Main-Track Derailment
Canadian National
Train N0 M-365-21-20
Mile 9.58, Saint-Maurice Subdivision
Cressman, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 22 May 2000, at approximately 0152 eastern daylight time, 23 cars of eastbound Canadian National train N0 M-365-21-20 derailed at Mile 9.58 of the Saint-Maurice Subdivision, near Cressman, Quebec. Six of the derailed cars were empty tank cars that had recently contained dangerous goods; three of them fell into the Saint-Maurice River. Four hundred feet of track was destroyed and two spans of the railway bridge across the river were heavily damaged. There were no injuries and no permanent environmental damage.
Ce rapport est également disponible en français.
Factual information
On 21 May 2000, the train departed Parent, Quebec, at 2127 eastern daylight time (EDT)Footnote 1 with 3 locomotives and 159 cars, including 128 loaded cars, 19 empty cars and 12 empty tank cars that had recently contained gasoline (UN 1203) or heating oil (UN 1202). The train was about 9 586 feet long and weighed approximately 15 230 tons.
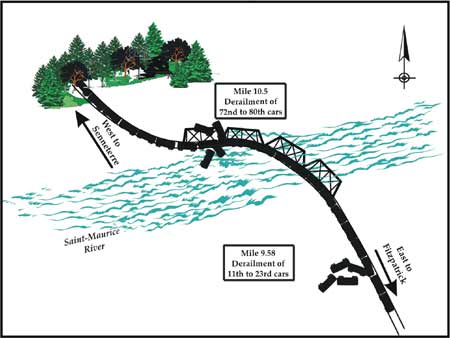
At about Mile 9.5, the train experienced an undesired emergency brake application. The event recorder indicates that, at the time of the emergency brake application, the train was travelling at 29 mph and the throttle was in the No 2 position. After the train came to a stop, the crew carried out the emergency procedures prescribed by regulations and the conductor went to the tail end to determine the cause of the emergency brake application. He found that 13 gondola cars (11th to 23rd cars), loaded with wood chips, had derailed at Mile 9.58. Canadian National (CN) subsequently received a call indicating that one tank car was floating in the Saint-Maurice River. Personnel at the site discovered that nine other cars (72nd to 80th cars), including two covered cars loaded with paper, one empty hopper car, and six empty tank cars that had recently contained gasoline (UN 1203) or heating oil (UN 1202), also had derailed on the bridge over the Saint-Maurice River at Mile 10.15 (see Figure 1). Two tank cars were punctured, but only a minimal quantity of product spilled into the river. No one was injured as a result of the accident.
Some 400 feet of track was destroyed and two spans of the bridge were heavily damaged. One hopper car, 2 covered cars, 13 gondola cars and 6 tank cars were damaged. The hopper car was destroyed. All the damaged tank cars were 111A cars—the head of the tank on two of the tank cars was punctured, the head of the tank on another was deformed, and the shell of the three others was deformed. Damage to the top fittings was noticed on one of the tank cars.
The hopper car and the empty tank cars were placed near the middle of the train (74th to 80th cars). The weight ahead of these cars was approximately 7 000 tons, and the weight behind was approximately 8 700 tons. The hopper car and three tank cars fell off the bridge and another tank car was left hanging from the bridge structure (see Figure 2). The hopper car was a cylindrical pressure-flow car with three outlet valves and no centre sill, and was constructed of 3/16-inch plate, Class AAR C-612.

The Saint-Maurice Subdivision extends from Fitzpatrick (Mile 0.0) to Senneterre (Mile 256.9). It consists of a single main track. Train movements are governed by the Occupancy Control System (OCS) in accordance with the Canadian Rail Operating Rules (CROR), and are supervised by a rail traffic controller (RTC) based in Montréal, Quebec.
In the accident area, the track is Class 3 and the maximum authorized speed is 40 mph for passenger trains and 30 mph for freight trains. The track runs northwest/southeast, and has a downward grade to the east of 0.2 per cent between Mile 10.5 and Mile 9.5. There are several curves on both sides of the accident site. The track was mostly made up of partly worn rail from various sources. The rails were laid on double-shouldered tie plates secured by four spikes per tie. The north rail consisted of 100-pound rail in jointed, 78-foot lengths, and the south rail was 100-pound continuous welded rail.
The north rail had failed in a three-degree, right-hand curve at Mile 9.58. Pieces of the broken rail were recovered and sent to the TSB Engineering Laboratory. Examination revealed that the rail failure occurred when the head of the rail separated from the web (TSB Engineering Laboratory report LP 050/00). The failure started with a crack originating in an elongated inclusion of manganese sulphide, then propagated transversely to the rail web, then longitudinally. This type of failure is typical of a vertical split head (VSH). Oxidation in the rail section indicates that the vertical separation had existed for several months. The VSH led to subsidence of the running surface of the rail over a distance of 1.78 m, and created a flattened area on the rail head that was visible to the naked eye.
The rail was 100-pound Dominion MRC ARA HF, and was cast in 1943. It was a partly worn rail whose lay date and accumulated tonnage are unknown. The use of partly worn rails is common practice in the industry. In principle, the procedures for rail recovery, as set out in CN's Standard Practice Circular (SPC) 1303, "Classification of Rail," take into account rail wear but not accumulated tonnage.
Vertical wear of the rail head was 1/4 inch (7 mm), which is the limit set out in SPC 3200. CN had planned to replace the rail due to head wear in its 2000 maintenance program.
The area foreman inspected the portion of track where the derailment occurred on 20 May 2000, two days before the accident. His last previous inspection was on 18 May 2000. During these two inspections, the foreman found no exceptions in the area of Mile 9.5.
The rail flaw detection car inspected the derailment area on 19 May 1999 and 08 October 1999. During these inspections, it detected several internal defects such as VSHs and progressive transverse fissures. The last inspection revealed a transverse fissure at Mile 9.42 and VSHs at Mile 9.61 and Mile 9.64. Visual inspections between the last rail flaw detection car test and the derailment revealed two more identical defects in the derailment area.
In accordance with the SPCs and Transport Canada's Railway Track Safety Rules, rails must be tested at least once a year for Class 3 tracks used by passenger trains. However, on the Saint-Maurice Subdivision, rails are inspected by the rail flaw detection car twice a year. Rail testing frequency is generally determined by risk analysis based on the type of traffic and track history. For example, the testing frequency is increased when traffic increases, when more internal defects are found, or when the rail is worn or close to its fatigue resistance.
A rail test was to be done four days before the accident but was postponed because the equipment was not available.
Analysis
This accident actually consisted of two separate derailments that occurred almost simultaneously. Analysis by the TSB Engineering Laboratory revealed that the low rail in the curve at Mile 9.58 failed due to a VSH. This failure led to the derailment of the lead cars (11th to 23rd cars) in the train.
The VSH originated as cracks initiated by inclusions. It was not recent, and had progressed over a period of time; however, it was not detected because it was probably not long enough when the last rail test was done about seven months before.
The frequency of testing with the rail flaw detection car was increased due to the specific characteristics of the track (growing number of internal defects, worn rail). However, these special measures taken by CN to control rail breaks were insufficient because, once VSHs are initiated, they propagate rapidly.
Since the rail involved in this accident was a partly worn rail, information on its accumulated tonnage was not available because the procedures for rail recovery and classification are based on rail wear, not accumulated tonnage. Since the behaviour of a rail under fatigue depends largely on accumulated tonnage, accumulated tonnage data would have provided an additional indicator of rail condition and permitted a more effective risk assessment and rail testing planning more appropriate to the actual characteristics of this portion of track.
Defects such as VSHs can sometimes be detected because the attendant subsidence of the running surface is visible when one concentrates specifically on examining for that phenomenon. However, this level of concentration cannot be sustained indefinitely because, when inspectors are doing bi-weekly track inspections from hi-rail vehicles, they must do many different visual inspections simultaneously (rails, rail joints, rail anchors, ties, tie plates, spikes, ballast, turnouts, crossings, signal equipment, drainage, ditches and embankments, fences, and clearances). Separate inspections are done on turnouts and crossings, but all the other items must be inspected simultaneously while travelling at speeds of 15 to 20 mph on the hi-rail vehicle. When people must perform more than one task at a time, their performance on at least one of the tasks is diminished. People can keep track of five to nine items of information at a time; however, if several concurrent tasks require the use of the same faculty, for example vision in the case of track inspectors, this number will decrease. As a result, visual signs like those that indicate a VSH can escape the attention of the inspector and will not always be detected.
Moreover, since the rails were to be replaced that year and the track was to be tested soon by the rail flaw detection car, it is likely that the inspectors' attention was unconsciously diverted to other infrastructure elements instead of the visual signs of the VSH.
The derailment of the 72nd to 80th cars was a result of the first derailment, which occurred at the head end of the train. When the 11th to 23rd cars derailed on the broken rail, the emergency brakes applied. The empty cars in the middle of the train were caught between the block of loaded cars at the head of the train, which were decelerating due to the braking force generated by emergency braking, and the sudden pile-up of the derailed cars and the cars behind them, whose brakes had not yet been applied. Due to the weight of the block of cars in the tail end of the train and the speed they were travelling, the resultant inertia applied high compression forces to the couplers, which led to the second derailment. Since the hopper car was empty and of light construction and had no centre sill, it was more vulnerable and consequently yielded first. Based on the damages observed on the hopper car, it was deformed by compression forces, was lifted, and struck the top chord of the bridge superstructure; the tank cars behind the hopper car piled on top of it, damaging the bridge structure and the covered cars further ahead.
The position of the heavy cars towards the end of the train affected the level of forces generated along the train. A train configuration that would take into account the dynamics of the train would allow more effective control of the forces generated and would reduce the risk of derailment in the event of undesired braking.
Findings
Findings as to causes and contributing factors
- The train derailed when the low rail in the curve failed as a result of a vertical split head (VSH).
- The VSH was not recent; however, it was not detected because it was probably not long enough when the last rail test was done about seven months before.
- The special measures taken by CN to control rail breaks were insufficient because, once VSHs are initiated, they propagate rapidly.
Other findings
- Accumulated tonnage data can provide an additional indicator of rail condition and permit a more effective risk assessment and rail testing planning more appropriate to the track characteristics.
- Since inspectors must perform many visual inspections concurrently, visual signs like those that indicate a VSH can escape their attention and are not always detected in bi-weekly inspections.
- The derailment of the 72nd to 80th cars was a result of the first derailment at the head of the train.
- A train configuration that would take into account the dynamics of the train would allow more effective control of the forces generated and would reduce the risk of derailment in the event of undesired braking.
Safety action
Safety action taken
After the accident, Transport Canada (TC) increased its monitoring on the Saint-Maurice Subdivision. On 08 May 2002, TC sent a Notice to CN on the track condition. Furthermore, CN reduced the speed on certain sections of track and is regularly inspecting the track between Fitzpatrick and Parent (Mile 118.9). CN will replace 21 miles of track on that subdivision in 2002.
TC and the railway industry have agreed to form a working committee that will include union representatives. The committee has to determine if changes to the Railway Track Safety Rules and to the methods used by the industry are required. The committee will examine issues such as rail testing frequency and parameters to evaluate track conditions.
As for train configuration, TC recognizes that, by taking into account the train dynamics, the forces generated will be more effectively controlled in the event of undesired braking, thereby reducing the risk of derailment. Several stakeholders, including TC, have started discussions to initiate a research project on the subject. The goal of this project, entitled "Train Dynamics Simulator," is to create a simulator to assess the dynamics parameters on train movements to determine the impact on trains, cars and track. As a result of the project, new regulations could be established and action could be taken to reduce the risks related to train dynamics.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .