ASL (500 feet AGL) and 1371 feet ASL (500 feet AGL), respectively.Footnote 16
1.11 Flight recorders
1.11.1 Automatic dependent surveillance-broadcast system
Although not required by regulation, the occurrence aircraft was equipped with an automatic dependent surveillance-broadcast out (ADS-B out) system. The ADS-B out system broadcasts information such as aircraft position, altitude, and ground speed to air traffic control. Through a partnership with NAV CANADA, Aireon receives these data using a satellite system and records them. The ADS-B out system on board the occurrence aircraft transmitted data every few seconds and provided the investigation with useful flight path information. The results will be discussed further in section 1.16.2 of the report.
1.11.2 Satellite communication system
The aircraft was equipped with a Honeywell Sky Connect satellite communication system (part number [P/N] 1616-050-03A, serial number [S/N] 17185) that permitted communication and tracking via the Iridium satellite system. The system, which is not required by regulation, automatically transmits aircraft altitude, speed, and position data, which is then stored on ground-based servers. The automated flight-following system consists of satellite tracking technology on the ground and in the aircraft. Using a web interface, the operator is able to monitor the aircraft stored data and retrieve flight data from the previous 6 months.
The Sky Connect system records and transmits at intervals determined by the user’s requirements. The default interval for this system is 3 minutes; however, some operators have reduced the interval to as low as 30 seconds. According to Honeywell, operators will sometimes reduce the interval following an accident to improve the system’s ability to establish a more accurate last known position. The occurrence aircraft’s Sky Connect system was programmed to transmit data at 1-minute intervals.
1.11.3 Cockpit voice recorder
Although not required by regulation,Footnote 17 the occurrence aircraft was normally equipped with an L-3 Communications FA-2100 cockpit voice recorder (CVR) (P/N 2100-1020-00, S/N 000812234). On 08 January 2019, the CVR was removed and sent for repair. The CVR repair was deferred in accordance with the minimum equipment list,Footnote 18 which stipulates that items shall be repaired within 120 consecutive calendar days.
In compliance with the minimum equipment list, the circuit breaker was pulled out and secured, and an inoperative (INOP) sticker was placed on the CVR control panel.
While the CVR was undergoing repairs, the contracted provider of technical record keeping inadvertently signed off the CVR repair as having been completed on the aircraft. As a result, when the CVR was returned to North Star Air, it was placed in inventory instead of being re-installed on the occurrence aircraft. Consequently, cockpit audio data for the occurrence flight was not available to the investigation.
At the time of the occurrence, 329 days had elapsed since the CVR had been removed.
1.11.4 Flight data recorder
The flight data recorder (FDR) regulations that apply to multi-engine turbine-powered aircraft are contained in Canadian Aviation Regulations (CARs) section 605.33.
According to Transport Canada (TC), as the occurrence aircraft was operated under a TC-approved supplemental type certificate that limited the maximum number of passenger seats to 19, an FDR was not required by regulation and was not installed on the aircraft.
1.12 Wreckage and impact information
The aircraft struck the ground on an approximate heading of 167° magnetic (M), in a slightly nose-down, right-wing-low attitude with the landing gear extended. The wing flaps were partially extended, consistent with the pilot-selected position of “flaps 1.”Footnote 19
After the landing gear struck the edge of the road adjacent to the airport, the right wing contacted the tree line at a height of about 5 feet. The aircraft slewed to the right, causing the left wing and then the empennage to strike trees at a height of about 20 feet. The aircraft continued to slew right to about 60° from the original direction of travel, sliding approximately 350 feet. The aircraft came to rest (Figure 2) on a heading of 225°M.

The landing gear, wings, and tail sustained extensive damage, and the fuselage was buckled and damaged from impact with trees. The propellers, which separated from the engines, showed damage consistent with the engines producing substantial power on impact. No fuel leakage was evident.
The investigation could not determine how much ice had accumulated on the aircraft during the occurrence flight. However, the investigation was able to determine, based on the pattern of remaining ice, that the wing de-icing boots had been operated during the occurrence flight.
1.13 Medical and pathological information
There was no evidence that the captain’s or FO’s performance was degraded by any medical, or physiological factors.
1.14 Fire
There was no evidence of fire in flight or after the impact.
1.15 Survival aspects
1.15.1 General
The cockpit remained intact and provided a survivable space. Both crew seats remained attached to the aircraft primary structure. The cockpit door became obstructed by freight that shifted during the accident sequence; therefore, the pilots exited the aircraft through the FO’s cockpit window.
1.15.2 Safety belts
The aircraft’s pilot seats were equipped with lap straps and inertia-reel shoulder harnesses. The shoulder harnesses on the DC3-TP67 may make it difficult for some flight crew members to reach the landing gear controls and cockpit instrument panel switches. On the occurrence flight, the flight crew used their lap straps but not their shoulder harnesses.
1.15.2.1 Previous TSB recommendation on the definition of safety belt
The use of a 3- or 4-point restraint system (consisting of a lap strap and shoulder harness) ensures a more equal distribution of the impact forces and reduces the severity of injuries to the upper body and head.
The TSB has investigated many accidentsFootnote 20 involving aircraft that were equipped with detachable shoulder harnesses in which the harnesses were not worn at the time of the accident.
Following an accident involving an Airbus Helicopters AS 350 B2 helicopter on 14 December 2017 in Tweed, Ontario,Footnote 21 the TSB investigation determined that the passengers’ shoulder harnesses were not used with the lap straps. Based on the definition of “safety belt” in the CARs at the time, the company had considered that it would be in compliance with the regulations if the occupants wore either the lap strap alone, or the lap strap combined with the shoulder harness. Therefore, the Board recommended that
the Department of Transport amend the Canadian Aviation Regulations to remove any ambiguity associated with the definition of “safety belt.”
TSB Recommendation A19-01
On 07 July 2021, TC published amendments to relevant sections of CAR 605 that included new wording to remove any ambiguity pertaining to the use of safety belts, and clarified that safety belts, including shoulder harnesses, must be fastened. In March 2022, the Board considered TC’s response to Recommendation A19-01 to be Fully Satisfactory.Footnote 22
1.15.3 Emergency locator transmitter
The Artex Model G406-4 406-MHz ELT (P/N 455-5021-366) activated; however, the whip antenna, which is located on the right side of the aircraft and near the top of the fuselage below the dorsal fin (Figure 3), was ripped off the aircraft during the impact sequence. As a result, the ELT’s distress signal was not detected by the SAR satellite system.

1.15.3.1 Previous TSB recommendation on emergency locator transmitter crash survivability standards
Following an accident involving a Sikorsky S76 helicopter on 31 May 2013 in Moosonee (CYMO), Ontario,Footnote 23 the TSB recognized that aircraft equipped with ELT systems that meet current design standards will continue to be involved in occurrences in which potentially life-saving SAR services will be delayed as a result of damage to the ELT system, decreasing the survivability of an accident. In many instances, ELT signals have not reached the Cospas-SarsatFootnote 24 system because of a broken antenna or a break in the wire connecting the ELT unit to the antenna. Therefore, the TSB recommended that
the Department of Transport establish rigorous emergency locator transmitter (ELT) system crash survivability requirements that reduce the likelihood that an ELT system will be rendered inoperative as a result of impact forces sustained during an aviation occurrence.
TSB Recommendation A16-05
In September 2020, TC indicated that it had amended the CARs to require that, as of 07 September 2020, new applications for design approval of an ELT meet the latest crash survivability requirements.
In its March 2021 reassessment of TC’s response, the Board considered that the actions taken by TC will significantly reduce the risks associated with the safety deficiency identified in Recommendation A16-05. Therefore, the Board considered the response to Recommendation A16-05 to be Fully Satisfactory. Footnote 25 However, the TSB noted that these new standards do not apply to legacy ELTs.
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP003/2020 – NVM Data Recovery
- LP090/2020 – ADS-B Data Analysis
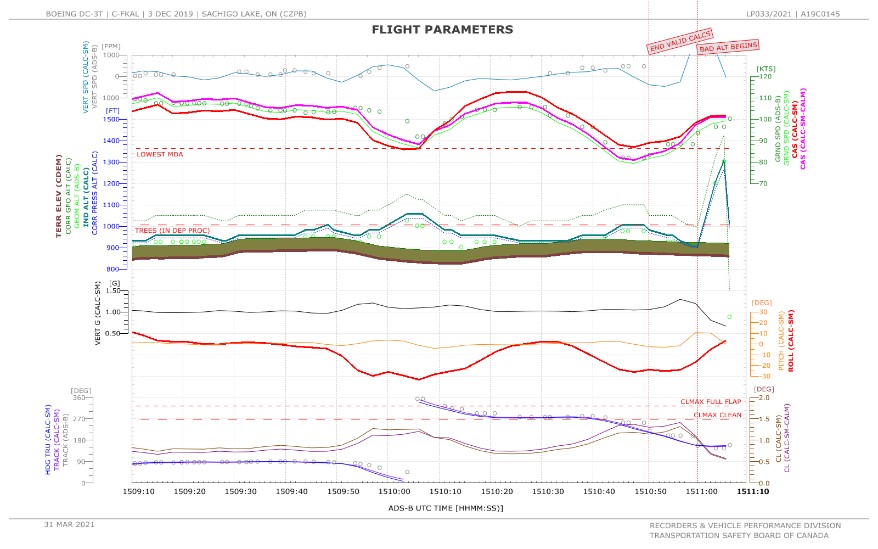
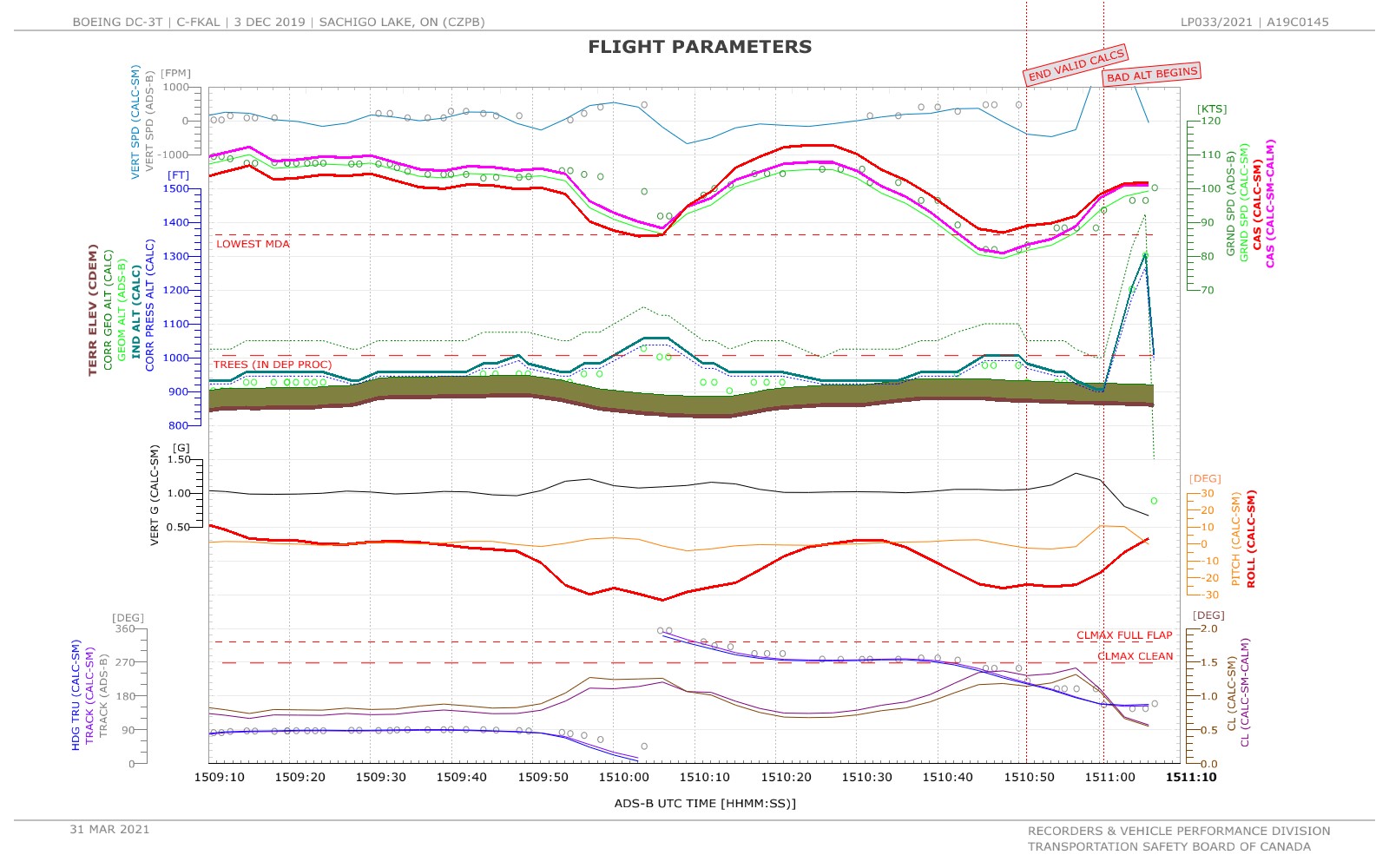
- LP033/2021 – Performance Analysis
1.16.2 Performance analysis
1.16.2.1 General
To assist the investigation, a performance analysis was conducted at the TSB Engineering Laboratory in Ottawa, Ontario, using NAV CANADA’s and Aireon’s ADS-B data and available weather information. The ADS-B data contained position, altitude, ground speed, track, and vertical rate information. This made it possible to reconstruct the final 11 minutes of the occurrence flight (Appendix A).
1.16.2.2 Aerodynamic stall assessment
After passing south of the airfield, the aircraft entered a left-hand turn to position on a downwind leg for the circuit. The entry to the first turn was made at about 100 knots calibrated airspeed (KCAS), which reduced to about 86 KCAS as the altitude increased by about 100 feet. The estimated bank angle averaged about 30°. During the brief level period after the turn as the aircraft flew westward and generally parallel to the runway, the airspeed recovered to about 113 KCAS and the altitude returned to the entry value.
The final turn was similar; however, the estimated bank angle was about 25°, which was shallower than the previous turn. As the aircraft entered the turn, the airspeed decreased to a minimum value of 87 KCAS, and the altitude increased by about 60 feet. The lowest airspeed and highest altitude occurred relatively early in the turn as the heading was passing through southwest. Beyond this point, the altitude reduced again, the airspeed increased, and the bank angle either remained steady or reduced.
Based on the aircraft weight, configuration, and banked turn of 30° at constant altitude, the power-off stall speed was estimated to be 77 KCAS. As a result, the lowest estimated airspeed margin for stall was 10 KCAS during the final turn. It was also determined that the stall margin was greater during the final turn than it was during the turn to the downwind leg of the circuit. The margins would have been greater with power on, as was the case in this occurrence. Any effects of residual ice contamination on the stall margin are unknown. In addition, the stall warning system did not activate during the crash sequence. Based on this performance analysis, the investigation determined that it is unlikely that the aircraft stalled during the final turn.
1.16.2.3 Tree contact
During the final seconds of recorded ADS-B data, the last 3 recorded data points showed anomalous altitude values. In particular, the data points indicated a sudden 400-foot climb and descent within about 7 seconds. The investigation believed that this was unrealistic and inconsistent with the nature of the crash damage. It was determined, in consultation with Aireon, NAV CANADA’s provider for satellite-based ADS-B services, that the probability of the recorded values being somehow corrupted after transmission by the aircraft was extremely remote. In addition, this anomalous data coincided with the aircraft’s passage over an area of tall trees on the northern edge of the runway clearing; there were no other indications of erroneous data at any other point during the flight. The circumstances therefore suggest a high likelihood that the erroneous pressure altitude data transmitted by the aircraft via ADS-B was the result of damage to the pitot-static tubes just before impact with the ground. The investigation determined that the last 11 minutes of the flight were generally flown only 100 feet or less from treetops, and within 200 feet or less of the ground. During the final turn, the aircraft’s altitude had been steadily decreasing toward terrain over about 10 seconds before reaching one of its lowest points during the entire flight. This position coincided with the last valid altitude data. At that point, the corrected barometric altitude placed the aircraft at or below the estimated height of the treetops.
The DC3-TP37 aircraft’s air data system uses pitot-static tubes to measure altitude. The tubes are mounted on very long supports that hang unusually low below the fuselage, by about 2 feet (Figure 4). They are vulnerable to damage if there is any contact with treetops. Since the air data system requires precision calibration to measure altitude correctly, damage to the pitot-static tubes could lead to erroneous altitude measurements.

The investigation determined that it is highly likely that the erroneous altitude data in the final seconds of the flight was the result of damage to the pitot-static tubes from contact with treetops north of the runway clearing. The aircraft did not subsequently climb away and it impacted the ground and road adjacent to the runway perimeter fence.
1.17 Organizational and management information
1.17.1 General
Reference in this report to company manuals, procedures and checklists, or sections thereof, refers to information within these documents that was applicable on the date of the occurrence.
1.17.2 North Star Air
North Star Air, which was established in 1997, holds an operating certificate for operations under CARs subparts 604 (private operators), 703 (air taxi operations), 704 (commuter operations), and 705 (airline operations). It also holds an approved maintenance organization certificate (CARs Subpart 573). The company’s headquarters is located at the Thunder Bay Airport (CYQT), Ontario. It has 5 remote bases, 4 in Ontario (Sioux Lookout Airport [CYXL], Pickle Lake Airport [CYPL], Red Lake Airport [CYRL], and Kapuskasing Aerodrome [CYYU]) and 1 in Manitoba (Thompson Airport [CYTH]). North Star Air provides passenger, charter, and cargo service to more than 50 remote northern communities in Ontario, Manitoba, and Nunavut. At the time of the occurrence, the North Star Air fleet consisted of 3 DC3-TP67 aircraft, 3 Avions de Transport Régional ATR72-500 aircraft, and 7 Pilatus PC12 aircraft. The occurrence aircraft was being operated under CARs Subpart 704. The company consisted of over 250 employees, including 27 management staff, 75 pilots, 10 flight followers, 29 maintenance personnel, and 133 support staff.
North Star Air operations were authorized for flight conducted under VFR and IFR. The company did not have authorization for VFR over-the-top operations.Footnote 26
1.17.3 Organizational structure at North Star Air
At the time of the accident, North Star Air’s organizational structure was as shown in Figure 5.
![North Star Air organizational structure (Source: North Star Air, Company Operations Manual, Revision 6 [16 January 2019], section 2.1, p. 2.1-1)](/sites/default/files/eng/rapports-reports/aviation/2019/a19c0145/images/a19c0145-figure-05.jpg)
At North Star Air, the “Accountable Executive has full responsibility for and authority over all human resources and major financial decisions.”Footnote 27 The accountable executive (AE), at the time of the occurrence, had been in that position since 2014 and had served as the operations manager (OM) for 2 years before that.
The OM is responsible for safe flight operations, in accordance with CARs Commercial Air Service Standard 724,Footnote 28 and reports to the AE. At the time of the occurrence, the OM had been in that position since 2014.
Both the AE and OM were based at the North Star Air headquarters.
There was a chief pilot (CP) for the company’s CARs Subpart 703 operations and another one for both CARs subparts 704 and 705 operations. According to North Star Air’s company operations manual (COM), the CPs are responsible to the OM for the professional standards of the pilots under their authority.Footnote 29
The 704 and 705 operations CP at the time of the occurrence assumed that double role on 31 July 2019, following a company decision to merge those duties under a single CP. His background was predominantly with CARs Subpart 705 operations. Before becoming CARs subparts 704 and 705 operations CP, he had flown as a line pilot on North Star Air’s ATR-72 since September 2018. He worked remotely from Alberta and made monthly or sometimes bi-monthly visits to CYQT. He also spent some time in Thompson, Manitoba, and Montréal, Quebec, dealing with the company’s CARs Subpart 705 operations. He had limited interaction with the company’s CARs Subpart 704 flight crews and there was no indication that he had visited any of the company’s other remote bases leading up to the accident.
The company organizational chart shows the safety management system (SMS) manager reporting directly to the OM. While the organizational chart does not show a direct line of communication from the SMS manager to the AE, this relationship existed and was established in North Star Air’s COM.
The investigation was unable to establish the level of management oversight of the remote bases; the company was unable to provide any information regarding management team visits.
1.17.4 Safety management at North Star Air
1.17.4.1 General
An SMS is generally defined as a formalized framework for integrating safety into an organization's daily operations, including the necessary organizational structures, accountabilities, policies and procedures, so that “it becomes part of that organization's culture, and of the way people go about their work.”Footnote 30 While individual employees routinely make decisions about risk, an SMS focuses on organizational risk management, yet includes and supports the decision makers at the operational personnel level. An SMS is scalable and can be designed to meet the needs of a given operation in a way that respects the nature of the sector.
According to the International Civil Aviation Organization, the purpose of an SMS is
[…] to provide service providers with a systematic approach to managing safety. It is designed to continuously improve safety performance through: the identification of hazards, the collection and analysis of safety data and safety information, and the continuous assessment of safety risks. The SMS seeks to proactively mitigate safety risks before they result in aviation accidents and incidents.Footnote 31
1.17.4.2 Safety management at North Star Air
In late 2014, North Star Air introduced a voluntary hazard and incident reporting system and database to encourage employee engagement in safety. Such a system was not required by regulation.
In February 2016, the company submitted an SMS Procedures Manual to TC for approval in anticipation of the addition of CARs Subpart 705 operations to its air operator certificate (AOC). In accordance with the regulations, in order to obtain approval for a CARs Subpart 705 AOC, North Star Air was required to establish and maintain an SMS. Footnote 32
In February 2017, TC provided the company with a letter stating that its SMS Procedures Manual dated 19 February 2016 had “been reviewed and [...] approved in accordance with the Canadian Aviation Regulations (CARs) subsection 705.152(2).” This was despite the fact that 6 of the 17 SMS elements Footnote 33 were not fully implemented and that the company was not yet approved for 705 operations. There is no mechanism or regulation in the CARs that enables the Minister to approve an SMS for a 703 or 704 certificate holder.
During the year that it waited for TC’s approval, North Star Air continued trying to develop its SMS. However, in the summer of 2017, North Star Air’s SMS manager went on extended leave (approximately 4 months) and was not replaced. During this time, the SMS implementation stalled at North Star Air, and the 6 SMS elements that had not been fully implemented remained unimplemented. In the months leading up to June 2018, the SMS manager, with the assistance of the OM, began addressing the remaining requirements.
In May 2018, North Star Air had its AOC approved for CARs Subpart 705 operations. At the time of this 705 operations addition to North Star Air’s AOC, TC did not review North Star Air’s SMS manual, but relied on the approval issued in 2017.
A few months after North Star Air obtained its AOC for CARs Subpart 705 operations, the OM became aware that some of the company’s SMS requirements had not been fully implemented. To gain a better understanding of the gaps that existed, North Star Air hired a third-party consulting firm to review its SMS and make recommendations as appropriate. The consulting firm identified that, while the SMS was functioning, it fell short of TC’s SMS requirements. The consulting firm’s report indicated that North Star Air needed to review its SMS policies against the established regulatory expectations and that all procedures should be moved into a separate manual, making 2 manuals: 1 manual for SMS policies and 1 for SMS procedures. It also identified that North Star Air’s SMS should include a path showing what happens from the issuing of a safety report to the closing of that report. The report highlighted instances where risk assessments were incomplete, root-cause analyses were not performed, short- and long-term corrective action plans were missing, and timelines for follow-up audits were not set.
As a result of these findings, North Star Air took actions to address the issues identified, including hiring more staff to help manage its SMS and having the consulting firm re-write the company’s SMS manual.
1.17.4.3 Previous report of visual flight rules operations in instrument meteorological conditions
In December 2017, TC informed North Star Air’s OM that allegations had been received about company DC3-TP67s operating on multiple occasions under VFR in IMC and flying at inappropriate altitudes for the direction of flightFootnote 34 in the vicinity of CYMO. The reason TC informed North Star Air was to allow it the opportunity to conduct an internal investigation. The allegations were entered into the company’s SMS as report 4301 titled NSA Aircraft Not Remaining VFR. The OM conducted the investigation, including interviews with the pilots. In the root-cause analysis section of the report, the OM indicated “unable to determine due to inconclusive evidence.” The short-term corrective action plan indicated that the OM contacted all the DC3-TP67 captains verbally and via email about the concerns raised in the allegations and reminded them of the requirement to abide by the regulations. The FOs were excluded from this corrective action. The long-term corrective action plan indicated that the company would monitor for re-occurrence; however, the report did not outline how this monitoring would be done. In March 2021, the company’s SMS database indicated that the investigation into these allegations was ongoing.
1.17.4.4 Review of North Star Air safety management system
During this investigation, the TSB reviewed North Star Air’s SMS database. The investigation identified an incomplete root-cause analysis from a 2017 report, and the following in relation to reports from 2019:
- Inconsistent and/or incomplete short- and long-term corrective action plans
- Timelines for corrective action not being adhered to
- Inadequate follow-up to ensure effectiveness of corrective actions
- Hazards not being entered into the SMS
- Incomplete internal operational audits
1.17.5 Operational control system
North Star Air utilizes a Type C pilot self-dispatch system, in which “operational control is delegated to the pilot-in-command of a flight by the Operations Manager, who retains responsibility for the day-to-day conduct of flight operations.”Footnote 35 This delegation includes the responsibility for the pilot-in-command to make decisions to delay a flight when conditions are not suitable, and to change a flight plan, when, in their opinion, it is deemed necessary.
According to the COM, “each flight shall be conducted under an IFR flight plan, VFR flight plan, or flight itinerary, as appropriate.”Footnote 36 The purpose of filing a flight plan or flight itinerary is to ensure that, if the aircraft is overdue, the appropriate controlling agency or joint rescue coordination centre will be notified so that SAR alerting services can be initiated. The COM also stipulates that VFR flights “shall be conducted under VFR Flight Plan or VFR Flight Itinerary as appropriate, except where the flight is conducted within 25 nautical miles of the departure aerodrome.”Footnote 37 This mirrors the CARs requirements to file a flight plan or flight itinerary.Footnote 38
In order for a flight to meet the requirements of a company flight itinerary, the flight crew must provide the company flight followers all the details of the flight as listed in the Canada Flight Supplement.Footnote 39 Flight followers are provided this information through a company operational flight plan (OFP).
The company has designated flight followers, who monitor the progress of flights. Flight follower duties include checking weather, NOTAMs, and runway surface conditions at various stations; ascertaining aircraft maintenance status; and providing flight crews with the appropriate passenger/cargo manifest for the flight.Footnote 40 Flight followers are not responsible for assisting pilots with pre-flight preparation, such as the completion of the OFP.
Under Type C pilot self-dispatch system requirements, the pilot-in-command is required to pass along messages concerning departures, en-route stops, and arrivals to flight followers.Footnote 41 According to North Star Air’s COM, electronic flight tracking can be used by flight followers, as it was for the occurrence flight, as an alternative method to track flight departures, progress, en-route stops, and arrivals at destination.Footnote 42 These data were used by the company for flight tracking only, and not for operational quality assurance processes or SMS investigations.
On the day of the occurrence, the OFP was not submitted by the captain to the company flight followers.
1.17.6 Operational flight plans
According to CARs subsection 704.17(1), an OFP must be prepared in accordance with the operator’s TC-approved COM. Per North Star Air’s COM, OFPs shall be completed for every flight.
The occurrence OFP indicated that, at an estimated fuel burn rate of 950 pounds per hour, a total of 1420 pounds of fuel was required to complete the flight to CZPB under VFR.Footnote 43 This included a 30-minute fuel reserve, as required by regulation for flights conducted under VFR. According to the OFP, 2500 pounds of fuel was on board the aircraft and its take-off weight was 29 647 pounds, approximately 350 pounds below the maximum permissible take-off weight.Footnote 44 The OFP did not include any upper level wind values and it indicated an estimated time en route to CZPB of 56 minutes, based on a true airspeed of 190 knots and no-wind. The investigation determined that some of the company’s DC3-TP67 pilots, including the occurrence pilot, routinely omitted putting wind information in the OFP during pre-flight planning.
The investigation looked into IFR options on the day of the occurrence. Based on the weather at the time, Gillam Airport (CYGX), Manitoba, was the nearest suitable aerodrome that met the requirements as an IFR alternate aerodrome for CZPB. With the forecast winds along the route, an IFR flight to CZPB, with CYGX as an alternate aerodrome, would have required 2733 pounds of fuel to meet the regulatory fuel requirements.Footnote 45
The investigation determined that IFR options were often very limited due to the remoteness of the area and the lack of available alternate aerodromes. Some DC3-TP67 pilots would opt to file a VFR flight plan. Given that the fuel requirements are lower for a VFR flight than for an IFR flight, this allowed for significantly greater payload (i.e., cargo) and provided an operational advantage by reducing cockpit workload.
1.17.7 Visual flight rules operating minima
When conducting VFR flight, pilots are responsible for traffic separation and obstacle clearance. According to CARs section 602.115, in uncontrolled airspace, like the airspace surrounding CZPB, the minimum visual conditions for day VFR flight below 1000 feet AGL are as follows:
- The aircraft is operated with visual reference to the surface.
- Flight visibility is not less than 2 miles (unless otherwise authorized in an AOC).
- The aircraft is operated clear of cloud.
These requirements are echoed in North Star Air’s COM. With regards to the requirement to operate with visual reference to the surface, the COM states “when operating under VFR, the company aircraft shall not enter cloud at any time and be operated with visual reference to the surface of the earth.”Footnote 46
In addition to the above criteria, CARs section 704.23 stipulates:
Except when conducting a take-off or landing, no person shall operate an aircraft in VFR flight [...] during the day, at less than 500 feet AGL or at a horizontal distance of less than 500 feet from any obstacle.Footnote 47
North Star Air’s COM makes no reference to these minimum altitude and horizontal distance requirements. According to the CARs, IMC exist when the meteorological conditions are below the minima specified in Division VI of CARs Subpart 602. The purpose of the VFR operating minima is to establish a minimum level of safety. Humans “often incorrectly believe that change will be easy to detect.”Footnote 48 However, research has shown that the accuracy of pilot judgment is diminished in a degraded visual environment.Footnote 49 In poor weather, pilots may have difficulty assessing height, speed, and distance due to the lack of terrain features and reduced visual cues. Likewise, without additional references such as the horizon or other structures surrounding the runway (i.e., peripheral visual cues), a pilot’s judgment of attitude and height can also be diminished, and vertical or lateral deviations can go undetected.Footnote 50 As outside visual cues diminish, workload increases and pilots must progressively rely on their flight instruments, backing up visual manoeuvres by cross-checking flight instruments to ensure the accuracy of visual perception.Footnote 51,Footnote 52
Operating below the minimum altitude and horizontal distance requirements prescribed for VFR flight can lead to controlled flight into terrain.
1.17.8 Approach briefing
With regards to crew briefings, North Star Air’s standard operating procedures (SOPs) state that “for every approach and landing, the flight crew shall be briefed on the critical aspects of the procedure,”Footnote 53 and that “the approach should be briefed by the pilot who will fly the procedure.”Footnote 54 The SOPs indicate that the briefing is to follow the “AMORTS” format, where each letter stands for what the briefing must cover (Approach, Minima, Overshoot, Radios, Transition and Timing, Speeds and Supplementary remarks).Footnote 55
In the event that the pilots must deviate from the briefed procedure, North Star Air’s SOPs state that “the PF shall advise the PNF [pilot not flying] of the change.”Footnote 56
In this occurrence, the captain initially briefed the FO of his intention to conduct a visual approach to Runway 10, using the omni-bearing selector (OBS) for guidance. Once the captain realized that the planned approach was not going to work, he began manoeuvring the aircraft without briefing the FO as to his revised plan. During most of the low-level manoeuvring, the FO was unaware of the aircraft’s position and the captain’s planned course of action. It was not until the aircraft was north of CZPB that the FO became aware of where the aircraft was in relation to the airport and that the plan was to complete a manoeuvre similar to a left-hand circuit for landing on Runway 10.
Although icing was encountered during the descent to CZPB, the pilots did not discuss potential icing considerations (i.e., speed adjustments and the associated increase in required runway length).
1.17.9 Organization safety culture
1.17.9.1 General
Safety culture established within complex organizations is recognized as adaptive, evolving “gradually in response to local conditions, past events, the character of the leadership and the mood of the workforce.”Footnote 57 As a determinant of how people behave day-to-day, safety culture was defined as “the ‘engine’ that drives the system towards the goal of sustaining maximum resistance towards its operational hazards regardless of the leadership’s personality or [economic] concerns [faced by the industry].”Footnote 58 As a subcomponent within complex organizations, smaller groups of people who operate unique technology or who by design perform independently of the wider organization reside within a subculture, which is characteristically marked by a set of unique beliefs and interests related to safety.
Safety culture tacitly communicates expectations to new and existing members of the organization, affecting both how the work is accomplished and how fully members participate in an organization’s processes.
Safety culture is the way safety is perceived, valued, and prioritized in an organization. A positive and active safety culture reflects the actual commitment to safe operations at all levels (i.e., the vertical integration of information) in the organization. Safety culture has also been described as “how an organization behaves when no one is watching”Footnote 59 or "the way we do things around here.”Footnote 60 The organization’s safety culture is influenced by the values, attitudes, and behaviours of the stakeholders.
Establishing a positive safety cultureFootnote 61 has many challenges; however, it is a necessary first step in creating the values, attitudes, and behaviours required for operators to effectively manage the risks associated with their operations. These efforts and investments will eventually lead to a positive safety culture where unsafe practices are seen as unacceptable by all stakeholders and risks are managed to a level as low as reasonably practicable, improving the management of operational hazards.
The strength of an organization’s safety culture starts at the top and is characterized by proactive processes to identify, assess, and mitigate operational risks. If unsafe conditions are not identified, are allowed to persist or are not effectively prioritized by the operator, an increased acceptance of such risks can result at all levels of the organization, reducing the effectiveness of the operator’s SMS and its safety performance. The hierarchy of influences on the way work is accomplished in an organization has been described as the “4 Ps:”Footnote 62
- Philosophy: An organization’s philosophy provides a broad specification for how it wants to operate and it communicates values throughout the organization.
- Policies: An organization’s policies represent broad specifications of how management expects tasks to be carried out.
- Procedures: An organization’s procedures dictate the specific steps an individual should take to accomplish a task. They operationalize the philosophy and policies by indicating how work will be carried out.
- Practices: An organization’s practices represent what actually happens in day-to-day operations. In an ideal world, practices and procedures would be identical. However, in reality, practices may differ from procedures for any one of number of reasons.
One measure of a positive safety culture could be an alignment across the 4 Ps and efforts to identify any gaps and continuously improve. If the 4 Ps are not focused on safety and are not aligned to achieve the higher-level goal of safe operations, this may indicate that a negative safety culture is present within an organization.
1.17.9.2 Safety culture at North Star Air
The investigation determined that the captain and some other DC3-TP67 pilots demonstrated a result-oriented attitude and took great pride in completing scheduled flights and transporting as much cargo as possible. Although the captain had extensive experience on the DC3-TP67, the investigation could not determine how much experience he had flying in an IFR environment. The investigation determined that during the 2 months before the occurrence, all the flights conducted by the captain had been in accordance with VFR. However, for more than 10% of the flights, the weather at destination was reported to be conducive to IMC. Additionally, approximately 35% of the flights were conducted in weather where the pilots would have lost visual reference to the ground at some point during the flight.
It was also determined that the FO had previously conducted VFR flights in IMC with other captains at North Star Air and that the FO was comfortable with the occurrence flight operating under VFR, believing that it was acceptable under the regulations.
Previously, on 21 June 2019, at approximately 0140 Eastern Daylight Time, a North Star Air DC3-TP67 aircraft crashed shortly after taking off from Fort Hope Airport (CYFH), Ontario.Footnote 63 On board were 2 flight crew members, including the captain of the present occurrence, who was then acting as the PNF. The flight crew executed a forced landing on Eabamet Lake, Ontario. The aircraft sustained substantial damage. Neither pilot was hurt; however, they were not wearing the shoulder harness, which was identified to the company. At the time of this occurrence (A19C0145), no action had been taken by the company to address this issue.
1.18 Additional information
1.18.1 Transport Canada oversight
1.18.1.1 General
Transport Canada Civil Aviation, through its surveillance program, “verifies that enterprises are complying with regulatory requirements and that they have effective systems in place to ensure they comply with regulatory requirements on an on-going basis.”Footnote 64 The program includes “assessments, program validation inspections (PVIs) and process inspections [PIs].”Footnote 65
PVIs provide for system surveillance and an overall review of the company using sampling methods to verify whether the company has the systems in place to comply with regulatory requirements. PIs are inspections that focus on one or more specific processes. They verify whether the processes comply with regulatory requirements and work properly. The frequency of these inspections depends on factors such as the type of operations, turnover of key company employees, compliance history and nature of the findings.
1.18.1.2 Changes to Transport Canada’s approach to safety management system approvals and surveillance
In the mid-2000s, TC began requiring the implementation of SMS across different segments of commercial aviation. According to TC, SMS was introduced into the regulations to provide “an extra layer of protection to help save lives.”Footnote 66 To ensure the effectiveness of a company’s SMS, TC established an approval process. In 2005, TC issued the publication entitled Safety Management Systems: Implementation Procedures Guide for Air Operators and Approved Maintenance Organizations.Footnote 67 That document, which was cancelled in April 2017, stated that:
Organizations applying for an Air Operator or AMO [approved maintenance organization] Certificate on or after the date the SMS regulations come into force must incorporate all the SMS components and elements as part of their initial application for certification. Existing certificate holders or new entrants, whose application is dated and accepted by Transport Canada prior to the date the SMS regulations come into force, will have the opportunity to utilize the exemption.
Post certification audits for new entrants will be scheduled by the applicable Transport Canada Centre/Office of Primary Interest and will include an assessment of the SMS.Footnote 68
In addition, in October 2007, TC issued Staff Instruction (SI) 107-002 entitled Safety Management System (SMS) Certification Procedures for New Organizations. In June 2009, TC published Issue 02 of that SI, which defined an assessment as “a process comprised of a documentation review and on-site review of the entire organization in order to determine if the safety management system is documented, in place and effective.”Footnote 69 It also stated: “Twelve months following initial certification a new organization shall undergo a full SMS assessment using the assessment procedures contained in the SI SUR-001.”Footnote 70
SI 107-002 was cancelled in 2015, and TC stopped conducting the assessments that were previously required for newly certificated operators within 12 months of the initial certification.
Effective 01 April 2018, TC implemented changes to its approach to surveillance with the introduction of its Surveillance 2.0 program. One of the most notable changes associated with Surveillance 2.0 was that TC ceased using systems-level surveillance activities (i.e., assessments and PVIs) as a primary means of surveillance. Instead, the PI became the primary surveillance activity used to determine compliance and risk. Under Surveillance 2.0, assessments would no longer be used as a planned surveillance activity.Footnote 71 TC considered that process inspections serve as an effective performance indicator that can be used to detect systemic breakdowns, and indicated that in the event a systemic breakdown is discovered during process level surveillance, reactive surveillance can be initiated to further explore and address those concerns. According to SI SUR-001 (Issue 08), “assessments will be conducted as a reactive surveillance activity only when invoked by the Oversight Advisory Board (OAB).”Footnote 72,Footnote 73
1.18.1.3 Oversight of North Star Air
In September 2016, TC conducted a PVI on North Star Air, which at the time was operating solely under CARs Subpart 703. The PVI identified 5 findings of non-compliance related to the company’s quality assurance program and operational control. North Star Air addressed these findings and TC closed the PVI in December 2017. Following this PVI, the company was put on a 2-yearFootnote 74 planned surveillance interval.Footnote 75
On 14 December 2017, TC received allegations that North Star Air’s DC3-TP67 aircraft were flying on multiple occasions in IMC without an IFR clearance around CYMO. The details of the allegations were provided to North Star Air for internal investigation.
In February 2018, TC conducted a reactive PI on North Star Air in response to the de-icing issues related to an accident in March 2017, and the allegations received regarding flights in/out of Moosonee. As part of this PI, TC also conducted 3 flight inspectionsFootnote 76 on the DC3-TP67s. These flight inspections, which had been announced in advance to the company, were deemed “uneventful” by TC inspectors. The February 2018 PI resulted in no findings of non-compliance, and no further action was taken by TC in response to the allegations of non-compliance received in December 2017.
In May 2018, North Star Air was approved for CARs Subpart 705 operations. However, since it was no longer required to assess newly certificated operators within 12 months of initial certification, TC did not conduct an assessment of North Star Air’s SMS to determine if the company was able to effectively manage the risks associated with adding CARs Subpart 705 operations to its existing operations.
In November 2018, TC conducted another PI on North Star Air, looking at the company’s CARs subparts 703, 704, and 705 flight dispatch process and SMS reactive process. This PI resulted in 1 operational finding related to North Star Air’s COM. No findings were issued against North Star Air’s SMS. TC’s PI worksheets indicate that the reporting process and reactive reports, including implementation of corrective action plans, were reviewed and verified, and no issues or gaps were identified.
At the time of the November 2018 PI, the SMS report related to the 2017 VFR in IMC allegations submitted to TC had been open for almost 1 year. However, according to TC, North Star Air’s SMS investigation dated prior to North Star Air’s 705 operational approval was not subject to TC’s action since the investigation was initiated prior to the SMS regulatory requirement.
On the day of the occurrence, TC was conducting a scheduled PIFootnote 77 at the company’s Thunder Bay base. The letter dated 01 November 2019 that TC had sent North Star Air to inform them of the upcoming PI indicated that the inspection would include an evaluation of the following areas of operation:
- Operational dispatch
- Quality assurance program
- Technical dispatch
- Maintenance release
- Reactive process
- Proactive process
- Investigation and analysis
- Risk management
As a result of the occurrence, the scope of the December 2019 PI was expanded, and the inspection concluded in early January 2020. The PI identified 6 findings of non-compliance related to the following aspects of North Star Air’s operation:
- Quality assurance program (CARs Subpart 706)
- Defect rectification and control procedures (finding related to CVR on occurrence aircraft)
- Flight and duty time monitoring (CARs Subpart 705)
- Pilot training files (CARs Subpart 705)
- Weight and balance process (CARs Subpart 705)
- Pilot qualifications (CARs Subpart 705)
With the exception of the finding related to the CVR issue, no findings were directly related to North Star Air’s CARs subparts 703 or 704 operation. In addition, there were no specific findings related to the company’s SMS.
According to TC’s post-PI notes, the January 2020 PI discovered the following:
- Examples of pilots flying with expired aircraft type currency qualifications
- An instance of training flight documentation being falsified
- DC3-TP67 crews conducting flights with the auto-feather system not working properly
- A documented case of an aircraft taking off above the maximum permissible weight
- Instances of flight timings being falsified to cover up duty day exceedances
- A substantial increase in the number of occurrences, incidents, and accidents in the last 5 years
- 3 accidents involving the DC3-TP67 fleet, 1 of which resulted in the aircraft being written off
- An issue with the company culture, including a belief that “the job must get done regardless of weather, limitations, or regulations”Footnote 78
1.18.1.4 TSB Recommendation A16-13
Transportation companies have a responsibility to manage safety risks in their operations. Compliance with regulations can only provide a baseline level of safety for all operators in a given sector. Since regulatory requirements cannot address all risks associated with a specific operation, companies need to be able to identify the hazards and mitigate the associated risks specific to their operation. However, regulators must have assurances that companies possess the ability to effectively manage safety.
Following a controlled flight into terrain accident involving a Sikorsky S-76 helicopter conducting a night-time departure on 31 May 2013 in CYMO,Footnote 79 the TSB recommended that
the Department of Transport conduct regular SMS assessments to evaluate the capability of operators to effectively manage safety.
TSB Recommendation A16-13
In September 2021, in its most recent response, TC indicated that it is:
- developing oversight tools to more effectively communicate non-compliances to Canadian Aviation Document holders. This is being monitored by the Finding Review Committee, which reviews all findings entered by TC inspectors to ensure findings related to violations of rules-of-conduct are clearly documented. This will assist in building an aviation record and in identifying re-occurrence, which can be evidence of a systemic failure used to trigger system-level surveillance, enforcement action, and/or certificate action.
- seeking to improve the effectiveness of SMS oversight, which it acknowledges is a current weakness in the program. TC is developing a proposal for effective safety oversight of management systems, which is currently undergoing internal review and consultation. This initiative is planned to be completed over the next 2 years.
In its March 2022 reassessment of TC’s response, the Board indicated that it is encouraged by TC’s efforts to update and improve its surveillance methodology; however, the Board is concerned that, as per TC’s surveillance planning and procedures, SMS assessments are only conducted as a reactive surveillance tool. According to TC’s Staff Instruction (SI) SUR-001 - Surveillance Procedures, assessments “will be conducted as a reactive surveillance activity only invoked by the Oversight Advisory Board (OAB).”Footnote 80 In addition to TC’s 4 categories of surveillance activities (system vs process level, targeted vs compliance level inspections), the Board continues to recommend the use of regular SMS assessments as part of TC’s planned (and reactive) surveillance activities to ensure that SMS are evaluated regularly and updated based on results of integrated and fulsome evaluations and to ensure that an operator has the ability to effectively manage safety. As TC indicated it will not be conducting regular SMS assessments, the risks associated with the safety deficiency identified in Recommendation A16-13 remain. Therefore, the Board considered the response to Recommendation A16-13 to be Satisfactory in Part.Footnote 81
1.18.2 TSB Watchlist
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada’s transportation system even safer. The following Watchlist 2020 issues are relevant to this occurrence.
1.18.2.1 Safety management
An SMS is an internationally recognized framework that allows companies to identify hazards, manage risk, and make operations safer—ideally before an accident occurs. Although the issue of safety management has been on the Watchlist since 2010, TSB investigation reports continue to note various deficiencies and concerns.
There has been little progress to extend the application of SMS beyond CARs Subpart 705 operators. SMS requirements still do not apply to CARs subparts 702, 703, and 704 operators, flight training units (which operate under CARs Subpart 406), or non-certified aerodrome operators, although some have implemented SMS on a voluntary basis. Combined, CARs subparts 702, 703, and 704 operators make up over 90% of all Canadian commercial air operators. As a result, TC does not have assurances that these operators are able to effectively manage safety. Many of these are smaller companies and, without the benefit of an SMS, they continue to miss opportunities to improve the safety of their operations. The likelihood of more fatalities and serious injuries therefore remains high. Footnote 82
Although there has been some progress in addressing this issue, that progress has been piecemeal. At its Canadian Aviation Safety Collaboration Forum in March 2022, TC indicated that it plans on starting consultation for incorporating SMS for CARs subparts 406, 702, 703, 704, and 573 operators not currently required to have SMS. TC plans to publish the amendments in the Canada Gazette, Part II in late 2025.
ACTIONS REQUIRED Safety management will remain on the Watchlist for the air transportation sector until
|
1.18.2.2 Regulatory surveillance
All transportation operators are responsible for managing the safety risks within their organizations and operations. Regulations help by providing operators a guiding framework and stipulating certain minimum requirements and levels of safety. However, it is up to operators to meet those requirements; it is TC’s responsibility to inspect and audit operators to confirm that they are compliant with these regulations and that minimum levels of safety are met.
However, TC’s surveillance has not consistently proven effective, and the TSB has noted various deficiencies and concerns over the years.
TC is not always effective at identifying gaps in a company’s safety management processes and intervening in a timely manner. Moreover, at times, there has been an imbalance between the use of traditional inspections to verify compliance with regulations, and auditing company safety processes to assess if they are working.
Canadians travelling on and using services provided by TC-inspected and -approved transportation companies expect that these operations are safe and that they meet the basic regulatory requirements — and if not, that TC will take proactive steps so that operators are returned to compliance in a timely manner.
However, when this does not happen and surveillance measures are not sufficient to identify safety deficiencies—or if TC is unable to intervene to ensure that operators take appropriate corrective actions—then unsafe or non-compliant operating practices may continue. As a result, minimum levels of safety may not be met, putting in jeopardy the safety of people, property, and the environment.
In 2019, TC developed and implemented guidance, tools, and training to improve the quality of findings produced during surveillance activities, as well as the decisions made related to the oversight of commercial aviation, and its risk-based planning methodology.
|
ACTIONS REQUIRED Regulatory surveillance will remain on the Watchlist for the air transportation sector until TC demonstrates, through surveillance activity assessments, that the new surveillance procedures are identifying and rectifying non-compliances, and that TC is ensuring that a company returns to compliance in a timely fashion and is able to manage the safety of its operations. |
1.18.3 Crew resource management best practices
1.18.3.1 General
This section will highlight some of the industry’s accepted crew resource management (CRM) best practices as they apply to pilot decision making, situational awareness, and crew communication.
1.18.3.2 Pilot decision making
Effective decision making involves gaining an accurate understanding of the situation, appreciating the implications of the current situation, formulating one or more plans and contingencies, then implementing a course of action. Equally important is the crew's ability to recognize changes in their situation and to reinitiate the decision-making process to ensure that changes are accounted for, and plans modified accordingly. Failure to adequately consider the potential implications of a situation increases the risk that a decision will produce an adverse outcome that may result in an undesired aircraft state. A number of factors affects this process.
An important aspect of the decision-making process is the concept of mental models.Footnote 83 An individual’s mental model is largely dependent on the person’s understanding of the circumstances, expectations about the future, and past experience. People use their past experience and their knowledge to rapidly categorize the situation they are experiencing and make judgments.Footnote 84 As an individual develops experience in novel situations, those situations and the course of action selected create potential matches for future decisions. This can be both positive and negative, depending on situational context. Just as successful positive behaviours will have a reinforcing effect, if a higher-risk decision results in a positive outcome, it can cause an individual to become more relaxed toward higher-risk behaviours, making it more likely that they will repeat these behaviours in the future.Footnote 85,Footnote 86 In some circumstances, this tendency can lead to decisions based on an inaccurate or incomplete understanding of the situation, of the implications of the situation, or of alternative courses of action available.
Studies show that “pilots tend to underestimate the likelihood of loss of control and overestimate their ability to continue to control the aircraft if visual references are lost.”Footnote 87 Similarly, pilots who deliberately accept increased risk (e.g., operating in a degraded visual environment) tend to have a greater risk tolerance, experience less anxiety in that situation, and perceive the risk as being relatively low.Footnote 88 A misjudgment of risk may lead to inappropriate decisions and at-risk behaviour.
Organizational factors can also directly or indirectly influence pilot decision making. SOPs directly support pilot decision making by providing pilots with what their company considers to be predetermined successful solutions for specific situations. The SOPs establish expectations with regard to acceptable levels of risk for pilots to use as a frame of reference when required to make an operational decision.
Pilot decision making can also be influenced by the norms that may develop within an organization. In an effort to meet organizational goals, well-intended behaviours that incrementally increase risk may emerge over time. For this reason, it is important that organizations reinforce the importance of adherence to SOPs and identify, through their SMS, informal practices that increase risk level.Footnote 89
In a crew environment, every effort should be made to align mental models. If the crew is unable to align mental models due to differences in personality, communication style, or authority gradient, critical information may not be accounted for when considering the potential implications of a situation and during the formulation of plans and contingencies. This will result in sub-optimal decision making, and could produce an unacceptable level of risk.
1.18.3.3 Situational awareness
Situational awareness is a critical component of decision making. As a construct, situational awareness is defined as “the perception of the elements in the environment within a volume of time and space, the comprehension of their meaning, and the projection of their status in the near future.”Footnote 90 All 3 processes involve information-processing stages at which shortcomings may occur, and that may result in incomplete or inadequate situational awareness. Several factors and biases such as context, knowledge, experience, training, and individual physiology can influence situational awareness.
Flight crew actions need to be based on a common understanding of the current state of the aircraft, the intended flight plan, and the threats to these activities in order to perform in a coordinated, efficient, and safe manner. This common understanding between the crew members is referred to as team or shared situational awareness.Footnote 91,Footnote 92 When team situational awareness is high, crews are better able to effectively anticipate and coordinate their actions toward achieving their common goal.
Shared situational awareness is developed and maintained by a crew through a number of discrete and continuous behaviours. Discrete behaviours include flight planning, in-flight briefings, and identification of key points in the flight, such as attaining minimum altitudes. These activities are planned checkpoints to describe current state and future plans and to provide an opportunity for setting, and checking that all crew members have, the same understanding.
Continuous behaviours include threat and error management, callouts of changes of aircraft state and instrument setting or mode, and communication of changes to plans. These behaviours ensure that information and state changes are communicated between crew members to update the shared situational awareness on an ongoing basis. All of these are aspects of CRM that enable effective crew interactions. Such continuous behaviours are influenced by the training and operational approach taken by operators.
1.18.3.4 Attentional narrowing
Pilots operate in a complex environment in which they have to monitor multiple sources and types of information. Because human attention is limited, pilots must prioritize the different information carefully to ensure they do not overlook relevant information.
Workload is a function of the number of tasks that must be completed within a given amount of time. If the number of tasks to be completed increases, or if the time available to complete those tasks decreases, then workload increases. An increase in workload places greater cognitive demands on the pilot, which can adversely affect the pilot’s ability to perceive and evaluate cues from the environment, and may result in attentional narrowing.Footnote 93,Footnote 94
Attentional narrowing occurs when
the individual is focusing all conscious attention on a limited number of environmental cues to the exclusion of others of a subjectively equal or higher detectability, or of a more immediate priority.Footnote 95
The relevant cues may be available; however, individuals experiencing high workload tend to limit their attention to the stimuli they perceive to be most important or most relevant to the task at hand.Footnote 96 Likewise, attentional narrowing is more likely to occur when there is a high motivational intensity or a heightened state of arousal, or stress.Footnote 97 If a pilot places greater importance on external cues, it can draw their attention away from the flight instruments, resulting in degraded situational awareness and potentially allowing deviations to go undetected.Footnote 98,Footnote 99
In a study involving 15 accidents, inaccurate perception accounted for 72% of the breakdowns in situational awareness.Footnote 100 Because attentional narrowing can lead to inaccurate perception, it represents a significant risk in complex, high-risk domains such as aviation.Footnote 101
To reduce the likelihood of attentional narrowing, pilots must continually evaluate their situation. This implies scanning relevant sources of information, such as cockpit displays, to ensure an accurate perception of the situation and to identify whether the plan is working out as expected or whether a change in the plan is required. In a multi-crew aircraft, communication from other crew members can be critical in recognizing and overcoming the effects of attentional narrowing.
1.18.3.5 Crew communications
In order to align mental models, increase crew situational awareness, and optimize the decision-making process, crews must be highly effective communicators and be comfortable providing and receiving feedback. However, these communication skills require practice and reinforcement to be effective, particularly when safety margins are reduced or if there is a significant difference in experience levels. In the case of a junior FO, paired with a senior captain, there may be a natural tendency for the FO to be reluctant to speak up, in any way, for fear of being wrong or for giving the impression that they are in some way questioning the actions of the much more experienced captain. This is sometimes referred to as a strong trans-cockpit authority gradient. An authority gradient is attributable to differences between the pilots, such as age, experience, rank of crew members, and the manner in which one or both crew members explicitly or implicitly place emphasis on these differences.Footnote 102
Modern CRM programs highlight barriers to effective communication, such as trans-cockpit authority gradient, and provide multiple communication strategies that can be drawn upon depending on the severity of the situation, the time available, and the other person(s) involved in the communication process. In particular, they provide FOs with strategies when trying to raise a concern to a captain, and they provide captains with strategies to recognize when an FO is uncomfortable or is trying to raise a concern. In order for these strategies to be effective, flight crews need to be provided with realistic opportunities to practice these skills and receive feedback, so that the theory can be put into practice. Otherwise, flight crews may have difficulty employing these CRM skills when they are most needed in the aircraft. A common strategy often used during pre-flight briefings by experienced captains to combat trans-cockpit authority gradient is to explicitly encourage a more junior FO to speak up whenever they feel uncomfortable, or are unsure of the plan. Setting clear expectations and sending a signal to the FO that their feedback is welcomed and encouraged increases the likelihood that the less-experienced individual will feel confident to speak up.
1.18.3.6 Crew resource management training at North Star Air
TSB investigators reviewed North Star Air’s initial 1-day CRM course. The training is conducted over the course of 8 hours and includes all required elements outlined in subsection 724.115(38) of the Commercial Air Service Standard 724.
A large portion of North Star Air’s initial CRM course originated from TC's CRM training package,Footnote 103 introduced in the 1990s. North Star Air’s initial CRM program focuses primarily on awareness, rather than teaching practical CRM skills in an operational setting. This is consistent with earlier-generation CRM programs that were primarily aimed at changing attitudes toward CRM. North Star Air’s initial CRM program does include some modern CRM elements, such as discussions related to threat and error management or the surprise and startle effect, that are covered in Advisory Circular (AC) 700-042.Footnote 104
The review of North Star Air’s initial CRM training program identified the following elements, given their potential significance to the occurrence:
- The presentation identified the following elements as at-risk behaviours:
- Flying in bad weather
- Taking shortcuts
- Complacency due to overconfidence or because of a sense of security when flying with an experienced crew member
- Overconfidence and ignoring consequences, which can adversely affect judgment
- The presentation stated that pilots should speak up and escape to a safe altitude:
- if there has been a loss of situational awareness;
- if they do not understand what is happening; or
- if they have a concern and want clarification.
North Star Air’s initial CRM course ends with a case study using TSB Aviation Investigation Report A11H0002, which is about a Boeing 737-210C that crashed during final approach to Resolute Bay Airport (CYRB), Nunavut.
According to North Star Air, the company does not have a separate CRM recurrent training program. The company’s 4-hour recurrent CRM training is conducted in accordance with AC 700-042, and uses training material from the company’s initial CRM course.
North Star Air uses designated company CRM trainers, selected based on their experience in a training capacity. None of the company’s CRM trainers have completed formal CRM facilitator training, nor are they required to by regulation.
1.18.4 Adaptations
Adaptations are intentional deviations from formalized rules or procedures. They are often a result of not fully understanding the purpose of a rule or procedure, not anticipating the potential consequences of an adaptation, or a perception that the existing procedures are unnecessary, difficult, time-consuming, unworkable, or simply not enforced. When adaptations are performed with no negative consequences, they can persist and become routine and standard practice. In doing so, the adaptation becomes normal behaviour and it can erode the safety margins created by rules and procedures.
People rarely follow rules or instructions precisely, for reasons and in ways that make sense to them given their circumstances, knowledge, and goals.Footnote 105
While a company prescribes policies and procedures to set boundaries for safe operations, individuals may push the boundaries to become more productive or obtain some other benefit. This can lead to adaptations of procedures and to a shift beyond the prescribed boundaries described in the procedures, toward unsafe practices.Footnote 106 Without intervention, the communication of successful adaptations between crew members tends to lead to the spread of adaptations throughout an organization.
Such adaptations are unlikely to be recognized as deviations by those within the group employing them. The adaptations slowly become normal behaviour, and the risk associated with them is unlikely to be recognized.Footnote 107
1.18.5 Controlled flight into terrain
1.18.5.1 General
Controlled flight into terrain (CFIT) occurs “when an airworthy aircraft under the control of the flight crew is flown unintentionally into terrain, obstacles, or water, usually with no prior awareness by the crew.”Footnote 108
In the early 1990s, CFIT was the primary cause in fatal aircraft accidents worldwide. In the following decades, operators and regulators made strides to reduce accidents of this type. Many new technologies have been introduced, such as terrain awareness and warning systems, enhanced ground proximity warning systems, global navigation satellite systems, digital terrain databases, and moving map displays with graphic depiction of the aircraft’s position relative to terrain. Also, improved training is available, such as CFIT awareness training, CFIT escape manoeuvre training, and enhanced CRM training with threat and error management. When combined, these advances have reduced the number of CFIT accidents, to the point where in-flight loss of control has surpassed CFIT as the primary cause of fatal accidents for aircraft over 5700 kg.Footnote 109
In Canada, there has also been a reduction in CFIT accidents. A TSB statistical review of CFIT accidents in Canada was conducted for the period 1992 to 2019.Footnote 110 The review looked at accidents where Canadian-registered aircraft in commercial flights operating under VFR continued into IMC and a CFIT accident occurred.
In the 28-year period examined, the following accident numbers were noted:
- 60 accidents involved commercial operators (64 fatalities); of those,
- 34 accidents involved airplanes (45 fatalities), and
- 26 accidents involved helicopters (19 fatalities).
A correlation testFootnote 111 was used to determine whether there was any trend in this type of accident over the 28-year period. The number of accidents of commercial airplanes showed a decreasing trend over 28 years, while the numbers of accidents involving commercial helicopters did not show statistically significant trends. Most of the overall decrease in number of accidents took place during the first 14 years of this period (1992 to 2005), with no trend in the period 2006 to 2019.
1.18.5.2 Controlled flight into terrain training at North Star Air
Transport Canada’s standards require companies operating under CARs Subpart 704 and conducting IFR flights to provide training on the avoidance of CFIT.Footnote 112 This training is to consist of:
- factors that may lead to CFIT accidents and incidents;
- operational characteristics, capabilities, and limitations of ground proximity warning systems if applicable;
- CFIT prevention strategies;
- methods of improving situational awareness; and
- escape manoeuvre techniques and profiles applicable to the airplane type.
The North Star Air DC3-TP67 training program met this requirement by providing DC3-TP67 pilots online training.Footnote 113 The captain had last received CFIT awareness training in February 2019 and the first officer in April 2019.
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
2.1 Introduction
There was no indication that an aircraft system malfunction contributed to this occurrence. As a result, the analysis will address the human, operational, and organizational factors that contributed to the occurrence.
The analysis will focus on pilot decision making and the sequence of events that led to the collision with terrain during low-level flight. It will also examine the safety culture, supervision, and safety management at North Star Air Ltd. (North Star Air). In addition, it will address issues related to crew resource management (CRM), regulatory oversight, flight planning, the use of cockpit restraint systems, cockpit voice recorders (CVRs), and emergency locator transmitter (ELT) design standards.
2.2 Pilot decision making
The pre-flight weather information available to the captain indicated low ceilings and visibilities reduced in light snow would be encountered on the route from Red Lake Airport (CYRL), Ontario, to Sachigo Lake Airport (CZPB), Ontario. Visual flight rules (VFR) flight in such conditions, especially for a multi-engine, fixed-wing aircraft, would leave very little safety margin to deal with in-flight challenges such as avoiding terrain and obstacles, diverting, dealing with an emergency, etc. However, the risks inherent with a VFR flight along this route in such conditions can be mitigated by operating under instrument flight rules (IFR), greatly enhancing the safety margins.
The investigation determined that, based on the aircraft fuel and cargo load, a suitable alternate aerodrome would have been available for the occurrence flight to be conducted under IFR if an additional 233 pounds of fuel had been uploaded to the aircraft. However, because of the captain’s history of operating under VFR, consideration was not given to determining what IFR options existed prior to departing CYRL. Instead of looking for IFR options, the pilots departed on a VFR flight, without having filed the flight plan or flight itinerary required by regulation and the company’s operations manual.
Shortly after takeoff from CYRL, the aircraft entered, and climbed above, the cloud layers before reaching the planned cruising altitude to CZPB. This action was not in accordance with the regulations governing VFR flight, which require the aircraft be operated clear of cloud and in visual contact with the surface at all times. As the aircraft approached CZPB, the pilots initiated a descent through the cloud layers by reference to their flight instruments.
Once the aircraft broke out of cloud at very low level, the aircraft was not in a position to land and the captain flew a large low-level 360° turn, at a height as low as 100 feet above ground level (AGL), in order to remain clear of cloud. This low-level manoeuvring occurred approximately 400 feet below the minimum altitude required for a commuter flight conducted under VFR in uncontrolled airspace.
After completing the 360° turn, the aircraft was once again not in a position to join the final approach and land on Runway 10. Again, the captain continued operating visually by conducting a low-level manoeuvre similar to a left-hand circuit, which brought the aircraft in close proximity to a significant obstacle (a 150-foot tall tower), in conditions that were below the minimum required meteorological conditions for VFR flight.
As outlined above, a series of operational decisions that were made during this occurrence resulted in increased risk levels. The investigation determined that the captain had a history of conducting VFR flights in instrument meteorological conditions (IMC). Over time, the pilot’s repeated success conducting these types of operations resulted in a reduced perception of risk, which contributed to his willingness to deviate from regulations, despite the well-documented risks associated with operating under VFR in IMC.
Finding as to causes and contributing factors
The decision to depart on, and continue, a VFR flight in IMC was influenced by a distorted perception of risk resulting from successful past experience in similar situations.
2.3 Collision with terrain during low-level flight
In the absence of CVR and flight data recorder information, the investigation focused on the meteorological conditions present and the aircraft’s flight profile during the final moments of the flight. The investigation considered the possibility that the aircraft, which was operating at extremely low altitudes, experienced an aerodynamic stall, potentially aggravated by the presence of ice. An in-depth performance analysis concluded that, although the stall margin decreased immediately following the turn from downwind, the stall margin improved as the aircraft descended to near tree-top level in the final moments before the impact. This reduced likelihood of a stall in the final moments is supported by the absence of any audible stall warnings during the flight. Because it is unlikely that a stall occurred, the rest of this section will consequently outline the most likely scenario of what did occur.
After the aircraft’s descent from the enroute altitude, the captain conducted a large low-level visual 360° turn in IMC at altitudes considerably lower than the minimum en-route altitude for VFR under Canadian Aviation Regulations (CARs) Subpart 704 and the minimum descent altitude for an instrument approach to Runway 10. Then, at heights that varied between 150 and 225 feet AGL, he flew a circuit-type manoeuvre for landing on Runway 10. As a result, from the moment that the aircraft descended below the clouds in anticipation of a visual approach, the flight was being conducted at a significantly elevated risk level, outside the safety envelope provided by the regulations. Operating below the minimum altitude and horizontal distance requirements prescribed for VFR flight can lead to controlled flight into terrain (CFIT). At these low altitudes in IMC, the pilots would have had very little time to respond to any unexpected obstacles.
During the unbriefed, ad hoc circuit-type manoeuvre to Runway 10, the aircraft remained within 0.4 nautical miles (NM) of the runway, passing within 0.12 NM of a 150-foot tall tower. As a result, the aircraft, which had operated at low altitude for an extended period of time, was being manoeuvred at a height and a horizontal distance from obstacles that represented a significant risk of collision.
As the aircraft passed abeam the threshold of Runway 10, the captain, seated in the left-hand seat, entered a low-level turn for the final approach. After 2 previous unsuccessful attempts to position the aircraft for landing on Runway 10, it is likely that the captain, who had a history of completing VFR flights in poor weather, was highly motivated to carry out the approach to landing. The captain’s attention was likely fixated on outside references, trying to locate, and position the aircraft for landing on, Runway 10. The high workload resulting from the lack of visual cues during the turn from the downwind leg due to the low visibility, low clouds, and snow-covered terrain could have contributed to attentional narrowing, making it difficult for the captain to accurately assess height, speed, and distance. However, because of previous experience in similar weather conditions, the reduced safety margins went undetected, and the captain continued the attempted visual approach.
Data from the automatic dependent surveillance-broadcast (ADS-B) suggests that the captain was unaware of the aircraft’s exact position relative to Runway 10, possibly believing that the aircraft was lined up for the approach. Unbeknownst to the captain, the aircraft, which had been operating at low level for several minutes, continued descending, making contact with the trees and the terrain, in a more or less level attitude, sliding approximately 350 feet. During this crash sequence, the pitot-static tubes, which inputs to the ADS-B signal, was compromised due to impact with trees.
Finding as to causes and contributing factors
The captain likely experienced attentional narrowing while carrying out a high-workload visual approach at very low altitude in IMC. This most likely resulted in an inadvertent but controlled descent that was not detected until the aircraft collided with terrain.
2.4 North Star Air Ltd.
2.4.1 Safety culture at North Star Air
The investigation gathered information that may be indicative of inconsistency within the safety culture at North Star Air. For example, on the day of the occurrence, the captain did not file a flight plan or flight itinerary, which is contrary to the CARs and North Star Air’s company operating procedures.
More significantly, the investigation also determined that some DC3-TP67 pilots at North Star Air had developed casual attitudes toward regulatory compliance that resulted in routine adaptations eroding safety margins, and that they would routinely operate VFR in IMC given that:
- IFR options were often very limited due to the remoteness of the area and the lack of available alternate aerodromes;
- the fuel requirements are lower for a VFR flight than for an IFR flight, which allows for significantly greater payload (i.e., cargo); and
- this provides an operational advantage by reducing flight time and cockpit workload.
This practice of flying VFR in IMC eroded safety margins. In particular, it placed pilots at significant risk owing to:
- the potential for loss of control and/or CFIT because of low ceilings and poor visibility;
- reduced diversion options in case of deteriorating weather conditions because of alternate aerodromes not being factored into flight planning; and
- the decision to opt for less fuel in order to take more cargo, which meant less fuel being available for diversion, possibly leading them to push the weather because of the lack of other options.
Additionally, in 2017, the allegations about North Star Air DC3-TP67 aircraft operating on multiple occasions under VFR in IMC had been raised to Transport Canada (TC), and the company reminded DC3-TP67 pilots verbally and via email about the VFR regulations. However, some DC3-TP67 pilots continued to conduct VFR flights in IMC.
As an operational group with its own subculture, some DC3-TP67 pilots adopted unsafe practices that were operationally advantageous, such as conducting VFR flights in IMC. The routine success of these practices led to the perception that they were safe.
As seen in this occurrence, after checking the weather, the pilots decided to conduct a VFR flight in IMC, even though both pilots were IFR-rated and the flight could have been conducted with the planned cargo load under IFR. At the time of the occurrence, the persistence of this unsafe practice, which deviated from regulatory requirements and had been previously identified, was an indication of a negative safety culture within North Star Air’s DC3-TP67 operation.
Finding as to causes and contributing factors
The result-oriented subculture of some North Star Air’s DC3-TP67 pilots, which emphasized mission completion over regulatory compliance, resulted in VFR flights, such as the occurrence flight, being conducted in IMC.
2.4.2 Supervision at North Star Air
At North Star Air, the operations manager (OM) is responsible for the supervision of flight operations. The chief pilots (CP), who report to the OM, are responsible for the supervision of flight crews. At the time of the occurrence, the OM was located at North Star Air’s headquarters in Thunder Bay, Ontario. The CP for 704 and 705 operations worked remotely from Alberta and made monthly or sometimes bi-monthly visits to Thunder Bay. He also spent some time in Thompson, Manitoba, and Montréal, Quebec, dealing with the company’s CARs Subpart 705 operations. He had limited interaction with the company’s CARs Subpart 704 flight crews and there was no indication that he had visited any of the company’s other remote bases leading up to the accident.
There was no operational management presence and no day-to-day direct supervision of DC3-TP67 flight operations and flight crews at the company’s remote bases, nor is it required by regulation.
The absence of on-site supervision increases the risk that deviations from company procedures and/or regulations may go undetected. As a result, companies that do not have direct on-site supervision of flight operations must take adequate steps to ensure that operations are conducted safely, and in accordance with the regulations. At North Star Air, the company employed a Type-C pilot self-dispatch system, which relied solely on flight crew experience to ensure safe operations and regulatory compliance. Although the company operations manual outlined the requirements for VFR flight, the absence of direct supervision meant that company pilots had considerable latitude when it came to making operational weather-related decisions. Over time, a subculture, which included non-compliance with VFR regulations, developed amongst some DC3-TP67 pilots and went undetected by the company management team.
Finding as to risk
If minimal supervision of flight crews occurs within a company’s flight operation, there is a risk that previously identified unsafe or non-compliant practices will persist.
2.4.3 Safety management
North Star Air operates under CARs Subpart 705 and is therefore required by regulation to have a safety management system (SMS). The expectation is that companies requiring an SMS will have, or will implement, systems to proactively manage risk. This can include a variety of different means, including developing new procedures, increasing supervision and communication, or leveraging technology. In the case of North Star Air, for example, the company had readily available electronic flight tracking data that provided detailed information about routes and altitudes flown on previous flights. This data permitted company management to proactively and reactively identify issues related to compliance with regulations and company procedures, as seen in both the 2017 allegations of operating VFR in IMC and in this occurrence. However, contrary to what would be expected of an SMS enterprise, North Star Air did not use this information as a means of monitoring its DC3-TP67 operation to ensure flights were being conducted in accordance with the regulations. This represents a missed opportunity to identify potentially unsafe flight operations, which would also provide an indication of the state of the company’s safety culture.
In addition to the missed opportunity to identify unsafe flying practices, the investigation found examples of SMS investigations that had incomplete analyses of underlying factors, inconsistent and/or incomplete corrective action plans, mismanaged corrective action timelines, and inadequate follow-ups. The company also excluded first officers (FOs) from some safety discussions, like the expectations communicated following the 2017 allegations of VFR flights in IMC. As a result, the FOs had not received a clear message from company management that operating under those conditions was prohibited, and what actions to follow if those conditions were encountered during a flight. In the absence of clear direction from management, the occurrence FO was not unduly concerned about operating visually in conditions that were below VFR weather limits.
Finding as to causes and contributing factors
North Star Air’s SMS did not identify the underlying factors that led to the reported instances of company aircraft operating VFR flights into IMC, nor were any additional measures taken to monitor its DC3-TP67 operation to ensure flights were being conducted in accordance with regulations. As a result, previously identified unsafe practices persisted, and played a direct role in this occurrence.
2.5 Crew resource management
Modern CRM training is predicated on threat and error management. Critical components of threat and error management include topics such as decision making, situational awareness, and crew communication. Flight crews should be taught practical strategies that help ensure effective crew communications, thereby helping align team mental models, to optimize flight crew decision making. This will help them avoid traps or mitigate threats and errors that may arise.
As seen in this occurrence, from the time the captain decided to conduct the large 360° turn until shortly before landing, the FO was unaware of the aircraft’s position or the captain’s plan. At no time did the FO attempt, nor feel the need, to assert himself even though he was unaware of the plan and the aircraft was being visually manoeuvred at very low altitudes in IMC. Instead of seeking additional information (rebuilding situational awareness) from the more experienced captain, or proposing a different course of action, the FO began calling altitudes and airspeeds.
When the captain initiated the 360° turn, he did not brief his intended course of action nor actively seek out the FO’s opinion to ensure that they had a shared mental model of the situation. Instead, the captain, who had extensive experience on the aircraft and in that role, adopted a single-pilot mindset for the rest of the flight. This is likely due, in part, to attentional narrowing from the increased workload that would have occurred as the aircraft was manoeuvred at low altitude in very poor weather. As a result, the lack of communication between the captain and the FO resulted in degraded situational awareness, leading to sub-optimal decisions that significantly increased the risk of a CFIT accident.
From the point that the aircraft commenced the large 360° turn, the flight crew stopped acting as a cohesive team. Each crew member had a different mental model and both lacked the necessary CRM skills and/or strategies to re-align their mental models and choose a safer course of action. The initial CRM training provided by North Star Air met the requirements of subsection 724.115(38) of Commercial Air Service Standard 724; however, the training was based on earlier generation CRM standards that were primarily aimed at changing attitudes toward CRM. It did not include many practical modern CRM strategies such as highlighting barriers to effective communication, specifically trans-cockpit authority gradient, and multiple communication strategies that can be drawn upon depending on the severity of the situation, the time available, and the other person(s) involved in the communication process. As a result, North Star Air’s program was ineffective at providing FOs with adequate training in practical CRM strategies to use when they need to speak up because they are concerned about the safety of the flight, or if they are unsure of the plan. Likewise, North Star Air’s CRM program did not provide captains with adequate practical strategies to create an atmosphere where an FO’s feedback is welcomed and encouraged, which would increase the likelihood that a less-experienced individual feels confident to speak up.
Finding as to risk
If pilots of multi-crew aircraft are not provided with, and given an opportunity to practise, modern CRM strategies, there is increased risk that safety margins will be compromised because of breakdowns in crew coordination.
2.6 Transport Canada oversight
When SMS was introduced, it was intended to provide an additional layer of safety beyond traditional regulatory oversight. Before 2015, TC required all SMS enterprises to undergo an assessment to verify that the systems in place were effective to ensure ongoing regulatory compliance and to manage safety. However, in recent years, there has been a shift in TC’s approach to surveillance planning away from systems-level surveillance activities, such as assessments and program validation inspections (PVIs), in favour of the more narrowly focused process inspections (PIs).
In 2015, TC stopped conducting the assessments previously required for newly certificated operators within 12 months of the initial certification. As a result, TC began to approve a company’s SMS without having any assurances that the elements, which are described in a company’s SMS manual, are actually in place and effective. TC approved North Star Air’s SMS manual in 2017 when the company had a CARs Subpart 703 and CARs Subpart 704 air operator certificate. At that time, 6 of the 17 SMS elements were not fully implemented. When CARs Subpart 705 operations, which require an SMS, were approved in 2018, TC did not revisit North Star Air’s SMS manual approval from 2017.
This is not the first time that issues related to TC’s ability to provide adequate oversight have been identified in TSB investigations. One of those investigations resulted in multiple recommendations related to TC’s approach to oversight, including Recommendation A16-13, which specifically calls for TC to conduct regular assessments. However, in recent years TC appears to be moving in the opposite direction: first by removing the requirement to conduct an assessment as part of the SMS approval process, and more recently, with the decision to rely on PIs as the primary surveillance activity.
At the time of report writing, SMS assessments are now used only as a reactive surveillance activity when invoked by the Oversight Advisory Board.Footnote 114 The move from regular assessments and PVIs in favour of the more narrowly focused PIs represents a change in the nature of regulatory oversight activities that, as seen in this occurrence, makes it difficult for TC to have assurances that an SMS enterprise has the ability to effectively manage safety. Safety management and regulatory surveillance are on the TSB’s Watchlist. Until Recommendation A16-13 is addressed, the safety deficiencies related to SMS and regulatory surveillance identified in this occurrence will continue, increasing the risk of unsafe conditions going undetected and persisting.
Finding as to risk
If TC approves a company’s SMS without first conducting an in-depth review to ensure that all required elements are present and effective, SMS enterprises may not have the ability to effectively manage safety.
In addition to the reduction of systems-level surveillance activities, this investigation also highlighted previously identified issues with TC’s verification of company corrective action to ensure a timely return to a state of compliance. In response to the December 2017 allegations of North Star Air DC3-TP67s operating on multiple occasions under VFR in IMC, which also happened in this occurrence, TC provided the information about the allegations to the company for its internal investigation. Also, TC initiated a reactive PI in February 2018 that included 3 flight inspections. Those flight inspections were deemed to be uneventful; however, it is unrealistic to think that pilots would knowingly engage in rule-breaking behaviour when they are aware that the flight is being monitored by the regulator.
TC did not include in its November 2018 PI the allegations of pilots conducting VFR flights in IMC. As a result, TC did not identify that the company’s investigation had not determined a root cause, that it resulted in corrective action directed only at the captains, and that, at the time of the occurrence, the investigation was still open after almost 2 years. As seen in this occurrence, the unsafe practice of operating under VFR in IMC persisted unbeknownst to the regulator.
Finding as to risk
If TC relies on operators to investigate allegations of regulatory non-compliance without monitoring them, there is an increased risk that the unsafe practices that are being investigated will persist.
2.7 Visual flight rules flight planning
Flight plans and flight itineraries are designed so that search and rescue (SAR) alerting services will be initiated in the event of an overdue aircraft. Flight plans also provide critical information that will help SAR personnel respond in a timely and appropriate manner. In this occurrence, the pilots departed without having filed a flight plan or flight itinerary, contrary to regulatory requirements. As a result, the occurrence flight did not have the protection provided by a flight plan or a flight itinerary. Fortunately, owing to the nature of the crash and its proximity to the airport, the flight crew was able to easily reach safety and obtain assistance from the nearby police service personnel.
Finding as to risk
If pilots do not file flight plans or flight itineraries, as required by regulations, there is a risk that following an accident SAR services will be delayed, reducing the aircraft occupants’ chances of survival.
2.8 Cockpit restraint systems
In this occurrence, and as seen in the other North Star Air’s DC3-TP67 occurrence that took place on 21 June 2019, the pilots did not wear the available inertia-reel shoulder harness. Shoulder harnesses help ensure a more equal distribution of impact forces. Wearing a lap strap and a shoulder harness is known to reduce the severity of injuries to the upper body in the event of an accident, compared to wearing only the lap strap. The shoulder harness allows for some freedom of movement to reduce the likelihood that pilots will either unfasten it during flight or not wear it at all.
However, on the occurrence aircraft type, the layout of the cockpit panel switches and the location of the landing gear controls can make it difficult for pilots to reach them while wearing a shoulder harness. Nevertheless, if pilots do not use available shoulder harness, there is an increased risk of injury in the event of an accident. The risks associated with not wearing a shoulder harness have been extensively documented, and were also communicated to North Star Air.
Finding as to risk
If cockpit restraint systems do not fully accommodate pilot functional reach or if they are not used correctly, there is an increased risk of injury during an accident.
2.9 Absence of cockpit voice recording
Although not required by regulation, the occurrence aircraft was normally equipped with a CVR. However, following repairs, a paperwork error resulted in the CVR being placed in inventory instead of being re-installed in the occurrence aircraft. At the time of occurrence, it had been 329 days since the CVR had been removed, i.e., over 200 days beyond the maximum permissible time defined in the minimum equipment list. Since the CVR had not been re-installed in the occurrence aircraft, valuable information was not available to assist the investigation.
Finding as to risk
If cockpit voice and flight data recordings are not available, it is more difficult to accurately assess CRM, standard operating procedure execution and effectiveness, and workload management. As a result, the absence of on-board flight recordings can limit the identification of safety deficiencies and the advancement of safety.
2.10 Emergency locator transmitter
In this occurrence, the aircraft’s ELT activated; however, because the whip antenna was ripped off during the crash sequence, a signal was not detected by SAR satellites. Although it did not play a role in the outcome of this occurrence, it highlights previously identified risks associated with ELT design standards. As a result, the TSB issued Recommendation A16-05 calling for TC to establish rigorous ELT system crash survivability requirements. The Board assessed the recommendation as fully satisfactory when TC implemented updated regulations for new ELT design approvals. Although recent regulatory amendments include more stringent requirements for new ELT design approvals, these do not apply to legacy ELTs.
Finding as to risk
If aircraft operate with ELTs approved under legacy design standards, there remains a risk that potentially life-saving distress signals will not be detected because of damage caused to the ELT system during an accident.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- The decision to depart on, and continue, a visual flight rules flight in instrument meteorological conditions was influenced by a distorted perception of risk resulting from successful past experience in similar situations.
- The captain likely experienced attentional narrowing while carrying out a high-workload visual approach at very low altitude in instrument meteorological conditions. This most likely resulted in an inadvertent but controlled descent that was not detected until the aircraft collided with terrain.
- The result-oriented subculture of some North Star Air’s DC3-TP67 pilots, which emphasized mission completion over regulatory compliance, resulted in visual flight rules flights, such as the occurrence flight, being conducted in instrument meteorological conditions.
- North Star Air’s safety management system did not identify the underlying factors that led to the reported instances of company aircraft operating visual flight rules flights into instrument meteorological conditions, nor were any additional measures taken to monitor its DC3-TP67 operation to ensure flights were being conducted in accordance with regulations. As a result, previously identified unsafe practices persisted, and played a direct role in this occurrence.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If minimal supervision of flight crews occurs within a company’s flight operation, there is a risk that previously identified unsafe or non-compliant practices will persist.
- If pilots of multi-crew aircraft are not provided with, and given an opportunity to practise, modern crew resource management strategies, there is increased risk that safety margins will be compromised because of breakdowns in crew coordination.
- If Transport Canada approves a company’s safety management system without first conducting an in-depth review to ensure that all required elements are present and effective, safety management system enterprises may not have the ability to effectively manage safety.
- If Transport Canada relies on operators to investigate allegations of regulatory non-compliance without monitoring them, there is an increased risk that the unsafe practices that are being investigated will persist.
- If pilots do not file flight plans or flight itineraries, as required by regulations, there is a risk that following an accident search and rescue services will be delayed, reducing the occupants’ chances of survival.
- If cockpit restraint systems do not fully accommodate pilot functional reach or if they are not used correctly, there is an increased risk of injury during an accident.
- If cockpit voice and flight data recordings are not available, it is more difficult to accurately assess crew resource management, standard operating procedure execution and effectiveness, and workload management. As a result, the absence of on-board flight recordings can limit the identification of safety deficiencies and the advancement of safety.
- If aircraft operate with emergency locator transmitters approved under legacy design standards, there remains a risk that potentially life-saving distress signals will not be detected because of damage caused to the emergency locator transmitter system during an accident.
4.0 Safety action
4.1 Safety action taken
4.1.1 North Star Air Ltd.
Following the occurrence, North Star Air Ltd. implemented a flight operations quality assurance program.
4.1.2 Transport Canada
In December 2020, Transport Canada conducted a process inspection (PI), focusing on the evaluation and effectiveness of the long-term corrective action plan related to the flight operations findings from the December 2019 PI. Transport Canada concluded that the long-term corrective actions taken by North Star Air Ltd. were effective.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .