Derailment
Canadian National
train no. 698, Ontario Northland Railway
Mile 225.8, Newmarket Subdivision
North Bay, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 31 March 1996, at approximately 1414 eastern standard time, Ontario Northland Railway train No. 698, travelling southward, derailed at Mile 225.8 of the Canadian National (CN) Newmarket Subdivision. Three of the four coaches, the locomotive and the electrical power unit derailed. Eight passengers and two railway employees sustained minor injuries.
The Board determined that the trailing truck of the locomotive took the diverging route at the switch at Mile 225.8, damaging the track structure and resulting in the derailment. The switch had been damaged and its operation compromised as a result of the switch stand having been struck by a highway vehicle that had been driven onto posted CN property. CN officials had not been notified of the damage.
Ce rapport est également disponible en français.
1.0 Factual Information
1.1 The Accident
Southward Ontario Northland Railway (ONR) passenger train No. 698 (train 698) was en route from Cochrane, Ontario, to Toronto, Ontario, with 54 passengers. At approximately 1414 eastern standard time, while moving west to east approaching Mile 225.8 of the CN Newmarket Subdivision, just south of North Bay, Ontario, at a speed of approximately 44 mph, the locomotive engineer observed that the siding switch stand at Mile 225.8 was canted off-centre. Concerned that the switch might be damaged, he immediately initiated an emergency brake application. The locomotive engineer estimated that the train contacted the switch area at a speed of 20 mph. When the train came to a stop, the locomotive engineer looked back and observed that a portion of the train had derailed. All cars were upright (Figure 1).

The second locomotive engineer made an immediate emergency radio broadcast to alert other trains in the area of their situation. He then radioed the rail traffic controller (RTC) and received track protection for their train. Worried that there may be serious passenger injuries, he also requested emergency medical assistance. The first locomotive engineer, concerned that the electrical power to the coaches might cause a fire, shut down the power source. The first locomotive engineer remained in the lead locomotive, accessible to the locomotive radio, and the second locomotive engineer went back to the derailed coaches to assist the passengers.
The RTC contacted ONR officials in North Bay who immediately contacted ambulance services and the local police. Arrangements were also made to dispatch buses to the derailment scene.
Passengers reported that, as the train decelerated, the coaches bounced about and they observed dust and gravel flying by the windows. The bouncing motion threw some passengers from their seats. In the first coach behind the locomotive (the second car), the side wall separated from the floor. Once the train had stopped, passengers believed that steam coming from the first car (an auxiliary power unit (APU) ) and entering the coach through the opening in the side wall was smoke from a fire. The APU was tight against the first coach, blocking exit through the forward end door. The leading end side vestibule door (north facing) was jammed. The emergency windows would not open and the passengers exited the coach through the rear vestibule side door (south facing), which had been opened from the outside by the operating crew.
The train had come to a stop with the trailing truck of the lead locomotive, the APU and the first three coaches derailed to the south side of the track. The trailing truck of the APU had pulled away and the three derailed coaches were leaning at various angles. The passengers and crew in the second, third and fourth coaches were unable to detrain to the north side due to the wreckage debris; however, they were able to detrain through the south-facing vestibule side doors without difficulty.
Communication between passengers and the crew members was difficult as there were no portable loudhailers available. The public address system only functioned within the coaches and relied on auxiliary power.
Emergency personnel arrived by an adjacent CN service road and immediately administered comfort and first aid to the injured. Three injured passengers were taken by ambulance to hospital in North Bay. Buses transported the remaining passengers and crew to North Bay.
1.2 Injuries
Eight passengers and two crew members sustained minor injuries.
1.3 Track Damage
Approximately 350 feet of track was destroyed. The manually operated switch at Mile 225.8 was also damaged beyond repair.
1.4 Personnel Information
The operating crew consisted of two locomotive engineers, a conductor and an assistant conductor. The two locomotive engineers and the assistant conductor were positioned in the lead locomotive. The conductor was positioned in the last passenger coach. Two on-board service (OBS) personnel were in the second and third cars.
The operating crew members were qualified for their respective positions and met fitness and rest standards established to ensure the safe operation of trains.
1.5 Train Information
The train was marshalled from front to rear as follows:
| EQUIPMENT TYPE | ONR NUMBER | POSITION |
|---|---|---|
| Locomotive | 1808 | Leading |
| Auxiliary Power Unit | 204 | Second |
| Day Coach | 611 | First Coach |
| Kitchen car | 702 | Second Coach |
| Day Coach | 615 | Third Coach |
| Day Coach | 614 | Fourth Coach |
This train is operated daily from Cochrane, via North Bay, to Toronto. ONR crews operate the train from Cochrane to North Bay as it travels on the ONR Temagami Subdivision. At North Bay, the train is routed to CN's Newmarket Subdivision where it is operated to Toronto by a CN operating crew. The OBS personnel are all ONR staff and remain on the train for the entire trip.
1.6 Particulars of the Track
The CN Newmarket Subdivision is a north/south subdivision, stretching from Capreol, Ontario (Mile 311.1), to Parkdale, Ontario (Mile 2.4). Access to the CN Newmarket Subdivision from the ONR Subdivision occurs at Mile 226.8 in North Bay. At the occurrence location, the subdivision comprises a single main track with a two-degree left-hand curve, in the direction of the train's travel, and a 0.5 per cent descending grade.
The track consists of 115-pound continuous welded rail with softwood ties that were installed on crushed rock ballast. The track condition in the derailment area was good.
On 29 March 1996, two days earlier, the operating crew of ONR train No. 697 (train 697) passed over the area in the opposite direction and no problems were noted. Train 697 was the last train to pass over the switch before the arrival of train 698. There were no ONR or CN employees working in the area over the weekend.
1.7 Method of Train Control
The Newmarket Subdivision is governed by the Occupancy Control System (OCS) authorized by the Canadian Rail Operating Rules. Train movements are supervised by an RTC located in Toronto.
In the area of the accident, the authorized maximum train speed was 45 mph for passenger trains and 35 mph for freight trains.
1.8 Weather
At the time of the occurrence, the sky was overcast, winds were calm, and the temperature was five degrees Celsius.
1.9 Recorded Information
The event recorder on the locomotive used an eight-track tape recording system, and contained limited information. However, it did indicate that, at the moment the operator initiated the emergency brake application (no actual time recorded), the train was proceeding at a speed of 44 mph, with the throttle in the No. 8 (full throttle) position and the service brake released.
1.10 Occurrence Site Information
1.10.1 General
At the derailment site, a gravel CN service road runs parallel to the track, providing access to a track material storage yard. There is a single sign advising those approaching the roadway from a public thoroughfare, "Danger, Do Not Trespass"; however, access is not restricted. Local police have indicated that the road is used by some to drink in their vehicles, although the area is not known as a trouble spot and is infrequently patrolled.
Within the borders of the storage yard, there is a wye track used to reverse rolling stock. This wye track is also used to exchange ONR and CN equipment. The switch stand at Mile 225.8 is used to operate the manual switch that provides access to the north wye track.
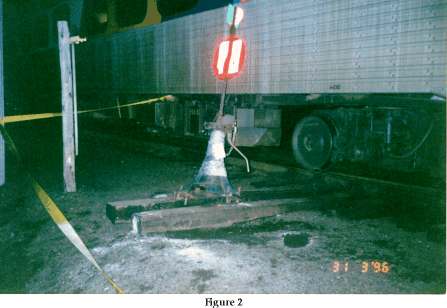
The switch was canted over at approximately 20 degrees from vertical. There were tire tracks from the gravel road stopping at the switch stand. There were scuff marks on the switch stand approximately 14 inches (36 cm) from the base of the stand and particles of white paint were imbedded in the scuff marks. The switch stand securing spikes were loose and the anchoring ties were dislodged (Figure 2). The switch was lined for the normal position and the switch target was in place and properly indicated that the switch was lined for the main track. An examination of the switch revealed that the components were in good condition, properly adjusted and well maintained. The force required to dislodge the switch stand was considerable. The person(s) responsible should have been aware of the impact, as damage to the vehicle would have been significant.
1.10.2 Equipment
The trailing truck of the locomotive was derailed and the locomotive was leaning at a slight angle. The leading end of the APU was still coupled to the locomotive. The trailing end extended over the open area between the main track and the north wye track. The trailing truck was missing.
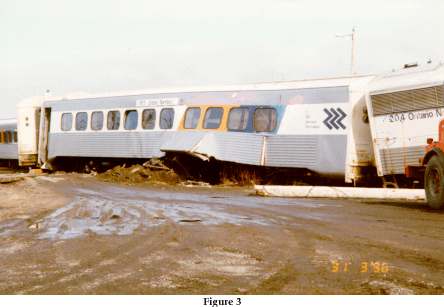
The first coach was completely derailed and in line with the north wye track. A gap, approximately 18 inches (46 cm) by 48 inches (122 cm), had opened between the south wall and floor. A hole had been punched in the leading end roof line and, due to minor frame deformation, the side vestibule door would only partially open. Most underslung components, including the hot water tank, had been torn away. The hot water tank was leaking and steam had escaped and entered the interior of the coach via the opening between the wall and the floor (Figure 3).
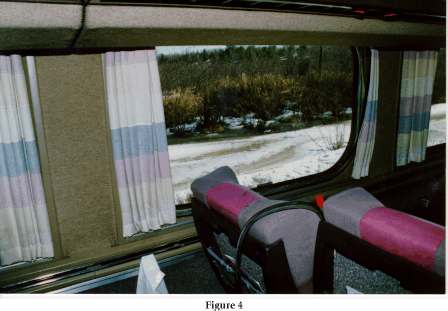
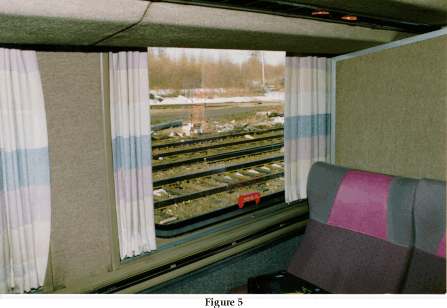
Five of the emergency exit windows in the first coach had their rubber gaskets partially or completely removed; however, the window panels were still in place. One of the five windows had been struck from the inside and cracked, and two had been loosened from their securement. One of the windows, with the gasket completely removed, was of the non-emergency window type with no lift-out handle. This window was still tightly in place. Some reclining seat backs were found to have partially obstructed direct access to the window handles (Figure 4). The rearmost emergency window (south side) was partially obstructed by a baggage containment area (Figure 5).
The leading end of the second coach (kitchen car) remained coupled to the first coach and extended from the north wye track back to the main track and was resting upright. The end door providing access to the first coach was not in line, making it treacherous to pass from one coach to the other through the end doors. The underframe was extensively damaged with underslung components and brake rigging damaged or torn off. The lead truck of the third coach was derailed near the main track. The fourth coach was not derailed. Debris from the derailed cars, as well as ballast and track material, had collected between the coaches and the main track.
1.11 ONR Passenger Equipment
1.11.1 General
The coaches are refurbished uni-level, lightweight commuter cars originally built for service in Toronto (GO Transit). As originally equipped, they did not have baggage storage areas, a galley for food preparation, or large washrooms supplied with hot water. The original seats, practical for commuter service, were small and easily cleaned. In order to make the cars suitable for long-distance passenger service, the ONR refurbished them to Ontario Northland Transportation Commission General specification No. 433 at their shops in North Bay and, at the time of the occurrence, 14 of the 20 coaches purchased had been refurbished. To meet this specification, large comfortable upholstered seats that rotate in pairs were installed. Each coach was equipped with relatively large washrooms with hot water. New heating, air conditioning and electrical systems were added and baggage storage areas were installed. The coaches were also equipped with manually operated doors and steps. The modifications made to each coach increased its weight by approximately 13,000 pounds.
At the time the coaches were originally constructed for commuter service, each coach had been built to meet the Association of American Railroads (AAR) Standard S-034-69 for structural strength. This standard outlines criteria for longitudinal impact resistance only. As originally designed, these commuter coaches complied with this standard. Once refurbished and extensively refitted, the modified coaches did not trigger AAR or regulatory interest.
1.11.2 General Lighting and Emergency Lights
General lighting, heating, air conditioning and the public address system are powered by the APU. The emergency backup system is powered by batteries in a case suspended from the underframe of each coach. This emergency system is activated automatically whenever power from the APU is cut off.
The battery system operates the emergency lighting only. These lights are located under aisle seats on one side of the coach, and overhead in the galleys, vestibules and washrooms. There are no emergency exterior lights to illuminate the exterior of the coaches for passengers detraining in the dark, nor are the coaches equipped with portable lights such as flashlights.
1.11.3 Doors, Steps and Windows
The ends of each coach contain a vestibule area. Each vestibule is equipped with a manually operated hinged side door and a hinged end door. The side doors in the respective vestibules are installed on opposite sides of the cars. All doors swing inward.
The vestibule side doors are secured with three latches, with large handles to rotate and lift the latches. No written instructions were posted to advise passengers how the door securement system operates.
From the interior of the coach, the mechanism on the top and bottom latches is visible and the operation of these latches is obvious. The mechanism for the middle latch is hidden but its operation would, no doubt, be thought to be consistent with the others. On the exterior, the operation of the latches is not apparent and there are no pictograms or written instructions to indicate the method of operation.
A panel covers the vestibule steps. The stairs are exposed by stepping on a release latch and manually lifting the panel, which then automatically exposes and lowers the steps. There were no written instructions posted on the interior or exterior to advise passengers or rescue personnel of the operation of the release latch and its location, neither of which is obvious (Figure 6). During an emergency evacuation, deployment of the stairs would help passengers exit the train and would lessen the risk of injury.

The end doors are secured in place with three latches in a similar fashion to the side doors. As with the side doors, there are no written instructions to provide passengers with information on how to operate the latches; however, as with the side doors, the latch operation is obvious from the interior and not as obvious from the exterior. The upper halves of both the end doors and the side doors contain large safety glass windows measuring approximately 31 inches (78.74 cm) by 12 inches (30 cm).
The coaches are equipped with 12 emergency escape windows located every second window (the kitchen car is slightly different with only eight emergency windows). These windows consist of two 1/4 inch (6 mm) panes of safety glass. They measure 31 inches (78.74 cm) high by 50 inches (127 cm) wide and weigh approximately 59 pounds (26.8 kg). The sills are approximately 34 inches (86 cm) from the floor. A non-illuminated three-part pictogram on the window, above the handle, illustrates its operation (it was noted that two of the emergency windows in coach 611 did not have a pictogram). Each emergency window is identified by a large red handle with the words "Emergency Exit / Pull Handle - Remove Rubber." The gasket is to be removed by pulling on the handle. A second handle, fixed to the window and exposed by pulling the first handle away, is to be pulled and the window is designed to swing inward as though on hinges at the top (according to the pictogram), toward the interior of the coach (Figure 7).

1.11.4 Emergency Equipment/Procedure Information
A safety information plaque measuring 9 3/4 inches (25 cm) by 5 3/4 inches (14.5 cm) is affixed to the corridor wall of each vestibule. The written information advises that each car is furnished with emergency exit windows and emergency equipment and exhorts passengers to become familiar with where these are located. A pictogram of the floor plan of the coach indicates the emergency exit locations as the emergency exit windows and the end doors. Attached to the exterior coach walls below the emergency windows are red decals written: "Emergency Window." From the outside, however, there is no method--other than breaking the glass--to gain entry through the emergency windows.
Individual passenger seating areas are not supplied with safety instructions and procedures. It is not the practice to make announcements to the passengers regarding the location of emergency equipment or emergency evacuation procedures. Emergency equipment in each car includes a basic first-aid kit, fire extinguishers, axe, sledgehammer, and a hand saw. These articles are stored in prominently marked and accessible bins in various locations in the coaches.
The first-aid and fire-fighting equipment meet the requirements of the On Board Trains Occupational Safety and Health Regulations ancillary to Part II of the Canada Labour Code.
1.12 Tests and Research
1.12.1 Emergency Window Exits
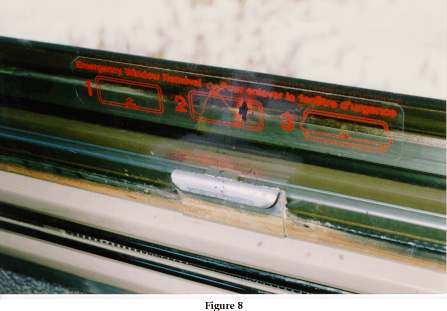
Since the passengers failed in five out of five attempts to open the emergency windows, tests were conducted to evaluate the operation of these windows as depicted on the pictogram, and to understand the difficulties that may have been encountered. The pictogram indicated that the bottom of the window must be eventually pulled inboard. At the first window, the seat back (the seat was in the reverse position) was partially obstructing access and inward window movement. The first step was therefore to swing the seat around to face forward. This involved the activation of a lever under the aisle seat before the seats would swivel. The location of the lever was not obvious and was difficult to locate under test conditions. The second step was to pull the bright red handle and remove the rubber gasket. As attempts to remove the gasket by two male TSB investigators of average height and weight were unsuccessful, the evaluation was continued at another window.
The gasket was removed on the second window by using a jerking motion. Once the gasket was removed, a small metal handle used to pull the window inward was exposed (Figure 8). However, the window remained stuck tightly in the frame. Loosening the window required considerable pulling and jerking on the small metal handle. Once the window was loose within the window frame, it became jammed and could not be removed. It was determined that the window must first be lifted upward using a jerking motion and then pulled inward. At this point, the window fell away from the frame. Considerable effort was then required to manoeuvre the heavy window to clear the path for exit.
1.12.2 TSB Engineering Branch Report
The TSB Engineering Branch conducted an examination of the emergency window operation, coach structural integrity, side and end door operation, and emergency escape signage. The report (LP 037/96) indicates that:
- the construction of the passenger coaches results in an exposed side sill, which in this case, was pushed outwards by debris at derailment;
- the location of the gap in the side wall of the coach, generated by rather gentle forces, minimized the possibility of an occupant falling out although the torn metal would have cut those who contacted the area;
- coach structural design standards principally address normal service loads and do not provide for the types of loads experienced in this derailment where debris piled up underneath the car and pushed the side sill outwards;
- VIA Rail Canada Inc. (VIA) passenger cars have rounded and completely enclosed bottoms without exposed side sills or small lips on the side sills;
- the emergency windows are not subject to scheduled removal and, if in place for a very long time, the seals become stiffer;
- structural deformation of the coach would make the emergency window removal more difficult;
- the jamming of the leading end side vestibule door as a consequence of minor damage is considered inappropriate;
- the force required to remove the emergency window gasket varied considerably and in some cases was beyond the capabilities of passengers of average strength;
- the little metal handle on the emergency exit windows limits the force that can be applied to it and causes the windows to jam on the window frame;
- the weight of the window makes it difficult to manoeuvre; and
- the lack of instructional signs on the exterior of the coach doors could hinder rescue efforts.
1.13 Other Information
1.13.1 The Evacuation
Although train-wide emergency evacuation instructions could not be broadcast, evacuation efforts by the OBS personnel and the train operating crew were met with relative calm. However, there were a few distraught and anxious passengers, and there were difficulties in informing passengers of a gathering point and providing them with information pertaining to their return to North Bay.
1.13.2 Passenger Car Safety Standards
At the time of this occurrence, there were no standards providing minimum safety criteria for the design, retrofit or refurbishing of railway passenger rolling stock. Furthermore, there were no standards providing for emergency exit design or the size, content, and visibility (including visibility in darkness or smoke) of emergency signage. No requirement existed to provide emergency information to passengers on boarding, including oral, written or pictorial information. Emergency voice broadcast capability on emergency power both inside and outside the cars as well as emergency exterior lighting and adequate portable lighting (flashlights) were not requisites.
On 20 November 1994, a VIA train with Light, Rapid, Comfortable (LRC) equipment struck a piece of rail placed on the tracks near Brighton, Ontario. The piece of rail damaged the locomotive fuel tanks and severed electrical cables. The fuel leaking ignited and the ensuing fire placed many passengers in a life-threatening situation. Forty-six passengers were injured (TSB occurrence report R94T0357). The TSB investigation into the accident exposed deficiencies in LRC passenger car safety design and evacuation standards. As a consequence, VIA, in concert with Transport Canada, rectified or initiated steps to rectify the identified safety deficiencies. In addition, the Board recommended that:
The Department of Transport, in consultation with the railway industry, establish standards governing all emergency aspects of railway passenger safety; and
Transportation Safety Recommendation R96-10
The Department of Transport review its procedures regarding regulatory oversight of railways to ensure that the required level of railway passenger safety is maintained.
Transportation Safety Recommendation R96-11
On 22 April 1995, VIA train No. 1, travelling westward at 17 mph, derailed at Mile 11.12 of the CN Clearwater Subdivision, near Blue River, British Columbia. All 13 coaches and the 2 locomotives derailed (TSB occurrence report R95V0089). Nine of the 172 passengers and 3 of the 15 OBS personnel sustained minor injuries. The design and fit-out of the various passenger cars in the train did not present undue obstacles to the safe and timely evacuation of the train; however, many of the same shortcomings in passenger coach safety design as those identified in the TSB report of the accident at Brighton were evident in this occurrence.
On 16 February 1996, eastbound Maryland Rail Commuter (MARC) train No. 286 collided with westbound National Railroad Passenger Corporation (Amtrak) train No. 29 on CSX main track near Silver Springs, Maryland. There were 3 operating crew members and 20 passengers on board the MARC train. There were 4 operating crew members, 13 OBS personnel and 164 passengers on board the Amtrak train. The fuel tank of the Amtrak lead locomotive ruptured on impact and the diesel fuel ignited. Fire engulfed the locomotive and burning fuel spilled onto the first MARC car (a cab car). Two crew members and seven passengers on the MARC train died of smoke inhalation.
Several surviving passengers on the MARC train stated that they were unaware of the locations of the emergency exits, and none knew how to operate them. Two of the passengers made several unsuccessful attempts to open the left and right exterior side doors. They stated that no instructions were provided concerning the operation of the door handle in an emergency. They eventually escaped through an opening in the damaged body of the second car.
The National Transportation Safety Board (NTSB) of the United States examined the first and second MARC cars and found that the left and right rear exterior side doors were jammed. None of the doors had removable windows or pop-out emergency escape panels for use in an emergency. Emergency quick-release mechanisms for the exterior doors were located in secured cabinets some distance from the doors they controlled.
The NTSB also found that one car had no interior emergency window decals, and noted that the exterior emergency decals were often faded or obliterated. Moreover, the information on the exterior decals directed emergency responders to another sign at the end of the car for instructions on how to open emergency exits.
No comprehensive passenger car safety standards were in place in the United States. Consequently, the NTSB concluded that U.S. Federal Railroad Administration (FRA) safety inspection personnel should determine whether unsafe conditions exist on other lines. The NTSB further concluded that the FRA should issue emergency orders to correct such unsafe conditions as necessary, and incorporate the emergency measures into minimum passenger car safety standards. On 12 March 1996, the NTSB recommended that the FRA:
Inspect all commuter rail equipment to determine whether it has:
- easily accessible interior emergency quick-release mechanisms adjacent to exterior passageway doors;
- removable windows or kick panels in interior and exterior passageway doors; and
- prominently displayed retro-reflective signage marking all interior and exterior emergency exits.
If any commuter equipment lacks one or more of these features, take appropriate emergency measures to ensure corrective action until these measures are incorporated into minimum passenger car safety standards.
Also, on 12 March 1996, the NTSB recommended that the Mass Transit Administration of the Maryland Department of Transportation:
Install removable windows or kick panels for emergency exits in interior and exterior passageway doors.
Install an easily accessible interior emergency quick-release mechanism adjacent to all exterior doors.
Install retro-reflective signage on car interiors and exteriors at emergency exits that contains easily understood instructions and clearly marks all emergency exits (doors and windows).
1.13.3 North Bay Police and CN Police Investigation
The North Bay police, working with the CN Police, removed the damaged switch stand to analyse the paint chips and took plaster imprint casts of the tire tracks leading to the damaged switch stand. Their investigation has determined that the damage to the switch was caused by a highway vehicle. The person(s) responsible did not report that they had damaged the switch.
2.0 Analysis
2.1 Introduction
The operation of train 698 was in accordance with company operating instructions and government safety standards just before the derailment, and played no role in the accident. When the switch stand was struck by the highway vehicle and dislocated from its securement, the mechanism could no longer hold the switch points tight to the rail. The train derailed when the passage of the locomotive opened the switch points, allowing the trailing truck to follow the diverging route, damaging the track and derailing the APU and the three coaches. The switch had been well maintained and showed no sign of pre-accident mechanical malfunction or maladjustment attributable to service neglect.
The locomotive engineer was attentive to the route ahead and, having noticed the damaged switch stand in time to brake, was able to reduce train speed significantly, reducing the severity of the derailment.
It cannot be categorically stated that the person(s) striking the switch stand would have been aware that the damage had occurred, nor is it certain that, having observed the damage, such person(s) would have been aware that the operation of the switch was compromised and thus, safe train operation jeopardized. However, considering the size and ruggedness of the switch stand, it is most likely that the highway vehicle sustained significant damage. The proper course of action to follow would have been to alert railway officials to the situation, so as to ensure the safety and well-being of others.
2.2 Consideration of the Facts
2.2.1 Emergency Exit
2.2.1.1 Emergency Windows
Passengers, who believed their lives were in jeopardy, were unable to free the emergency windows from their mountings, and so exit the train. Subsequent attempts by TSB investigators, under test conditions, met with similar results. It must be concluded, therefore, that the emergency exit windows, as designed and maintained, do not fulfil their role.
Although one major shortcoming--the difficulty in removing the rubber gasket--can be overcome by lubrication and/or routine maintenance, other aspects of the design of the emergency exit windows proved to interfere with their deployment, including:
- a propensity for the frame to jam even with the gasket removed;
- the difficulty in using the small handle to manoeuvre the window;
- the difficulty in moving the window aside once freed, considering its size and weight; and
- the interference to window access and removal as a result of baggage rack placement and seat design (seats rotated to the reverse position block window area).
In addition, even if the windows are successfully removed, there is a relatively high sill to clear, followed by a dangerously high jump to the roadbed. Only mobile, fit occupants would find such an exit route feasible. Since there is no mechanism to remove the emergency windows from the outside, the decals applied to the exterior walls of the coaches, presumably to assist first responders to an emergency, serve no apparent purpose.
It is cause for concern that one of the emergency windows that passengers attempted to open was not in fact fully outfitted for such use, in that there was no metal handle fitted to the window. During the installation of the window, such a defect should have been obvious; it was subsequently masked by the outer handle. Since there was no periodic maintenance of the window gaskets, this deficiency remained undetected until the attempted use in an emergency situation. Similarly, although there were sufficient numbers of emergency windows, two did not have pictograms illustrating their operation. While the instructions on the red handle would likely prompt passengers to pull the gasket away in an emergency situation, they then might be uncertain as to the next step, especially since the windows are difficult to remove. This oversight seems to indicate a lack of quality assurance regarding passenger safety features.
2.2.1.2 Vestibule Side Doors
The operation of the vestibule side doors and end doors is straightforward; they offer a relatively efficient means of escape. Emergency instructions assisting passengers in quickly identifying the operation of the doors (including the stairs) would improve safety as would instructions on the exterior providing the same information to first responders.
The jamming of the leading end vestibule side door, attributed to minor deformation of the car frame, points to a need to carefully engineer door-opening areas to resist impact to the extent practicable. Such a design consideration would be a suitable inclusion in a passenger car safety standard.
2.2.1.3 Emergency Information Sources
Other than the labelling on the emergency exit windows, the only emergency exit information provided was on the vestibule plaques. It is improbable that passengers, while boarding, would stop to take note of this information. Since rapid evacuation can be crucial in an emergency, increased passenger awareness of all exit doors and emergency escape routes would increase safety.
2.2.1.4 Emergency Power
The locomotive engineer's decision to shut down the auxiliary power source was prudent; however, this action rendered the internal public address system inoperative. The crew members were thus denied an effective means to advise and reassure passengers who were still in the coaches. The system was not designed to broadcast outside the train.
The emergency power provides little illumination in the coach seating areas and the emergency windows and equipment do not have lit features. Emergency lighting in these areas would improve safety. There is no provision for exterior lighting under auxiliary or emergency power. Such a feature would facilitate passenger evacuation and control in the dark.
It is also noteworthy that the derailment ripped away the batteries supplying emergency power to the first coach. Shutting down auxiliary power in similar circumstances of darkness could increase the risk to the well-being of passengers. There may be merit in developing a system of standard procedures for such situations.
2.2.2 Coach Design Considerations
2.2.2.1 Damage Prevention
In the first coach, the forces of the derailment ripped away most of the underslung features, including the emergency power source. The design of the coach deck-to-side-wall configuration also permitted the forces of the derailment to tear a portion of the side wall away. Such an opening could expose passengers to the danger of being thrown out onto the roadbed while also enabling the entry of fire, smoke or noxious fumes, which are potentially present at a derailment. VIA equipment has protection against deck-to-side-wall damage; a passenger car design standard should address both side wall securement and under-car protection.
There has also been no apparent consideration of emergency exit in the event that the end doors become impossible to use (as they were in this occurrence) and with the coach coming to rest on its side.
2.2.2.2 General
Passenger coach design and fit-out has been largely left to the discretion of the builder. With the exception of meeting AAR structural standards (which do not address safety features), and various codes requiring first-aid supplies and fire-fighting equipment, there were no standards to meet or follow.
As has been demonstrated by the 20 November 1994 VIA accident at Brighton and the 16 February 1996 MARC/Amtrak accident, passenger coaches can quickly become life-threatening enclosures. Carefully considered standards for all aspects of passenger safety are necessary.
2.2.2.3 Access to Private CN Roadway
Access to the private CN road was not physically restricted, presenting an opportunity for clear, unmonitored vehicular access to the railway right-of-way. Although a 'no trespassing' sign was posted warning the public of danger, it was apparently widely disregarded and had little effect. The roadway, therefore, exposed both the public to the dangers of the railway as well as the railway to the possibility of vandalism and theft. To the extent practicable, such access routes should be secured.
3.0 Findings
- The train was being operated in compliance with government safety standards and ONR operating instructions just before the derailment.
- The trailing truck of the locomotive was diverted onto the wye at the switch at Mile 225.8, fracturing and displacing the rail and derailing the train.
- The switch had been struck and damaged by a highway vehicle that had been operated on CN property without permission.
- The damaged switch could not maintain the positioning of the switch points necessary for safe train passage.
- The switch stand and components were in good condition and well maintained and adjusted before being damaged by the highway vehicle.
- The individual(s) responsible for damaging the switch did not report the damage to railway officials, thereby creating a situation that presented an extreme hazard to train operation.
- The evacuation of the first coach was hampered as the emergency exit windows did not function as intended.
- ONR passenger safety was compromised due to a lack of: emergency evacuation information; emergency lighting of emergency signage or equipment locations; signage outlining door and step operation; public address capability on emergency power; and explanatory emergency window pictograms on all emergency windows. Safety was further compromised by the installation of a standard window at emergency window locations, and by a seat back and baggage racks partially blocking access to certain emergency exit windows.
- There were no Canadian passenger car safety standards establishing minimum safety requirements for new or refurbished equipment at the time of this occurrence.
3.1 Causes and contributing factors
The trailing truck of the locomotive took the diverging route at the switch at Mile 225.8, damaging the track structure and resulting in the derailment. The switch had been damaged and its operation compromised as a result of the switch stand having been struck by a highway vehicle that had been driven onto posted CN property. CN officials had not been notified of the damage.
4.0 Safety Action
4.1 Action Taken
On 07 July 1996, the Board issued four interim safety recommendations addressing safety deficiencies with respect to the functionality of the emergency exit windows, the absence of explicit instructions to open the windows, and interference with their operation by coach seats and baggage racks. The Board recommended that:
The Ministry of Northern Development and Mines of Ontario ensure that:
- an immediate, one-time, functional test on all emergency window exits on ONR passenger coaches is conducted; and
- a program for regular functional verification of emergency window exits on ONR passenger coaches is established;
The Ministry of Northern Development and Mines of Ontario ensure that explicit instructions for use of the emergency window exits on ONR passenger coaches are readily available;
Transportation Safety Recommendation R96-02
The Ministry of Northern Development and Mines of Ontario ensure that seats and luggage racks do not interfere with the use of the emergency window exits in the passenger coaches; and
Transportation Safety Recommendation R96-03
The Ontario Northland Transportation Commission undertake research with an aim to installing, in ONR passenger coaches, emergency exit windows that can be readily removed by able-bodied passengers.
Transportation Safety Recommendation R96-04
In response, the Ontario Northland Railway (ONR) indicated that several measures were being implemented to facilitate passenger egress in an emergency situation:
- A functional test has been performed on all emergency windows on all Ontario Northland Northlander coach equipment. This work was done by a number of different employees at two locations on Ontario Northland. Each window was removed, cleaned and re-applied.
- A regular functional verification of emergency window exits will be scheduled annually as part of the regular coach maintenance program.
- A placard, outlining schematically and in writing the emergency features of the car, will be placed on each seat.
- The training program for on-board service personnel and operating crews has been reviewed and a retraining program put in place. The program will include a physical review of the safety equipment on the car and every trainee will be required to physically remove one of the emergency windows. ONR will also undertake to provide the same training to regular CN crews on layover in North Bay.
- The turnable seats have been secured in a position to ensure unobstructed access to three emergency exit windows on each side of the coaches.
In addition to the interim safety recommendations issued during the investigation into this occurrence, the Board made other recommendations in July 1996 regarding the overall standard and overview of passenger safety in the railway industry.
Shortly after the fatal VIA accident at Biggar, Saskatchewan, the federal Minister of Transport announced a delay in the re-introduction of the proposed amendments to the Railway Safety Act to determine whether further adjustments to the legislation were required. The upcoming modifications to the Act will include provisions for passenger safety and the implementation of a regulatory regime to enforce these provisions.
Industry rules respecting passenger train emergency response and evacuation are being developed as Transport Canada (TC) is currently reviewing the first draft of the Passenger Handling Safety Rules, as submitted by the Railway Association of Canada (RAC).
TC has also approved the Railway Passenger Car Inspection and Safety Rules, with an effective date of 01 February 1998. The rules contain provisions on emergency exits, trauma kits (including megaphones), instructions, signage, securement of baggage, and emergency lighting, and prescribe "fail-safe" design of electrical and mechanical circuits and systems.
TC has verified that ONR has complied with the Board's recommendations and has outlined that they will continue to monitor the ONR for compliance to passenger train safety requirements. TC has also indicated that a switch point lock has been installed to prevent a similar occurrence at this location.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board, consisting of Chairperson Benoît Bouchard, and members Maurice Harquail, Charles Simpson and W.A. Tadros, authorized the release of this report on .
Appendices
Appendix A— Glossary
- AAR
- Association of American Railroads
- APU
- auxiliary power unit
- cm
- centimetre(s)
- CN
- Canadian National
- FRA
- Federal Railroad Administration
- kg
- kilogram(s)
- LRC
- Light, Rapid, Comfortable
- MARC
- Maryland Rail Commuter
- mm
- millimetre(s)
- mph
- mile(s) per hour
- NTSB
- National Transportation Safety Board
- OBS
- on-board service
- OCS
- Occupancy Control System
- ONR
- Ontario Northland Railway
- RAC
- Railway Association of Canada
- RTC
- rail traffic controller
- TC
- Transport Canada
- TSB
- Transportation Safety Board of Canada
- VIA
- VIA Rail Canada Inc.