Loss of control during night approach and near collision with terrain
Helijet International Inc.
Sikorsky S-76C+ (helicopter), C-GHHJ
Tofino/Long Beach Airport, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 15 November 2015, at 0135 Pacific Standard Time, the Helijet International Inc. Sikorsky S-76C+ helicopter (registration C-GHHJ, serial number 760500) departed at night from Vancouver International Airport, British Columbia, on a night visual flight rules medical evacuation flight to Tofino/Long Beach Airport, British Columbia, with 2 paramedics and 2 pilots on board. While conducting a visual approach to Runway 29, the crew disengaged the autopilot at an altitude of 600 feet above sea level and manoeuvred toward the planned landing area. At approximately 0239, on short final, the helicopter's airspeed slowed, a high rate of descent developed, rotor speed began to decrease, and directional control was lost. Control was re-established over a beach, after the helicopter had descended to approximately 3 feet above ground level, and approximately 67 feet below the airfield elevation at Tofino/Long Beach Airport. The pilots then observed normal engine and drivetrain parameters and climbed to 500 feet above sea level to conduct a second approach. During this approach, additional control difficulties were encountered, but the helicopter was able to land. There were no injuries, there was no fire, and the emergency locator transmitter was not activated.
1.0 Factual information
The International Civil Aviation Organization's (ICAO's) Annex 13 requires states conducting accident investigations to protect cockpit voice recordings. Footnote 1 Canada complies with this requirement by making all on-board recordings —including cockpit voice recorders (CVRs)—privileged in the Canadian Transportation Accident Investigation and Safety Board Act. While the TSB may make use of any on-board recording in the interests of transportation safety, it is not permitted to knowingly communicate any portion of an on-board recording that is unrelated to the causes or contributing factors of an accident or to the identification of safety deficiencies.
The reason for protecting CVR material lies in the premise that these protections help ensure that pilots will continue to express themselves freely and that this essential material is available for the benefit of safety investigations. The TSB has always taken its obligations in this area very seriously and has vigorously restricted the use of CVR data in its reports. Unless the CVR material is required to both support a finding and identify a substantive safety deficiency, it will not be included in the TSB's report.
To validate the safety issues raised in this investigation, the TSB has made use of the available CVR information in its report. In each instance, the material has been carefully examined in order to ensure that it is required to advance transportation safety.
1.1 History of the flight
On 15 November 2015, at approximately 0135, Footnote 2 during the hours of darkness, C-GHHJ departed Vancouver International Airport (CYVR) on a medical evacuation (medevac) flight to Tofino/Long Beach Airport (CYAZ), British Columbia, in response to a call from the Critical Care Coordinator of British Columbia Emergency Health Services (BCEHS).
Before the flight, the flight crew, consisting of 2 captain-qualified pilots, had reviewed the weather, prepared the helicopter for the flight to CYAZ (which was scheduled to last 1 hour and 5 minutes Footnote 3), and filed a night visual flight rules (NVFR) flight plan.
The designated captain occupied the left-hand seat and was the pilot monitoring (PM). The designated first officer was seated in the right-hand seat and was the pilot flying (PF). Footnote 4
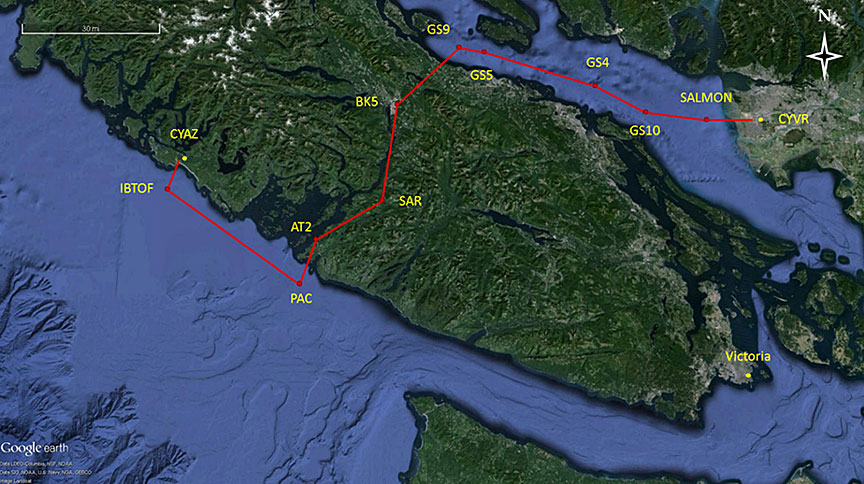
During the initial climb to 2500 feet above sea level (ASL) on the company-approved NVFR route (Figure 11), the flight crew discussed the limited visibility due to darkness. However, the clouds and reported visibility at the time met regulations for NVFR flight. Footnote 5
At 0155, BCEHS dispatch advised the flight crew that Turboflares Footnote 6 had been set up at the CYAZ temporary night helipad, and ground personnel were reporting that the weather was good with a few stars visible.
At approximately 0222, before crossing waypoint A Footnote 7 (Figure 1), the flight crew loaded and activated the global positioning system (GPS) area navigation (RNAV) global navigation satellite system Footnote 8 Runway 29 approach for CYAZ (Appendix A). Footnote 9 At this point, the crew deviated from the approved NVFR route to follow the published RNAV approach route and maintain a safe profile above terrain and obstacles during the approach to the airport. This is sometimes also done for the purpose of maintaining instrument flight rules (IFR) proficiency.
At 0224, the PF called for the initial approach checks. The PM read the initial approach checklist, confirming that the parking brake was in the OFF position and the radio altimeter low-height bugs were set to 200 feet. The PM asked the PF for a landing briefing, and the PF replied that they would be landing on the runway in front of them. The PM agreed and completed the checklist, which included checking the digital engine control unit (DECU).
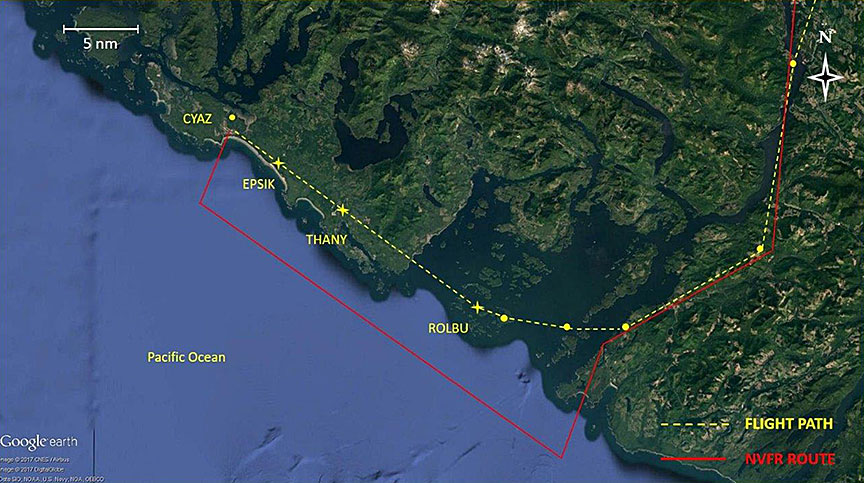
At 0232, the PF started to slow the helicopter and began a descent to 900 feet ASL. One minute later, the PM completed the final approach checklist. After crossing waypoint EPSIK (Figure 2) at 0237:06, the helicopter continued to slow and descend, levelling at 620 feet ASL as the PF maintained speed at 85 knots indicated airspeed (KIAS).
At 0238:18, the PM stated that the missed-approach point Footnote 10 was located at the threshold of Runway 29 and was visible on the helicopter's enhanced vision system (EVS) Footnote 11 screen. On 3 separate occasions, the crew discussed the fact that the landing spot was indicated by a flashing green light.
At 0239:01, the PF disengaged the autopilot, and the helicopter began to decelerate while maintaining a constant altitude. At 0.3 nm from the threshold of Runway 29, the helicopter's airspeed decreased below 60 KIAS (approximately VMINI Footnote 12), and its pitch attitude increased beyond 14° nose-up. The PF commented that they were closer to the flashing green light than expected and lowered the collective to minimum power. The helicopter began to descend quickly, and the indicated airspeed decreased to near zero.
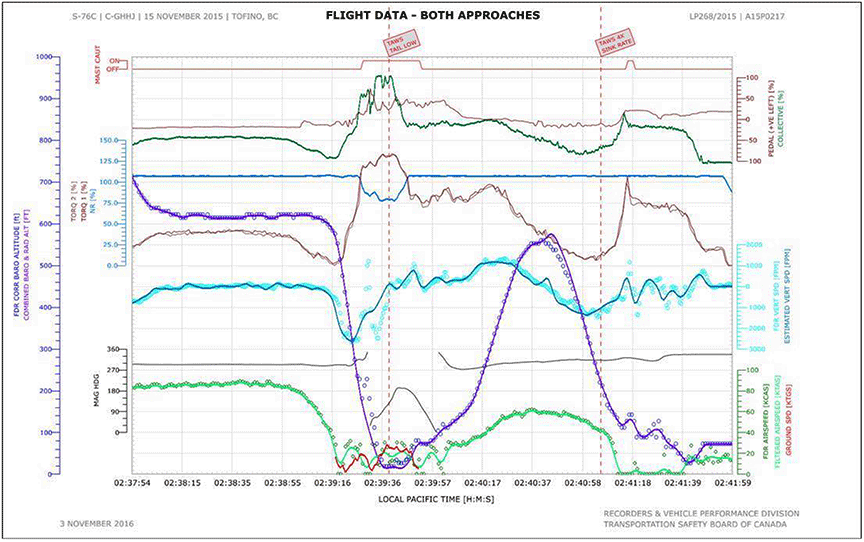
At 0239:19, the helicopter descended through 500 feet above ground level (AGL) radar altitude (Figure 3), triggering the enhanced ground proximity warning system (EGPWS) Footnote 13 voice alert of "FIVE HUNDRED." As the helicopter's descent rate increased through 2000 feet per minute (fpm), the PF asked the PM to monitor the rate of descent, and the PM alerted the PF that the airspeed was low.
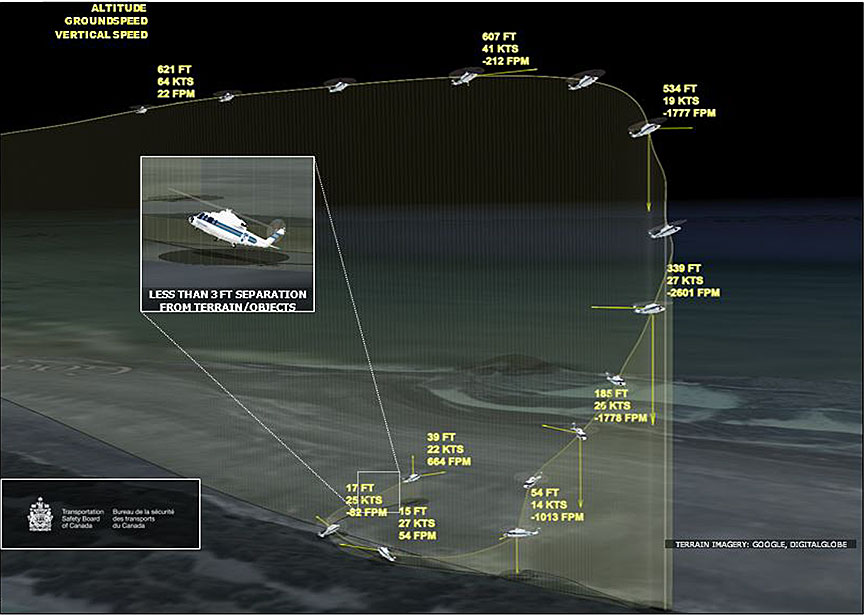
The helicopter descended through 300 feet AGL with a descent rate of approximately 2600 fpm. During the lower portion of the descent, with an aircraft heading of approximately 290°, the helicopter began flying backwards at about 20 to 25 knots and then started to yaw to the right. The main rotor rpm (NR) Footnote 14 decreasedfrom the normal governed value of 107%, and the engine torques were increasing to 100%.
At 0239:26, the EGPWS gave a voice alert of "TWO HUNDRED." The NR was decreasing through 89%, and the engine torques were increasing through 120%. The nose continued to yaw to the right, and the helicopter began to fly sideways and to the right. The descent continued, and the EGPWS gave a voice alert of "ONE HUNDRED." During that time, nearly full left-pedal input was being applied, but the yaw rotation continued to a heading of approximately 185° (approximately 255° right of the inbound course). Because the nose rotated to the direction in which the helicopter was moving, the airspeed began to increase, and the helicopter continued to descend through 50 feet AGL.
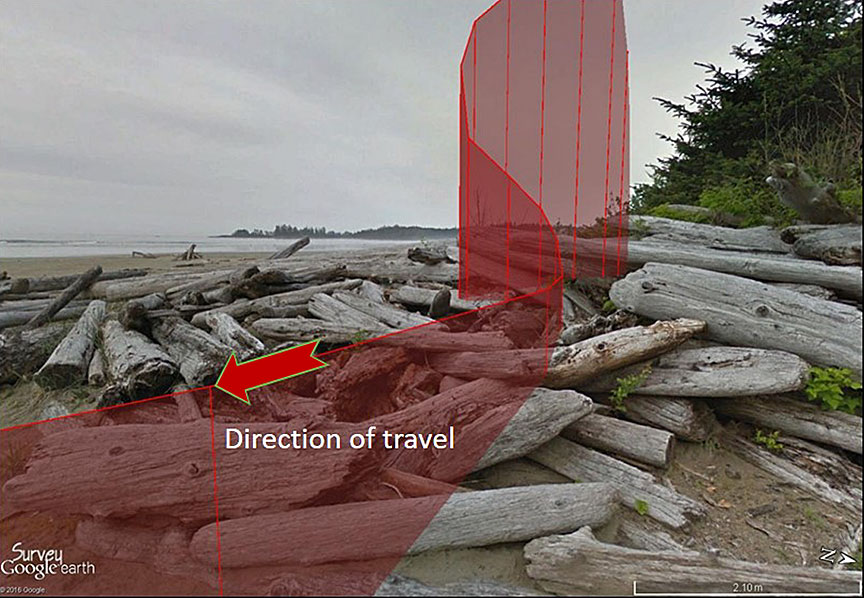
The PF increased the collective to the full-up position, and the engine torques reached 134% while the NR dropped to 77%. The helicopter passed along the foreshore at approximately 15 to 25 knots while at nearly 0 radar altitude (approximately 65 feet below the airfield elevation of 80 feet ASL). The terrain below the helicopter at this point consisted of bushes at the edge of the foreshore and large logs washed up against the beach embankment.
At 0239:39, with a pitch attitude of 11° nose-up, the EGPWS gave a voice alert of "TAIL TOO LOW."
The helicopter stopped descending at about 3 feet above the logs on the beach (Figure 4). The crew acknowledged that the flight parameters had returned to the normal operating range, with no caution or warning lights visible, and the captain confirmed that he had taken control as PF. The helicopter's airspeed increased, and the aircraft climbed away from the beach in a southerly direction.
The flight crew manoeuvred the helicopter back toward the temporary night helipad at CYAZ, climbing to 550 feet ASL with an airspeed of 60 knots. All engine parameters were indicating in the normal operating range during the short flight.
During the second approach to the temporary night helipad, the helicopter again began to descend rapidly. The EGPWS gave additional voice alerts of "MINIMUMS, MINIMUMS" and "SINK RATE, SINK RATE" as the vertical descent speed reached 1400 fpm. The PF arrested the descent and landed the helicopter on the temporary night helipad at 0241:44.
The flight crew completed the shutdown procedure, which included checking the maintenance page in the integrated instrument display system (IIDS) for engine performance exceedances. The IIDS did not display any exceedances or warnings.
After the flight crew and paramedics exited the helicopter, the captain noticed oil on the left side of the helicopter's fuselage. Maintenance personnel in Vancouver were contacted, and the medevac mission was cancelled. The Transportation Safety Board of Canada (TSB) was subsequently notified of the occurrence.
1.2 Injuries to persons
There were no injuries.
1.3 Damage to aircraft
The post-flight inspection revealed a significant quantity of oil on the helicopter's main rotor blades and on the left side of the fuselage. Company personnel were consulted and subsequently dispatched to CYAZ. On further inspection, it was determined that each of the main rotor spindles had come into contact with the elastomeric blade retention bearings on the main rotor hub and that a main rotor damper oil line had been broken.
Maintenance personnel changed the main rotor spindles as well as the damaged damper oil line. The cockpit voice and flight data recorder (CVFDR) was disabled to prevent overwriting of the data from the occurrence flight. A different flight crew carried out a test flight, and the helicopter was flown back to CYVR, where the company removed the CVFDR and forwarded it to Maxcraft Avionics Ltd. (Maxcraft) to download the flight and voice data. The helicopter was returned to active flight operations at BCEHS on 16 November 2015.
On 16 November, Maxcraft provided the company with the information downloaded from the CVFDR. The information showed that both engines experienced torque values in excess of 155% per engine, for a combined total of over 310%, during the recovery from the helicopter's initial loss of control on the first approach to CYAZ. Furthermore, during the occurrence, the torque value on the number 1 engine had exceeded 135% for 15 seconds, and the torque value on the number 2 engine had exceeded 135% for 13 seconds. These values indicated that the manufacturer's Footnote 15 maximum allowable combined dual-engine transient limit of 230% torque for 10 seconds had been exceeded.
On 25 November 2015, Helijet notified the TSB of another occurrence involving C-GHHJ (TSB aviation occurrence A15P0237). A helicopter flight crew had been preparing to depart CYVR on a medevac flight to Chemainus, British Columbia. When the collective was raised to lift off from the helipad, there was a high-frequency vibration in the flight controls and an abnormal noise. The vibration and noise ceased when the collective was lowered. Another attempt to take off was made, and a similar vibration and noise were noted. The helicopter was taxied back to the hangar, and maintenance personnel were consulted. Footnote 16
After learning of the aborted takeoff, the TSB contacted the helicopter manufacturer and provided a description of the events that had preceded it, together with the flight data recorder (FDR) data from the 15 November occurrence. The manufacturer had not been informed of the torque exceedances and low in-flight rpm values that the helicopter had been subject to in the 15 November occurrence.
The manufacturer subsequently deemed the helicopter not airworthy and required the helicopter to be removed from service until all dynamic components had undergone inspection and overhaul maintenance procedures. Upon further inspection of the dynamic components for possible damage, the maintenance organization concluded that there were "no major findings due to the overtoque [sic] incident." Footnote 17 The manufacturer also required each main rotor blade to be inspected and tested for bonding separation, with specific direction to ultrasonically inspect each blade at the root end where the laminates were bonded to the spar. During the course of these inspections, it was established that 1 of the 4 main rotor blades had experienced bonding separation on its lower surface.
On 26 November, the helicopter's CVFDR was secured and sent to the TSB Engineering Laboratory for data download and analysis. The analysis revealed that incorrect conversion factors had been applied when the data was first downloaded.
The TSB laboratory analysis established that, during the occurrence flight, a maximum peak engine-torque value of 134% per engine (for a combined engine torque of 268%) had occurred. It was also determined that, during the occurrence, the NR droop from 107% lasted a total of 19 seconds, reaching a minimum of 77% NR (Appendix B).
There is no normal or emergency in-flight procedure for a torque exceedance. The manufacturer does not require in-flight corrective action following a torque exceedance, but it does require maintenance action after the flight.
1.4 Other damage
There was no damage to property or objects.
1.5 Personnel information
1.5.1 General
| Captain | First officer | |
|---|---|---|
| Licence | Airline transport pilot licence – helicopter | Airline transport pilot licence – helicopter |
| Medical expiry date | 01 May 2016 | 01 May 2016 |
| Total flying hours | 6500 | 3772 |
| Total hours on type | 4500 | 806 |
| Total night-flying hours | 595 | 482 |
| IFR hours | 720 | 450 |
| Hours, last 7 days | 4 | 1 |
| Hours, last 30 days | 24 | 5 |
| Hours, last 90 days | 89 | 56 |
| Hours on duty prior to occurrence | 6 | 6 |
| Hours off duty prior to work period | 12 | 12 |
1.5.2 Captain
1.5.2.1 General
The captain was certified and qualified for the flight in accordance with existing regulations. The captain held a Canadian airline transport licence—helicopter, with type ratings on the Bell 206, Bell 47, McDonnell-Douglas 300, Robinson R22, and Sikorsky S-76. The captain's licence was endorsed with a Group 4 instrument rating, valid until 01 March 2017.
Before joining Helijet, the captain had accumulated IFR experience flying the Sikorsky S-76 overseas. In 2003, the captain received an airline transport pilot licence while working for another Canadian helicopter operator.
The captain was hired on a casual basis in February 2008 and became a full-time employee of the company in March 2009.
1.5.2.2 Company training
In February 2015, the captain underwent annual recurrent training and a pilot proficiency check (PPC) using a Sikorsky S-76C, full-motion, level D hydraulic flight simulator.
In April 2014, the captain completed a full-day course consisting of training on pilot decision making, crew resource management (CRM), and controlled-flight-into-terrain avoidance. Helijet did not offer NVFR approach training or black-hole training.
1.5.2.3 Work schedule
Air ambulance pilots at Helijet work either day shifts or night shifts. The night shifts are 12 hours long (1830 to 0630, or 2030 to 0830), and pilots rotate from day to night shifts on the day after the end of a day shift (for example, if the pilot's day shift ends on Tuesday, the pilot would rotate to the night shift beginning on Wednesday). Pilots are assigned to as many as 3 consecutive night shifts, for which crew sleeping quarters are provided. The night shift schedule is consistent with recommended fatigue management practices, whereby night shifts are shared among pilots based on rapid rotation, changing every few days. Footnote 18
The captain's flight and duty time limits were not exceeded. The captain had worked from 2030 to 0830 on the nights of 12 and 13 November 2015. During each of those 2 nights, the captain had obtained approximately 5 hours of sleep in crew quarters, accruing a sleep debt Footnote 19 of about 5 hours over both nights combined. On 14 November, the captain took an afternoon nap, started the duty shift at 2030, and had a 1-hour nap in the crew quarters before receiving the initial dispatch call. The flight was conducted at a period of low circadian rhythms. Footnote 20 The level of the captain's sleep debt, taking into consideration the amount of sleep obtained before the flight, was not sufficient to establish that the captain was fatigued at the time of the occurrence.
1.5.3 First officer
1.5.3.1 General
The first officer was certified and qualified for the flight in accordance with existing regulations, and held a Canadian airline transport pilot licence—helicopter, with type ratings on the Sikorsky S-61 and S-76. The first officer's licence was endorsed with a Group 4 instrument rating, valid until 01 March 2017.
The first officer joined Helijet in November 2013. Before joining Helijet, the first officer had no previous commercial helicopter flight experience. From 1998 to 2012, the first officer accumulated flight experience on the CH-124 Sea King helicopter with the Department of National Defence (DND). The first officer's experience with DND included numerous operational deployments and roles as an instructor pilot and crew commander. The first officer had also been involved in the oversight and professional development of junior pilots.
On 21 November 2013, the first officer received the Sikorsky S-76 type rating and a Group 4 IFR rating from Helijet. On 16 February 2014, the first officer upgraded to captain on the S- 76C+ and was the assistant chief pilot from July 2014 to August 2015. The first officer was a company training pilot and a Transport Canada–approved check pilot (ACP).
1.5.3.2 Company training
In September 2015, the first officer underwent annual recurrent training and a PPC using a Sikorsky S-76C, full-motion, level D hydraulic flight simulator. In August 2015, the first officer received a full-day course consisting of training on pilot decision making, CRM, and controlled-flight-into-terrain avoidance. Helijet did not offer NVFR approach training or black-hole training.
1.5.3.3 Work schedule
During the week before the occurrence, the first officer was in West Palm Beach, Florida, to administer simulator training and to conduct PPCs of company pilots. The first officer returned to Vancouver from West Palm Beach at approximately 2100 on 10 November 2015.
The first officer's flight and duty time limits were not exceeded. The first officer had worked a night shift from 2030 to 0830 on 13 November 2015, with about 5 hours of sleep in crew quarters, accruing a sleep debt of about 3 hours. On 14 November 2015, the first officer took an afternoon nap, started duty at 2030, and had 1.5 hours of sleep in crew quarters before the initial dispatch call. The flight was conducted during a period of low circadian rhythms. The level of the first officer's sleep debt, taking into consideration the amount of sleep obtained prior to the flight, was not sufficient to establish that the first officer was fatigued at the time of the occurrence.
1.6 Aircraft information
1.6.1 General
Records indicate that the helicopter was certified, equipped, and maintained in accordance with existing regulations and approved procedures. The helicopter had no known deficiencies before the flight and was being operated within its load and centre of gravity limits. The investigation found no indication that the helicopter had encountered any type of system-related malfunction during the flight.
| Manufacturer | Sikorsky |
|---|---|
| Type, model, and registration | S-76C+, C-GHHJ |
| Year of manufacture | 1995 |
| Serial number | 760500 |
| Certificate of airworthiness / flight permit issue date | 12 August 2011 |
| Total airframe time | 8023:58 |
| Engine type (number of engines) | Turbomeca Arriel 2S1 (2) |
| Maximum allowable take-off weight | 5307.03 kg |
| Recommended fuel type(s) | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A |
The occurrence helicopter is shown in Figure 5.

1.6.2 Description
The Sikorsky S-76 helicopter was designed and manufactured by Sikorsky Helicopter Corporation. Its U.S. Federal Aviation Administration (FAA) certification was awarded in November 1978, and Canadian certification followed. The S-76C type was awarded certification in 1991. It has a maximum takeoff weight of 5307.03 kg (11 700 pounds), a maximum speed of 155 knots, and a range of approximately 400 nm. The S-76C+ is equipped with the Turbomeca Arriel 2S1 engine and full-authority digital engine controls.
1.6.3 Helicopter performance
1.6.3.1 Exceedance of torque and powertrain limits
For dual-engine, power-on operation, the rotorcraft flight manual (RFM) gives minimum and maximum NR limits as follows:
- Continuous operation: minimum 106%, maximum 108%
- Transient operation: minimum 91%, maximum 109% (for up to 20 seconds)
In this occurrence, the NR was below 106% for a total of 19 seconds, and below 91% for 15 seconds.
For dual-engine, power-on operation, the RFM gives maximum torque limits per engine as follows:
- Continuous operation: 104%
- Transient operation: 160% (for up to 20 seconds)
In this occurrence, during the first approach (the loss-of-control event), both engine torques exceeded the continuous limit for 19 seconds and peaked at 134%. The peak did not exceed the transient limit.
With regard to the transmission, the RFM gives maximum torque limits for dual-engine operation as follows:
- Continuous operation: 100% input from each engine (200% combined)
- Transient operation: 115% input from each engine, for up to 10 seconds (230% combined)
In this occurrence, both engines were operating and producing nearly equal amounts of torque. The torque that each engine was producing was above 100% for 19 seconds, and above 115% for 16 seconds. In this occurrence, the combined torque peaked at 268%.
The Sikorsky S-76 Maintenance Manual states:
During dual-engine operations, transient overtorque is permissible up to torquemeter readings of 115% output torque for periods of not over 10 seconds for any single instance.
[…]
A main gear box that has operated beyond limits […] must be inspected. Contact Sikorsky Aircraft Commercial Product Support for instructions before further flight. Footnote 21
The occurrence helicopter does not have a system to capture and provide alerts of torque exceedances.
The RFM also gives engine limits for turbine temperature (T5), compressor speed (N1), and power turbine speed (N2); however, of these 3 parameters, only N2 was recorded on the FDR. The N2 values for each engine closely matched the NR, as expected.
The RFM gives the minimum limits for N2 as follows:
- Continuous: 90.5%
- Transient: 68% (up to 20 seconds, for one-engine-inoperative landing only)
In this occurrence, N2 was below 90.5% for a total of 15 seconds, and the lowest value was 77%. Therefore, the minimum continuous limit was exceeded while the minimum transient limit was not applicable for dual-engine operations.
Because T5 and N1 were not recorded on the FDR, it could not be determined whether their respective limits were exceeded.
A table showing the helicopter's powertrain limits and their exceedances is provided in Appendix C.
The data gathered from the occurrence helicopter indicate that the NR and engine torques were consistent with the collective control input and the design of the DECU. The DECU features a blowaway mode that allows dual-engine torque to exceed normal limits in the event of a significant decrease in NR. This mode is triggered when either of the following 2 conditions is met:
- a slow to moderate decay in NR to 100%, or
- a decay rate of 5% per second or greater when NR is at 104% or less.
Once the blowaway mode has been triggered, the engines provide torque up to the single-engine limit of 115%, or until the 2-minute single-engine N1 limit is reached, whichever occurs first. If NR falls below 90%, the engine torque limit is raised to 140%. While the blowaway mode is operating, the DECU also maintains N1 values within limits. If the 2-minute single-engine limit is reached, this event is logged and counted on the DECU digital readout or IIDS as a cue for appropriate maintenance action.
The data retrieved from the DECU for examination by the engine manufacturer indicated that no limits had been exceeded and --single-engine limits had been activated. The engine manufacturer's analysis indicated that no N1 limits had been exceeded.
1.6.3.2 Yaw control
In this occurrence, during the period of high engine torque, low NR, and rearward flight, the helicopter yawed to the right. This right yaw continued even when nearly full left-pedal input was applied to the tail rotor. Simplified estimates suggest that the tail rotor thrust required to control yaw with 134% engine torque is about 56% higher than that required for the out-of-ground-effect hover (Table 3). This demand exceeded the maximum capability of the tail rotor, because it required blade pitch values in excess of the mechanical limits.
| Scenario | Engine torque | Rotor speed (NR) | Required tail rotor thrust (pounds) | Estimated tail-rotor blade pitch |
|---|---|---|---|---|
| OGE hover, 11 000 pounds | 85% | 107% | 880 | 19° |
| Maximum torque case | 100% | 107% | 1030 | 21° |
| Overtorque case | 134% | 107% | 1380 | 27° |
| Occurrence case | 134% | 77% | 1380 | 46° |
Note: These results are from a simplified analysis performed by the TSB to estimate the approximate tail rotor thrust and blade pitch required for various hover conditions, and to compare relative differences between these cases. Actual values may differ.
An additional factor that may have further reduced yaw control was the helicopter's flight rearward and slightly to the right.
1.6.4 Helicopter systems
1.6.4.1 Full-authority digital engine controls
The S-76C+ includes a feature built into the full-authority digital engine controls that protects the engine and the main gearbox by preventing the pilot from exceeding posted limits during normal operations. The system is designed to limit fuel flow when either the all-engines-operating torque limit or the temperature limit is reached. If either of these conditions occurs, the reduced fuel flow causes the NR to decrease. However, these limits can be shifted upward via the blowaway logic when additional power is required in extreme flight conditions.
1.6.4.2 Enhanced ground proximity warning system
The occurrence helicopter was equipped with a Honeywell Mark XXII EGPWS, which meets the Canadian Technical Standard Order C151b Class A requirements for terrain awareness and warning systems. According to the manufacturer,
The MK XXII uses altitude rate from the Air Data Computer and Radio Altitude to detect when the aircraft is descending toward terrain at a high rate for its relative altitude above terrain. The MK XXII will provide alerting and warning to the pilot. Footnote 22
The Honeywell Mark XXII EGPWS has 6 modes that provide warnings when the aircraft may conflict with the terrain as recorded in its internal map or database. Footnote 23
During the occurrence sequence, modes 1 and 6 were triggered.
1.6.4.2.1 Mode 1: Alerting and warning of excessive rate of descent
Mode 1 of the EGPWS is triggered based on the rate of descent and the radio altitude (Figure 6). If the helicopter enters the yellow "alerting" envelope, a voice alert of "SINK RATE" will be heard and an amber caution annunciator lamp will illuminate. If the high rate of descent continues, the "SINK RATE, SINK RATE" voice alert will be repeated at an increasing frequency. If the helicopter enters the red "warning" envelope, the voice alert "PULL UP" will be played continuously, and the red warning annunciator lamp will illuminate. According to the manufacturer, "In both cases, as the pilot reacts to decrease the high rate of descent and the aircraft flight path exits the alerting/warning envelope, the annunciator lamp will extinguish and the voice alerts will cease." Footnote 24
During the occurrence, no "SINK RATE" or "PULL UP" warnings were activated on the first approach to CYAZ due to the autorotation Footnote 25 inhibit function Footnote 26 that was configured when the EGPWS was initially set up. When engine torque values fall below 7.5% torque, Mode 1 of the EGPWS is inhibited until engine torque values increase above 7.5% and the helicopter is out of the autorotation. The EGPWS then takes 20 seconds to reset before additional "SINK RATE" and "PULL UP" alerts can be activated.
![Enhanced ground proximity warning system mode 1: Alerting of excessive rate of descent (Source: Honeywell International Inc., 060-4314-200, <em>MK XXII Helicopter EGPWS Pilot Guide</em>, Rev. C [March 2004], with TSB annotations showing flight profile)](/sites/default/files/eng/rapports-reports/aviation/2015/a15p0217/images/a15p0217-figure-06.png)
1.6.4.2.2 Mode 6: Altitude call-outs, excessive bank angle, tail strike
Mode 6 of the EGPWS provides aural callouts for descent below predefined altitudes and minimums. In this mode, no caution or warning lights are illuminated. The actual callouts are selected from a menu when the system is installed.
The EGPWS installed on the occurrence helicopter was configured to provide aural altitude callouts at 500 feet AGL, 200 feet AGL, and 100 feet AGL, as well as a "MINIMUMS, MINIMUMS" callout. The flight crew can adjust the "MINIMUMS, MINIMUMS" callout from the EGPWS by setting the radio altimeter to the desired altitude.
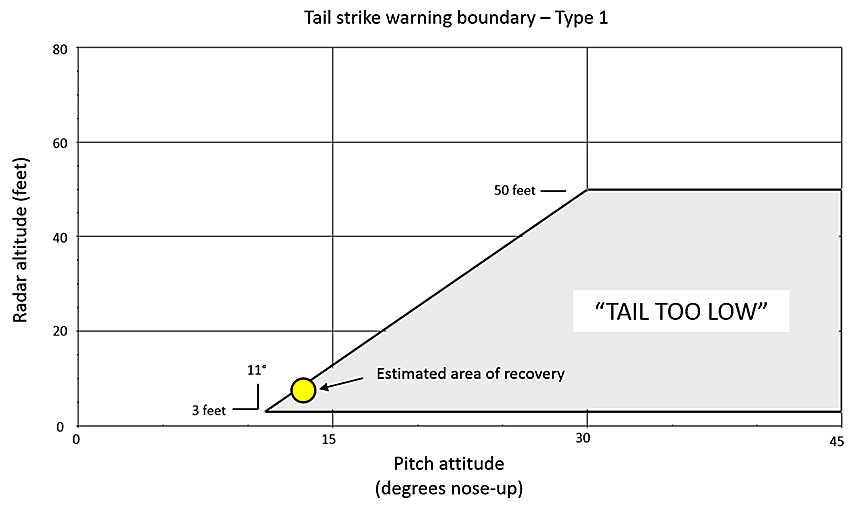
The EGPWS also provides a
tail strike warning function […] for applicable rotary wing aircraft based upon Radio Altitude, Pitch Attitude, Pitch Rate, and Barometric Altitude Rate. The voice message "Tail Too Low" is provided continuously while within the warning boundary. Unique warning boundaries are provided for applicable aircraft types. Footnote 27
The boundary set for the occurrence helicopteris depicted in Figure 7.
There are no emergency procedures or guidance specified in Helijet's standard operating procedures (SOPs) or operations manual for flight crew to deal with EGPWS alerts or warnings.
1.7 Meteorological information
Before the helicopter departed from CYVR, the 0100 aviation routine weather report (METAR) for CYVR was as follows: wind 300° true at 17 knots, visibility 15 statute miles (sm), light rain, few clouds at 1300 feet AGL, broken cloud layer based at 4100 feet AGL, overcast layer of cloud based at 7500 feet AGL, temperature 7°C, dew point 5°C, and altimeter setting 29.54 inches of mercury.
The METAR for CYAZ was available only between 0700 and 1700. The last reported METAR for CYAZ at 1700 on 14 November, the day before the occurrence, was as follows: wind calm, visibility 15 sm, broken cloud layer based at 5000 feet AGL, overcast cloud layer based at 22 000 feet AGL, temperature 6°C, dew point 5°C, and altimeter setting 29.69 inches of mercury. At 0058, the weather conditions reported from CYAZ personnel to the BCEHS dispatcher were a ceiling of 2300 feet and a visibility of 4 sm.
The 0700 reported METAR for CYAZ on 15 November was as follows: wind 010°T at 3 knots, visibility 15 sm, few clouds at 2000 feet AGL, few clouds at 22 000 feet AGL, temperature 2°C, dew point 2°C, and altimeter setting 29.63 inches of mercury.
The closest reporting weather station to CYAZ with 24-hour reporting was Comox Valley Airport (CYQQ), British Columbia, approximately 50 nm north-northeast of CYAZ. The 0200 METAR for CYQQ was as follows: wind 330°T at 12 knots, gusting to 17 knots, visibility 20 sm, overcast cloud layer based at 11 000 feet AGL, temperature 5°C, dew point 1°C, altimeter setting 29.59 inches of mercury.
During the flight, stars were occasionally visible, but there was little or no celestial lighting at the time of the occurrence.
1.8 Aids to navigation
CYAZ is equipped with a non-directional beacon. IFR approaches to Runway 29 include a non-directional beacon non-precision approach and an RNAV non-precision approach. An RNAV approach uses GNSS guidance, and is commonly referred to as a GPS approach.
According to the Canada Air Pilot (CAP), the RNAV Runway 29 approach (Appendix A) depicts a constant descent angle of 3.22°, the optimum descent path for a non-precision final approach segment. An aircraft flying at a ground speed of 110 knots requires a rate of descent of 630 fpm to achieve this descent path. This descent can continue until reaching the minimum descent altitude, which is 580 feet ASL (504 feet AGL) for Runway 29. Pilots on instrument approaches are prohibited from continuing the descent below the minimum descent altitude unless the required visual reference Footnote 28 is established and maintained in order to complete a safe landing.
There was no indication of problems with the available aids to navigation.
1.9 Communications
Radio communications between C-GHHJ and air traffic services were unremarkable throughout the flight, and no issues with communication were identified during the course of the investigation.
1.10 Aerodrome information
1.10.1 General
At the time of the occurrence, CYAZ was certified for day visual flight rules (VFR) operations only. CYAZ has 3 runways:
- Runway 07/25, which is concrete and measures 4999 feet long and 150 feet wide;
- Runway 11/29, which is asphalt and measures 4997 feet long and 100 feet wide; and
- Runway 16/34, which is concrete and measures 5000 feet long and 100 feet wide.
The elevation of CYAZ is 80 feet ASL.
Runway 07/25 runs parallel to the shoreline of Pacific Rim National Park, while Runway 11/29 runs parallel to the Pacific Rim Highway (Number 4) to Tofino. Because CYAZ is a daylight VFR airport only, no runway lights are installed. The surrounding area provides virtually no sources of cultural lighting. The terrain to the north of the airport is dense forest, and the Pacific Ocean is to the south.
The helicopter night landing site at CYAZ was situated on the compass rose at the intersection of Taxiways F, G, and H. There were 12 temporary green Turboflares that the airport operator had set up in a circle. The Helijet TOFLZ landing plate Footnote 29 for CYAZ (Appendix D) correctly indicated this position, but indicated that the lights were amber rather than green. The landing plate also indicated that there was "minimal ambient lighting at the airport and surrounding area" with "no runway lighting." The landing plate does not provide restrictions or cautions to flight crews about overcast conditions or nights without significant moonlight.
1.10.2 Temporary night helipad at Tofino/Long Beach Airport
Medevac helicopter operations were conducted at Tofino General Hospital until December 2011. The helipad at the hospital was then closed after TC determined that the helipad did not meet regulatory standards and was unsafe. Plans were made to temporarily relocate medevac operations to CYAZ, approximately 7 nm southeast of the hospital, until the hospital helipad could be improved and recertified. Because CYAZ was not certified for night operations, Helijet, the British Columbia Ambulance Service, and the airport operator worked with TC to develop an interim solution. Footnote 30
On 09 December 2011, TC inspected CYAZ and met with the airport operator, Helijet, and a local British Columbia Ambulance Service paramedic to discuss night medevac operations involving helicopters at the airport. Following an on-site inspection of the airport, the TC inspector presented the airport and Helijet with a list of actions to be undertaken before night medevac operations could begin. These included the following:
- physical specifications including lighting and a single flight path to conform to Subpart 305 of the Canadian Aviation Regulations (CARs) and CARs Standard 325 (Heliports), as well as TC's TP312;
- obstacle lighting to be installed on the main terminal building, the Tofino Air hangar, and the Quonset hut;
- windsock on south side of Runway 07/25 to be illuminated;
- Helijet to consult with NAV CANADA to arrange to have the automated weather observation system available 24/7 instead of only when air traffic control is operational;
- airport operator to conduct a risk assessment of this additional level of service and receive approval from the CYAZ accountable executive;
- TC to assist CYAZ by issuing a notice to airmen (NOTAM) and a Canada Flight Supplement amendment for night helicopter operations;
- TC to assist CYAZ by issuing a NOTAM advising of unmarked obstacles; and
- airport operations manual to be amended to reflect additional level of service.
Only one of these requirements, the illumination of the windsock, had been implemented before night flights into CYAZ began. Neither the airport operator nor Helijet informed TC that night medevac operations had begun.
At the time of the occurrence flight, the only visible lights at CYAZ would have been the 12 temporary Turboflares set up on the compass rose and an illuminated windsock.
1.11 Flight recorders
Although not required by regulation, the helicopter was equipped with a solid-state Universal CVFDR and a SkyTrac ISAT-100 flight-tracking GPS. These components were removed, analyzed, and found useful to the investigation.
1.11.1 Cockpit voice and flight data recorders
The CVFDR is capable of providing up to "120 minutes of cockpit voice and ambient audio recording, as well as 120 minutes of data link messages [and] at least twenty-five hours of flight data recording." Footnote 31 The occurrence flight had been captured in its entirety.
On 09 October 2012, Sikorsky Helicopter Corporation issued Service Letter CCS-76-AOL-12-0005R1 to all S-76 operators. The purpose of the service letter was to make operators aware of possible erroneous results when interpreting the downloaded FDR data if incorrect conversion factors are applied. The affected values may be those for engine torque and power turbine speed. The letter informed operators that interpretation of the downloaded FDR data required the use of specific conversion factors to achieve accurate results. The company did not provide Maxcraft with the manufacturer's service letter relating to the conversion factors for FDR data, and errors were made when the data was interpreted.
On 16 November 2015, Helijet management reviewed the cockpit voice recorder (CVR) recordings with the occurrence pilots. This is not permitted under the Canadian Transportation Accident Investigation and Safety Board Act (CTAISB Act). The operator was unaware that cockpit voice recordings are privileged under the CTAISB Act.
1.11.2 Satellite tracking ISAT 100
C-GHHJ was equipped with a SkyTrac ISAT 100 Airborne Data/Position Communicator GPS flight-tracking system. This device records flight information such as position, altitude, and ground speed and track in 5-second intervals. This information is automatically transmitted via satellite every 60 seconds.
The SkyTrac ISAT 100 unit was not immediately secured after the occurrence. As a result of the delays in preserving the ISAT 100 data, all of the 5-second flight-information recordings stored internally in the transceiver were overwritten by subsequent flights. On 25 November 2015, the ISAT 100 transceiver was secured and sent to the TSB Engineering Laboratory for data download and analysis. The 60-second position log data allowed the investigation to reconstruct the occurrence helicopter's path.
1.12 Wreckage and impact information
Not applicable.
1.13 Medical and pathological information
Not applicable.
1.14 Fire
There was no fire.
1.15 Survival aspects
Not applicable.
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP267/2015 – CVR Download and Transcript
- LP268/2015 – FDR Download and Analysis
- LP269/2015 – NVM [non-volatile memory] Recovery – ISAT 100
1.17 Organizational and management information
1.17.1 General
Helijet operates under CARs subparts 702, 703, and 704, using a fleet of 19 light and medium helicopters, and 2 light corporate jets. Helijet provides scheduled, chartered, and medevac services across British Columbia. Its bases of operation are located in Richmond, Vancouver, Victoria, Nanaimo, Prince Rupert, and Haida Gwaii. Aircraft are maintained, flown and administered by over 100 employees. Footnote 32
Since 1998, Helijet has been contracted to provide 24/7 air ambulance services for BCEHS using air medical–equipped Sikorsky S-76A and S-76C+ helicopters. Footnote 33
1.17.2 Rotary-wing operations and safety
The Helijet organizational structure is described in Section 2.0 of the Helijet International Inc. Company Operations Manual—Rotary Wing. The accountable executive (AE) designated in Helijet's safety management system (SMS) is the president and chief executive officer. The director of maintenance and the director of flight operations and safety report directly to the AE. At the time of the occurrence, 5 people reported directly to the director of flight operations and safety: the rotary chief pilot, the fixed-wing chief pilot, the flight operations coordinator, a base manager, and a manager of resort operations.
The company organization chart indicated that safety officer(s) report to the director of flight operations and safety. The duties of the safety officer were being fulfilled by the director of flight operations at the time of the occurrence.
The investigation determined that previous safety officers had experienced frustrations while in this role. These included difficulties in closing SMS reports, an inability to implement the proactive safety management processes outlined in the SMS manual, and challenges in carrying out safety-officer duties while flying a full schedule.
The director of flight operations and safety was responsible to the AE "for a systematic, explicit, comprehensive and proactive process for managing safety risks." Footnote 34 The operations manual further outlined 11 specific responsibilities of this position. At the time of the occurrence, the director of flight operations and safety was spending approximately 2 hours per week on safety-specific tasks, mostly related to processing reports received through the SMS reporting process.
The director of maintenance was responsible for ensuring that the helicopters were maintained in accordance with the manufacturer's standards and the regulatory requirements, thereby ensuring that they were airworthy.
After the occurrence flight, although it was known that the helicopter's transmission had been subject to torque values in excess of the maximum limits, the helicopter was returned to flight operations without the required maintenance being carried out on the drive system components.
1.17.3 Company safety management system
Although not required by regulation, Helijet had developed an SMS and had implemented it in 2013.
In its simplest form, an SMS is a documented process for managing risks. A functioning SMS includes but is not limited to Footnote 35:
- a process for setting goals for the improvement of aviation safety and for measuring the accomplishment of those goals;
- a process for identifying hazards to aviation safety and for evaluating and managing the associated risks;
- a process for ensuring employees are trained and competent to perform their duties;
- a process for the internal reporting and analyzing of hazards, incidents and accidents and for taking corrective actions to prevent their recurrence;
- a document containing all the safety management processes and a process for making employees aware of their responsibilities; and
- a quality assurance process for conducting periodic reviews or audits of the SMS.
A formal SMS may contain multiple mechanisms to improve safety. Some may support proactive safety management, such as initial risk assessments, and others may support reactive safety management, such as reporting mechanisms.
For an SMS to be effective, it must be supported by a safety culture that provides the commitment, competence, and cognizance Footnote 36 to develop and maintain safety management activities. The organization should be motivated to continually improve safety and to reduce risk. Appropriate resources must be allocated to these functions. It requires a technical competence to achieve its safety goals and to gather and analyze safety information. The organization needs to be aware of the requirement to be constantly vigilant against emerging hazards and the need to review current safety management mechanisms if they are not working as intended.
Helijet's SMS manual states that
It is the Company's continued objective to mitigate injury to all people employed and/or conducting business with Helijet; eliminate damage to equipment and property and to prevent all accidents – by developing work processes that will identify, reduce and ultimately eliminate safety incidents and hazards. Footnote 37
The SMS manual described a number of safety management processes, including reporting and risk assessment processes.
1.17.3.1 Safety reporting system
Effective safety management requires an organization to have the processes and mechanisms in place to identify and respond to significant safety events. This goal can be achieved through processes such as reporting tools, safety assurance processes, and reactive risk assessments. With such mechanisms, safety issues encountered during day-to-day operations are freely reported, addressed, tracked, and fed back to the individual who reported it. Information recorded may also be used to track safety trends in order to identify emerging safety issues.
Helijet's SMS included a process for collecting and disseminating information on incidents, accidents, occurrences, and hazards. The SMS manual laid out the process for entering and processing reports through the system, established the expectation that all employees would participate in the reporting process, and stated that the reporting system was non-punitive:
Helijet recognizes that a successful reporting system is based on an employee not being subject to retribution or penalty for reporting a safety concern. The exception would be for flagrant disregard for existing rules and regulations or wilful misconduct. Footnote 38
Information gathered during the investigation revealed that the SMS reporting process was being used to some extent, with an estimated 70 reports being received annually. However, instances were also identified where hazards or safety concerns were not reported through the reporting process. For example, approximately 1 month before the occurrence, a Helijet air ambulance pilot had recognized that CYAZ was a difficult place at which to land at night due to its lack of cultural lighting. This hazard was discussed with the airfield manager, and more Turboflares were added in a line along the taxiway extending from the compass rose. This provided additional visual cues to facilitate the departure of the helicopter and the arrival of the helicopter that was scheduled to come in later that evening. The identification of this hazard was not discussed with Helijet management or entered in the SMS reporting system.
1.17.3.2 Risk management
Effective safety management requires an organization to identify potential hazards and mitigate the potential risks to a level that is as low as reasonably practicable. This may be achieved through proactive risk management processes and practices, such as risk assessments of a new operating environment with the aim of introducing controls before commencing operations.
At the time of the occurrence, Helijet's SMS manual provided a list of generally accepted triggers for a risk assessment to be conducted. These included:
- Commencement of new operations or routes;
- Commencement of new activity; and
- Commencement of an existing activity in a new environment.
The SMS manual further specified the following:
Usually a Risk Assessment would be conducted before an activity takes place. The applicable Manager should consult with the Safety Department to determine the applicability of a Risk Assessment and establish who should be involved and establish a practical time line. Footnote 39
The SMS manual provided a process for conducting risk assessments and a format for documenting them based on guidance material provided by TC. The SMS manual did not provide practical advice with respect to who would conduct risk assessments or where the applicable forms could be accessed. At the time of this occurrence, the manual also did not define how the results of risk assessments were tracked.
Few risk assessments were completed after Helijet implemented its SMS in 2013. The director of safety was also the director of flight operations; this meant that safety-related monitoring activities were often not accomplished due to flight operations demands. A quality assurance manager had been appointed, but this role had not yet been established in flight operations.
Prior to the CYAZ occurrence, 4 temporary night helipad locations at airports were being used by Helijet for night medevac operations. When Helijet implemented its SMS program, no risk assessments were conducted on existing helipads, and this activity was not monitored as part of the SMS.
1.17.3.3 Safety management systems and regulatory oversight
Currently, in Canada, only large commercial carriers operating under Subpart 705 of the CARs Footnote 40 are required to have an SMS. While many smaller companies have recognized the benefits of SMSs and voluntarily begun implementing them within their organizations, approximately 90% of all Canadian aviation certificate holders are still not required by regulation to have an SMS. In TSB Aviation Investigation Report A13H0001, the Board concluded that under the current oversight model, TC cannot ascertain whether these operators are able to manage safety effectively.
As a result, the Board has recommended that
the Department of Transport require all commercial aviation operators in Canada to implement a formal safety management system.
Transportation Safety Recommendation A16-12
and that
the Department of Transport conduct regular SMS assessments to evaluate the capability of operators to effectively manage safety.
Transportation Safety Recommendation A16-13
To ensure that companies use their SMS effectively, and to ensure that companies continue operating in compliance with regulations, the Board also recommended that
the Department of Transport enhance its oversight policies, procedures and training to ensure the frequency and focus of surveillance, as well as post-surveillance oversight activities, including enforcement, are commensurate with the capability of the operator to effectively manage risk.
Transportation Safety Recommendation A16-14
TC has agreed in principle with all of these recommendations and has responded that it will continue to promote voluntary adoption of SMS while carrying out reviews of the existing regulations and surveillance processes. Pending the outcomes of these reviews, all 3 recommendations remain active and have been assessed as Unable to Assess, Satisfactory in Part, and Satisfactory Intent, respectively.
1.18 Additional information
1.18.1 Human performance
1.18.1.1 Mental models and building situational awareness
Situational awareness is defined as "the perception of the elements in the environment within a volume of time and space, the comprehension of their meaning and the projection of their status in the near future." Footnote 41
This definition outlines the 3 commonly accepted stages of situational awareness. Effective performance in dynamic environments relies on the individual's ability to take in information (level 1) and understand its meaning (level 2) and its implications for the future of the operation (level 3).
Developing situational awareness is not a passive process, but one in which both individuals and teams play an active role. In dynamic operational environments, individuals are actively involved in selecting the information that requires their attention and interacting with other team members to confirm their understanding of situations. Footnote 42
A mental model is an internal representation of a system and the operating environment that is developed through experience. An accurate mental model makes it easier for an individual to develop situational awareness at all stages by guiding their attention and allowing them to more quickly understand the meaning of the situation and project future states. An inaccurate mental model, however, may increase the likelihood that important information will not be attended to, or that its significance will not be recognized. This can occur if a crew, or a crew member, reverts to a default mental model when an unexpected situation is encountered. Footnote 43 Preparation and crew coordination play a critical role in ensuring that accurate mental models are developed that support situational awareness:
Expectations may be formulated based on the active mental model and prior expectations. They also may be developed through instructions or other communications. Pilots, for example, frequently develop strong expectations based on the pre-flight briefing. These expectations can provide a very efficient mechanism for filtering the data in the environment to a subset that is expected to be useful. Footnote 44
1.18.1.2 Crew resource management and authority gradient
CRM involves providing crews with the skills and tools necessary to optimize leadership, team formation, problem solving, decision making, and situational awareness. Footnote 45 Operators can support effective CRM by providing crews with CRM training and SOPs that encourage the sharing of information and confirming understanding. Procedures that support the development and maintenance of a shared mental model include cross-checks, standard calls, and briefings that focus on the risks associated with a specific flight while encouraging 2-way communication.
As a leader, the captain plays a critical role in establishing the tone for a flight. Effective captains strike an appropriate balance between exerting a level of authority that provides for expedient decision making and opportunities for open communication. In contrast, less effective captains may be more autocratic, shutting down input from the crew or abdicating responsibility. In doing so, they do not effectively control activities on the flight deck. Footnote 46
The balance of authority and interaction in the cockpit has been referred to as the cockpit authority gradient. In addition to assuming ultimate responsibility for the safety of a flight, a pilot who has assumed the role of captain typically has more authority over the person who has assumed the role of the first officer by virtue of their qualifications and experience. An equal level of authority between crew members can result in excessive professional courtesy and ineffective communications or cross-checking.
Pre-flight briefings provide an important opportunity to establish good teamwork and communication, and should address the team dynamic, as well as the technical issues anticipated for a flight. Footnote 47
1.18.2 Standard operating procedures for air ambulance operations
1.18.2.1 General
Commercial operators of aircraft that are to be flown by 2 or more pilots are to
establish and maintain standard operating procedures that enable the crew members to operate the aircraft within the limitations specified in the aircraft flight manual and that meet the Commercial Air Service Standards. Footnote 48
Helijet had established SOPs for the operation of the S-76C+ for air ambulance operations that met the requirements of CARs subsection 703.107(1).
The SOPs are divided into 9 sections: General, Before Flight, Departure, Cruise, Arrival, After Flight, Abnormal and Emergency Procedures, Noise, and Ambulance Service. The latest revision to Helijet Standard Operating Procedures: Air Ambulance Sikorsky 76C+ was effective 14 October 2014. During a program validation inspection by TC inspectors on 28 November 2014, Helijet's SOPs were reviewed and found to meet the requirements of CARs subsection 703.107(1).
1.18.2.2 Designation of pilot-in-command
Crews are scheduled for day or night shifts to allow the company to provide 24-hour operational services. Because of scheduling and contractual requirements, 2 captain-qualified pilots were commonly paired together during medevac flights.
According to the company's SOPs:
Unless otherwise specifically assigned by the Chief Pilot, the PIC [pilot-in-command], who is the pilot-in-command for all flights by that crew, will be the pilot whose name appears highest on the latest pilot list as published by the Chief Pilot for this purpose. Footnote 49
It was also company policy that, if one of the crew members was a training captain, this pilot should automatically assume the role of PIC, regardless of the training captain's position on the pilot list. At the time of the occurrence, this information was not included in the company SOPs or on the crew schedule, and the crew were unaware of the policy.
For the occurrence flight, as was typical, 2 captain-qualified pilots were paired together as a captain and a first officer. The on-duty pilot had been with the company the longest, had more hours on type, and was higher up on the pilot list, and therefore assumed the role of captain/PIC. The other captain, despite being a training captain, took the role of first officer. Determining which pilot took the role of PM and which took the role of PF was at the PIC's discretion. The crew agreed that the PIC would be the PM.
Both captains were aware of each other's experience. The PIC knew that the other captain was a training captain and had previously been the assistant chief pilot. The training captain knew that the PIC had much more experience with the company and with the S-76.
According to the SOPs, "whenever the aircraft is crewed by two pilots the crew coordination procedures in [the SOPs] shall be followed". Footnote 50
1.18.2.3 Pilot flying and pilot monitoring
1.18.2.3.1 Duties of the pilot flying
The PF is responsible for manoeuvring the helicopter throughout the flight. When the helicopter is under the control of the autopilot, the PF should continually monitor the flight path and make corrections accordingly. The PF duties are detailed in the company's air ambulance SOPs:
The PF's prime duty is to control the aircraft. The PF must keep the wellbeing and comfort of the passengers uppermost in mind when maneuvering the aircraft. Extreme maneuvers are forbidden. Where possible, angles of bank greater than 20 degrees are to be avoided. […] Rates of climb exceeding 1500 fpm or descent exceeding 1000 fpm, except where absolutely operationally necessary, are to be avoided. […] During any abnormal or emergency situation the PF is to give full attention to the flight path and control of the aircraft until the situation is under control. Footnote 51
Specific PF duties are discussed throughout the SOPs. Standard calls are included to "reduce the likelihood of an incorrect interpretation of a request or command and to initiate corrective action for undesirable situations". Footnote 52 When an abnormal rate of descent or abnormal rate of speed is observed, the PM should call "descent rate" or "speed." The PF should respond with "check, correcting" and correct the rate of descent or airspeed to within the normal parameters.
1.18.2.3.2 Duties of the pilot monitoring
The PM normally monitors the aircraft and systems, calls out any perceived or potential deviations from the intended flight path, and intervenes as necessary.
According to the company's SOPs,
The PM's prime duty is to monitor the aircraft and the actions of the PF.
The PM is to:
- Read the checklists.
- Monitor engine and all flight instruments (PM and PF) for unusual indications.
- Provide information to the PF on request.
- Manage flight navigation systems […].
- […] monitor the flight's progress to ensure that the clearances are being complied with.
- Keep a visual lookout for traffic
During any abnormal or emergency situation it is the PM's duty to analyze the problem, communicate the findings to the PF, consult the Emergency Procedures Manual and carry out the proper corrective actions as required. The PM should also be prepared to assist the PF in controlling the aircraft as necessary. Footnote 53
The company air ambulance SOPs specify that "the PM is to monitor the rate of descent. Call if over 750 FPM" and "call torques at 50% and every 10% above 50%; and N1 if limits are approached." Footnote 54
With regard to aircraft control and the assumption of control, the SOPs state the following:
It is essential that during all phases of ground and flight operation, both pilots clearly understand which pilot has control and is therefore the Pilot Flying (PF). […] the PIC shall specifically advise the flight crew of who is the PF. Whenever control is passed from one pilot to the other, the pilot relinquishing control must provide the pilot assuming control with any relevant aircraft performance information. […]
The PIC may assume control at any time. When advised that the PIC is assuming control the FO shall relinquish control immediately. Notwithstanding the previous, the FO shall assume control when necessary to protect the safety of the aircraft. It may be necessary for the FO to take control to avoid collision where there is inadequate time to properly communicate the requirement to the PIC due to pilot incapacitation. Footnote 55
In this occurrence, the PM took control of the helicopter approximately 40 seconds after the steep rate of descent, at which point the helicopter was approximately 3 feet AGL. The PM did not state that control was being transferred.
1.18.2.4 Pre-flight planning and briefing
The company's air ambulance SOPs define the flight crew duties and responsibilities before flight. Items that need to be taken into consideration include weather, routes, heliport and airport serviceability, duty time, helicopter equipment and serviceability, crew experience, ability and familiarity with the route, and landing location.
Before every flight each pilot shall brief the other on information about the flight that is relevant to their duties. […] As a minimum both pilots should know the following information:
- weather for departure, en route, destination, and (if applicable) alternate destination. […];
- fuel load;
- payload;
- flight time, route to be flown, and any work to be carried out;
- any duties in addition to those specified in these SOPs and other directives.
It is the PIC's responsibility to ensure that the required information is obtained and a proper briefing is carried out. Footnote 56
It was company practice for the crew members to plan for and brief the intended flight and flight plan. The briefing was to include a reference to the landing plates for the expected destination and a discussion of both the runway expected for landing and the expected visual references. The investigation determined that dispatch time constraints for departures often prevented medevac flight crews from conducting thorough pre-flight briefings. One of the primary purposes of planning and briefing is to establish a correct shared understanding of the route and destination.
Before the occurrence flight, the crew did not discuss the Helijet TOFLZ landing plate, nor did they discuss their individual experience with landing at CYAZ. The crew did not perform any pre-flight risk assessment concerning night flying, IFR, or visual cues. By takeoff, the crew had not established a correct shared understanding of the landing site, nor did they have a shared understanding that this would be both pilots' first approach to CYAZ at night.
1.18.2.5 Flight director and navigation systems
A coupled autopilot, when used correctly, can reduce flight crew workload and fatigue, and can increase the accuracy of the intended flight. For an NVFR approach, the SOPs stipulate, "No coupled flight in the visual circuit or near other traffic in the airport vicinity. No coupled flight below 1000 feet […]. Decouple before final approach checks or sooner." Footnote 57
1.18.2.6 Minimum airspeed
Although the SOPs do not have a minimum airspeed for an NVFR approach, the SOPs reiterate that the minimum airspeed in instrument meteorological conditions (VMINI) is 60 knots, as per the rotorcraft flight manual. Footnote 58 The SOPs also discuss that VMINI is below the best rate of climb speed (VBROC) and state the following:
Any reduction in airspeed results in an increase in power required. There may not be enough power to maintain level flight whilst accelerating back to the required speed. In addition the aircraft has a tendency to decelerate quite quickly when below Vbroc. Because of the power requirements, and difficulty with directional control in IMC at low airspeed, the aircraft will not be operated by this company in IMC at airspeeds of less than Vbroc, unless conducting a fully coupled autopilot approach. Footnote 59
1.18.2.7 En route
The EVS screen is designed to provide the crew with improved visual references. Both crew positions are provided with an EVS. The PM referred to his EVS throughout the flight. The PF, however, turned down the EVS because the display appeared too bright. The PF was flying without additional visual references from the EVS.
It was company practice to fly the intended and filed flight plan. If an unexpected situation arose in flight that required the nature of the flight to be changed, such as reverting to an IFR plan due to unexpected instrument meteorological conditions, the practice was to brief this change or to terminate the flight, return to base, make a new plan, and brief a separate flight plan.
The crew had planned for and filed an NVFR flight plan, which would have given them an approach across the ocean on a 358° heading onto Taxiway H. This would have been a direct approach to the temporary night helipad, as detailed in the landing plate (Appendix D). Contrary to the original flight plan, at 0222, the PM loaded into the GPS an IFR approach to Runway 29.
1.18.2.8 Arrival
1.18.2.8.1 Instrument flight rules check
The purpose of the IFR check is to prepare the flight crew for an IFR arrival. According to the SOPs, the IFR check is "not to be carried out when operating VFR." Footnote 60 The crew did not perform an IFR check or instrument approach briefing. The crew did not ascertain whether they still shared the same correct understanding of the route and destination.
TC's Multicrew Aircraft Standard Operating Procedures state:
Prior to each approach and landing, the flight crew shall be briefed on the critical aspects of the procedure. The approach should be briefed by the pilot who will fly the procedure. […] During the actual approach, the flight crew is to compare the procedure as it is flown to […] what was briefed. Should a deviation become apparent to the PNF [pilot not flying] or crew other than the PF, it shall be brought to the attention of the PF. The PF shall either correct the deviation or, if appropriate, indicate that the deviation is intentional and state the revised parameters or procedure. If it is appropriate to deviate from the briefed procedure, the PF shall advise the remaining flight crew members of the change. Footnote 61
The instrument approach briefing allows the PF to discuss how they intend to conduct the approach. The main points of the briefing are highlighted to ensure that both crew members understand and agree that the procedures are being interpreted correctly and to allow any errors or omissions to be corrected.
On an IFR approach, IFR checks are the first formal opportunity for the crew to determine whether they still share the same correct understanding of the route and destination, as established in the initial plan and brief.
A commonly used format for the instrument approach briefing is the AMORTES format:
- Approach: state the name of the approach, type of approach to be flown, and the Canada Air Pilot page number and effective date.
- Minima: state the minimum altitudes with applicable altimeter setting, procedure turn altitude, final approach fix crossing altitude, decision height, decision altitude, minimum descent altitude, and the radio altimeter alert warning settings.
- Overshoot: state the missed approach procedure to be flown.
- Radios: set up the navigation radio.
- Timing: state the time inbound and speeds to be flown.
- Emergencies: state the procedures for dealing with an emergency.
- Switches: both PF and PM set all navigation and horizontal situation indicator switches.
When flying an IFR approach, it is standard operating practice for company pilots to perform an IFR check and an instrument approach briefing:
At a point no less than 10 NM from the destination, prior to the beginning of the initial descent, an approach briefing, in the "AMORTES" format shall be given […]. Footnote 62
1.18.2.8.2 Initial approach check
On both VFR and IFR approaches, the TC Multicrew Aircraft Standard Operating Procedures require an approach briefing to be performed. It is standard operating practice for company pilots to complete an initial approach check early enough to "reduce the workload closer to the landing". Footnote 63 Part of the initial approach check is the landing briefing, which is intended to prepare the aircraft and the crew for landing at the intended landing site. The landing briefing should be given by the PF and "should outline the visual landing including the direction of the approach, touchdown point and taxi intentions". Footnote 64 The initial approach checks are the second (if flying an IFR approach) or first (if flying a VFR approach) formal opportunity for the crew to ascertain if they still share the same correct understanding of the route and destination, as established in the initial plan and brief.
At 0224:45, the PF called for the initial approach checks. At 0224:57, the PM called for the landing briefing. The PF responded that they were going to land on whatever runway they saw in front of them. The PF did not discuss the position of the landing site in relation to the approach or the temporary Turboflares on the compass rose, nor did the PF brief a missed approach or the probable airfield visual cues and terrain. At 0230:23, the PF stated that the PF had not landed at CYAZ within the past 6 months.
According to the company SOPs, "if a pilot has a doubt about a clearance, procedure, or situation, they must make that doubt known to the other pilot." Footnote 65 Standard calls are included to "reduce the likelihood of an incorrect interpretation of a request or command to initiate corrective action for undesirable situations." Footnote 66
1.18.2.8.3 Final approach checks
For both VFR and IFR approaches, the company SOPs state that the "Final Approach Check should be called for by the PF at the FAF [final approach fix] or when the aircraft is below 110 KIAS". Footnote 67 The final approach check typically includes a visual assessment of the landing site and surrounding area and configuration of the helicopter for landing. The final approach checks are the third (if flying an IFR approach) or second (if flying a VFR approach) formal opportunity for the crew to ascertain if they still share the same correct understanding of the destination.
At 0233:31 the PF called for the final approach checks, which the PM completed. At 0234:32, while the helicopter was descending, the PF commented that it seemed a little bit hazy and it felt like they were descending into fog. Despite the haze, the PF identified a bright light in the vicinity of the airport but could not envision the approach path in relation to the landing site.
The PM confirmed that they were headed to the area around the threshold of Runway 29 and then confirmed that parking would be to the right of the PF. The PF continued to question the location of the landing site.
1.18.2.9 Stabilized approach
The Helijet air ambulance SOPs do not describe a stabilized approach procedure specific to an NVFR approach, but they do describe the stabilized approach for IFR operations:
Final approach can be a very high workload period of flight and potentially one of the most hazardous phases of flight. A Stabilized Approach is intended to decrease workload, minimize crew distraction, and reduce the hazards associated with configuration changes at a critical phase of flight; generally it improves the likelihood of a successful approach. The Stabilized Approach configuration should be achieved no later than crossing the FAF/FAWP [final approach fix / final approach waypoint] […] If a stabilized approach is not achieved crossing the FAF/FAWP […] consideration should be given to executing a missed approach. Similarly, if one or more components of a previously stabilized approach are exceeded, consideration should be given to commencing a missed approach. Footnote 68
Two conditions that should prompt flight crews to consider a missed approach are a rate of descent greater than 1000 fpm and an airspeed deviation higher or lower than 10 knots from the briefed approach speed.
1.18.2.10 Missed approaches
During approaches, it may become inadvisable to continue to land. Reasons for discontinuing the approach may be but are not limited to:
- too high or too low of an airspeed;
- too high of a rate of descent;
- the required visual reference has not been established;
- the helicopter is not in a position to land within the intended landing area; and
- a flight crew member is not comfortable with the approach sequence, or an emergency or abnormal situation develops during the approach.
1.18.3 Night flying
1.18.3.1 Night visual flight rules
The principle behind VFR flight is that the pilot takes attitude reference from visual cues outside of the aircraft. Some basic requirements must therefore be met when conducting VFR flight, whether day or night. In Canada, under CARs sections 602.114 and 602.115, regardless of whether it is operated in controlled or uncontrolled airspace, the aircraft must be "operated with visual reference to the surface." Footnote 69 The CARs define "surface" as "any ground or water, including the frozen surface thereof". Footnote 70 Therefore, using TC's interpretation of the NVFR requirements, a flight conducted over an area away from cultural lighting and where there is inadequate ambient light to clearly discern a horizon (i.e., to continue flight solely by reference to the surface) does not meet the requirements for operation under VFR. Instead, the flight would be conducted by IFR, which requires pilots to rely on their flight instruments to ensure safe operation of the aircraft.
NVFR is permitted in several other countries. However, the night flying regulations in some countries differ significantly from those of the CARs. In Ireland, for example, NVFR flights are not authorized unless they are conducted within a control zone, at which point they will be operated as special VFR flights. Footnote 71 Night flights conducted outside a control zone must be conducted in accordance with IFR regulations. In the United States, the Federal Aviation Regulations specify that no person shall operate a helicopter under VFR at night unless that person has "visual surface light reference, sufficient to safely control the helicopter." Footnote 72
Currently, there is no requirement for Canadian commercial air operators to demonstrate that they will be able to maintain visual reference to the surface along a proposed NVFR route, either through cultural lighting or alternative means. One exception, however, is a special provision in CARs paragraph 702.18(3)(c) that permits single-engine VFR flights at night where the pilot does not hold an instrument rating. According to the Commercial Air Service Standards, the area overflown must be "illuminated by lights on the surface to ensure visual surface reference and conditions provide for a discernible horizon." Footnote 73
TSB Aviation Investigation Report A13H0001 identified that, without clearly defined NVFR requirements that establish unaided visual reference/lighting considerations or alternative means of maintaining visual reference to the surface (i.e., night-vision imaging systems), it is highly likely that accidents such as this one will continue to occur.
Therefore, the Board recommended that
the Department of Transport amend the regulations to clearly define the visual references (including lighting considerations and/or alternate means) required to reduce the risks associated with night visual flight rules flight.
Transportation Safety Recommendation A16-08
TC has indicated that one of the expectations for NVFR is that there be a discernible horizon. However, in remote areas or areas with little or no cultural lighting, NVFR flights are frequently conducted in conditions where there is no discernible horizon, and TC allows those operations to continue.
Industry operators and crews have generally come to interpret NVFR as meaning that a flight is operated adhering to VFR weather requirements and, in the absence of visual cues, is conducted using instrument-flying skills and procedures. TC itself approves NVFR routes in areas with little or no cultural lighting, and there is no requirement for operators to demonstrate that visual reference can be maintained along such routes.
The reported weather for the occurrence flight was a 2300-foot overcast ceiling with 4 sm of visibility; the captain accepted the flight. However, with a mid-level overcast ceiling and very limited to no cultural lighting, it is unlikely that the crew would have been able to discern a horizon or maintain visual reference to the surface after flying beyond the east shore of Vancouver Island en route to CYAZ.
Helijet's SOPs do not include a detailed section that addresses the hazards involved with night flying, nor do they outline precautions to take when flying night VFR approaches to ensure that a level of safety is maintained.
1.18.3.2 Black-hole effect
The black-hole effect is an inherent risk of night visual approaches. It is a visual sensory illusion that leads pilots to believe that they are approaching at a higher altitude than they actually are. Visual approaches at night require the flight crew to maintain an instrument scan with good cockpit resource management skills and communication.
According to the Flight Safety Foundation, "The black-hole effect typically occurs […] over water or over dark, featureless terrain where the only visual stimuli are lights located on and/or near the airport" Footnote 74 or landing zone. The absence of visual references in a pilot's near vision affects depth perception and can lead to a sensation of being too high on approach. In many cases, pilots will react to these false sensations by correcting altitude to below the correct flight path.
According to a study by the U.S. Air Force entitled "Visual Spatial Disorientation: Revisiting the Black Hole Illusion," Footnote 75 spatial disorientation is defined by Gillingham as "an erroneous sense of one's position and motion relative to the plane of the earth's surface." Footnote 76 The study also states:
Visual spatial disorientation (SD) is cited often as a contributor to aviation accidents. The black hole illusion (BHI), a specific type of featureless terrain illusion, is a leading type of visual SD experienced by pilots. A BHI environment refers not to the landing runway but the environment surrounding the runway and the lack of ecological cues for a pilot to proceed visually. The problem is that pilots, despite the lack of visual cues, confidently proceed with a visual approach. The featureless landing environment may induce a pilot into feeling steep (above the correct glide path) and over-estimate their perceived angle of descent (PAD) to the runway. Consequently, a pilot may initiate an unnecessary and aggressive descent resulting in an approach angle far too shallow (below the correct glide path to landing) to guarantee obstacle clearance. Footnote 77
Although not required by regulation, some operators designate appropriate landing areas as black holes, and integrate specialized training and procedures, including SOPs specific to black holes, into their operations. Helijet's SOPs and training program did not address black holes, and the operator had not identified any of its planned destinations as black-hole approaches.
1.18.3.3 Night-vision goggles
Night-vision goggles (NVGs) were first introduced in aviation by the U.S. Army in the 1970s. "The enhanced effectiveness of nighttime flight operations afforded by the use of NVGs created a demand for these devices by civil operators, who have round-the-clock flight requirements." Footnote 78
"The basic operating principle of NVGs is to receive and intensify ambient light and then present an image to the human eye." Footnote 79 Their use "can increase safety, enhance situational awareness, and reduce the pilot workload and stress that are typically associated with night operations." Footnote 80
Many helicopter emergency medical services (HEMS) operators, police forces, civilian search-and-rescue (SAR) organizations, and forestry and wildlife agencies have adopted NVGs for their night operations. Footnote 81 According to the Flight Safety Foundation, NVG use among civilian HEMS providers in the United States has grown from between approximately 2% and 5% in 2006 to more than 90%. Footnote 82 A large HEMS provider based in Western Canada has been flying with NVGs at night since the mid-2000s. NVGs are used by the Royal Canadian Mounted Police rotary-wing division, and by other provincial and municipal police and government agencies. Recently, a large Canadian offshore helicopter operator also began using NVGs for its night SAR operations. TC expects the use of night vision imaging systems to continue to rise, given the increased safety margins that they provide during NVFR operations. Footnote 83
Although there are some challenges associated with NVG operations, it is widely accepted that NVGs significantly reduce the risks associated with NVFR operations—particularly the risk of controlled flight into terrain.
At the time of the occurrence, the company was not using NVGs, nor was it required to do so.
1.18.4 Vortex ring state
Vortex ring state (VRS) is an aerodynamic phenomenon that occurs when a helicopter's flight path, airspeed, and rate of descent coincide with the helicopter's downwash. A helicopter in VRS quickly begins losing altitude, despite having power available to sustain flight. The investigation concluded that VRS was not a factor in this occurrence.
1.18.5 TSB Watchlist
The Watchlist identifies the key safety issues that need to be addressed to make Canada's transportation system even safer.
1.18.5.1 Safety management and oversight is a Watchlist 2016 issue
Safety management and oversight will remain on the TSB Watchlist until
- Transport Canada implements regulations requiring all commercial operators in the air and marine industries to have formal safety management processes and effectively oversees these processes;
- transportation companies that do have SMS demonstrate that it is working—that hazards are being identified and effective risk-mitigation measures are being implemented; and
- Transport Canada not only intervenes when companies are unable to manage safety effectively, but does so in a way that succeeds in changing unsafe operating practices.
At the time of the occurrence, Helijet's SMS was not yet fully developed, and it had not been assessed by TC. The issue of regulatory oversight of air operators, as raised in several previous TSB investigations, highlights the need for a clear regulatory framework requiring all companies to implement an SMS appropriate to the scope and size of its operations; a requirement to demonstrate that SMS that are effective in identifying hazards and mitigating risks since TSB investigations in all modes have identified instances in which safety management processes were weak or not used; and a balanced approach to regulatory oversight that allows the regulator to provide oversight of a company's safety management processes and intervene when necessary to address safety issues.
1.18.5.2 Unstable approaches are a Watchlist 2016 issue
Unstable approaches will remain on the TSB Watchlist until
- major airlines track stable approach–policy compliance through their safety management systems, and take action to reduce the number of unstable approaches that are continued to landing; and
- there is a reduction in the number of incidents of unstable approach and in the number of accidents in which approach stability was a causal or contributing factor.
As this occurrence demonstrates, unstable approaches and accidents in which approach stability was a causal or contributing factor remain an issue of concern.
In March 2014, the Board issued Recommendation A14-01 to Transport Canada requiring CARs Subpart 705 operators to monitor and reduce the incidence of unstable approaches that continue to a landing.
One of the responses to Recommendation A14-01 was TC's development of the Civil Aviation Safety Alert (CASA) to communicate with air operators operating under Subpart 705. In June 2014, CASA 2014-03 was published; it raised concern that Subpart 703 and 704 operators may also be affected by unstable approaches and encouraged them to address such approaches voluntarily.
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
There was no indication that a helicopter component or system malfunction contributed to this occurrence. The flight crew were certified and qualified in accordance with existing regulations. In this occurrence, the crew were not operationally ready for the conditions they encountered during the approach and landing at Tofino/Long Beach (CYAZ). Additionally, CYAZ did not meet the criteria for night operations, and had not been approved by Transport Canada (TC) for night operations. This analysis will focus on helicopter control, night flying, crew preparation and coordination, standard operating procedures (SOPs), safety management, and the helicopter's return to service.
2.1 Helicopter control
As the helicopter approached CYAZ, the crew decided to deviate from the night visual flight rules (NVFR) route and conduct a practice instrument flight rules (IFR) approach to maintain a safe profile above terrain and obstacles during the approach to the airport, as well as to maintain proficiency on an IFR approach. As the helicopter passed waypoint AT2, the flight crew loaded and activated the global positioning system (GPS) area navigation (RNAV) global navigation satellite system Runway 29 approach for CYAZ (Appendix A).
On several occasions during the flight, while discussing the approach, the crew referred to "the runway" at CYAZ, and the expectation of the pilot flying (PF) was to conduct an approach to a runway environment, rather than to the temporary night helipad.
The aerodrome at CYAZ was unlit, with the exception of an illuminated windsock and a ring of Turboflares on the compass rose that defined the temporary night helipad. At no time before or during the approach did the crew discuss the absence of aerodrome lighting at CYAZ.
Approximately 10 seconds after the autopilot was decoupled, the helicopter speed decreased below 60 knots indicated airspeed (approximately VMINI), and the pitch attitude increased to beyond 14° nose-up. Once the PF recognized how close they were to the intended landing zone and determined that the landing zone was not a runway environment, the PF attempted to adjust the approach by reducing collective input to minimum power and increasing the pitch attitude to slow the helicopter further.
The helicopter descended at rates exceeding 2600 feet per minute (fpm), with airspeed transitioning through 0 knots forward and entering rearward values. During the recovery attempt, the helicopter experienced a severe reduction in main rotor rotations per minute (rpm) (NR) and a loss of directional control. When the PF realized that the location of the landing zone was closer than expected, the large control inputs made to adjust the descent angle and speed resulted in a hazardous approach profile.
During the approach, both crew members were occupied with maintaining visual reference to the landing zone, and the hazardous approach profile went unrecognized.
While a visual approach was being conducted to a temporary night helipad at an unlit aerodrome at night, positive control of the helicopter was lost.
2.2 Night flying
2.2.1 Definition of night visual flight rules in Canada
Flights under visual flight rules (VFR) regulations must adhere to 2 principles—navigation with visual reference to the surface, and the "see-and-avoid" concept of traffic separation—regardless of whether the flight is conducted in daylight or darkness. Sections 602.114 and 602.115 of the Canadian Aviation Regulations (CARs) stipulate that all NVFR flights, whether conducted in controlled or uncontrolled airspace, must be "operated with visual reference to the surface." Footnote 84
NVFR regulations vary around the world. In some countries, NVFR is prohibited and night flights outside of control zones are required to be conducted under IFR. In other countries, NVFR is heavily restricted in terms of where the flight can be conducted. In the U.S., for example, NVFR regulations for helicopters require that there be sufficient light to safely control the aircraft. In Canada, the general NVFR regulations contain no such requirement.
What "visual reference to the surface" means is open to interpretation, because the concept is not defined in regulations. TC has indicated that one of the expectations for NVFR is that there be a discernible horizon. However, in remote areas or areas with little or no cultural lighting, NVFR flights are frequently conducted in conditions where no discernible horizon is present and where visual reference to the surface is not possible.
Industry operators and crews have generally come to interpret NVFR to mean that a flight is operated adhering to VFR weather requirements and, in the absence of visual cues, is conducted using instrument-flying skills and procedures. It was apparent during this investigation and other investigations that many pilots, including those at Helijet International Inc. (Helijet), believe that operating flights in this manner is permitted by the regulations. TC itself approves NVFR routes in areas with little or no cultural lighting, and there is no requirement for operators to demonstrate that visual reference can be maintained along such routes.
Canada does not have clearly defined NVFR requirements that establish unaided visual reference and/or lighting considerations, or alternative means of maintaining visual reference to the surface (i.e., night-vision imaging systems). Therefore, in TSB Aviation Investigation Report A13H0001, the Board recommended that
the Department of Transport amend the regulations to clearly define the visual references (including lighting considerations and/or alternate means) required to reduce the risks associated with night visual flight rules flight.
Transportation Safety Recommendation A16-08
CARs section 602.115 does not define "visual reference to the surface," which has been widely interpreted by the industry to mean "visual meteorological conditions." As a result, night flights may be conducted with inadequate visual references, increasing the risk of controlled-flight-into-terrain and loss-of-control accidents.
While the CARs provision for NVFR flight implies that a discernible horizon must be available, TC has been issuing approval for NVFR operations (routes, etc.) to operators in remote areas or areas with little or no ambient lighting. As a result, flights are commonly operated at night without cultural or celestial lighting that may provide discernible horizons. This practice leads flight crews to operate primarily with reference to instruments without the safeguards provided by the IFR regulations and standards.
If TC continues to allow night flights to be carried out under VFR with inadequate visual references, there is a risk of controlled-flight-into-terrain and loss-of-control accidents.
The occurrence flight was operated in weather that met the criteria for NVFR but had limited celestial illumination over an area with almost non-existent cultural lighting. During the flight to CYAZ, the flight crew remarked on the level of darkness and the absence of visible stars. Under these conditions, no discernible horizon or visual contact with the surface would have been available to the flight crew.
Helijet's landing plate for CYAZ cautions pilots that there is minimal ambient lighting at the airport and the surrounding area, and that the aerodrome is unlit.
After the autopilot was decoupled, the only visual cues available to assist the flight crew were the illuminated windsock and the 12 green Turboflares on the temporary night helipad. For much of the approach, the Turboflares would have appeared as a single light source.
The flight was conducted under NVFR without sufficient ambient or cultural lighting to maintain adequate visual reference to the surface.
2.2.2 Night vision imaging systems
Canada has vast areas with little or no cultural lighting to help a pilot maintain visual reference to the surface during unaided NVFR operations. In these regions, maintaining visual reference to the surface requires clear skies and significant celestial lighting, or the use of some type of night-vision imaging system.
In 2006, the U.S. National Transportation Safety Board (NTSB) published the Special Investigation Report on Emergency Medical Services Operations. This report highlighted the potential benefits of night-vision goggles (NVGs), but the NTSB did not issue a recommendation at that time to require their use. In 2009, the NTSB recommended that the Federal Aviation Administration (FAA) require helicopter emergency medical services (HEMS) operators to install night vision imaging systems equipment, and that pilots be trained in their use during night operations. To date, the FAA has not made night vision imaging systems a regulatory requirement for HEMS operations. However, more than 90% of HEMS operators in the U.S. have adopted NVGs to take advantage of the enhanced situational awareness and increased level of safety afforded by their use.
Other countries have introduced regulations requiring night vision imaging systems for night HEMS operations, and have introduced specific regulations related to the approval of night vision imaging systems for NVFR operations.
In Canada, there is currently no requirement for night vision imaging systems to be used in HEMS or any other operation. Nevertheless, in recent years, there has been a significant increase in the number of operators that have adopted some type of night vision imaging system. With the emergence of newer-generation NVGs, many of the limitations of earlier versions are no longer factors that deter operators from adopting them. Consequently, NVG use among the civil rotary-wing community has steadily increased.
Helijet aircraft are not equipped with night vision imaging systems, although the company routinely conducts NVFR flights over large areas with little or no cultural lighting. In weather that is technically suitable for VFR but provides little ambient lighting, it is not always possible to conduct these flights with visual reference to the surface. Even if such flights are begun with reference to the surface, there is a risk—especially in remote areas with limited weather forecasting—that conditions along the route will change and the required visual reference to the surface will be lost.
If, during NVFR operations, pilots continue flight in conditions where no cultural or ambient lighting exists and there is no alternate means of maintaining visual reference to the surface, there is an increased risk of controlled-flight-into-terrain and loss-of-control accidents.
2.2.3 Training
Helijet's TC-approved training syllabus did not include specific training regarding NVFR approaches and the black-hole illusion. Although such training is not currently required by regulation, other operators surveyed include mandatory black hole–specific training as part of their approved syllabi.
Helijet aircraft were operating in a number of locations that presented challenging night approaches with few visual references. To be effective, training must be designed to meet the operational needs of the company, be effectively delivered, and be followed up with recurrent training to encourage ongoing skills retention and development.
If flight crews do not receive effective training in NVFR operations and the associated illusions, they are at risk of not being adequately prepared for the challenges of flying in a night environment.
2.3 Crew preparation and coordination
As noted above, a night approach and landing at CYAZ presents operational challenges to flight crew. Specifically, the lack of ambient light at that location means that there is no horizon available by which to judge the attitude of the helicopter, and the lack of cultural lighting provides insufficient reference to help judge distance or approach angle.
Despite these challenges, this task can be carried out successfully if the crew are appropriately prepared for the conditions. Proper preparation helps the crew anticipate the conditions they will encounter, clearly understand their roles during the approach and landing, and ensure that they are prepared to respond to unsafe conditions encountered during the approach and landing. Effective preparation helps crews develop an effective mental model of the operational conditions they will encounter, which is critical to developing and maintaining situational awareness in flight.
2.3.1 Briefings
Operational briefings provide an important opportunity for crew to review relevant operational information and develop plans to respond to anticipated operational challenges. In this occurrence, the crew had not reviewed the landing plate prior to the flight. Further, the environmental conditions for the arrival at CYAZ, and the fact that neither crew member had previously flown into CYAZ at night, were not discussed before arrival. As a result, the crew had not established an accurate individual or shared mental model of the destination or its associated hazards.
Helijet's air ambulance SOPs mandated that crews conduct a crew briefing prior to the flight, which "should include information about procedures that are seldom used." Footnote 85 The SOPs also required an IFR check Footnote 86 and a landing briefing as part of the initial approach check. Footnote 87 The purpose of the landing briefing was to "outline the visual landing including the direction of approach, touchdown point and taxi intentions." Footnote 88
By not conducting thorough briefings, the crew missed opportunities to review the available information about aerodrome conditions at CYAZ and to discuss the risks of a night approach to a temporary helipad at an unlit aerodrome, in an area with little ambient and cultural lighting. The investigation determined that, in practice, senior pilots sometimes tailored their briefings when flying with other senior pilots or if approaching more familiar landing sites, such as airports or hospital helipads. This practice created scope for the occurrence crew to tailor their briefings based on their perceived experience and seniority.
Required briefings were not conducted. As a result, by the final approach, neither crew member had developed a correct or complete mental model of the landing site.
The accepted practice of not fully briefing all approaches contributed to the ineffective crew coordination in this occurrence, reducing information exchanged between 2 senior crew members.
2.3.2 Effect of crew pairing on crew coordination
The authority gradient between flight crew members is driven by qualifications and experience. An equal level of authority (a "flat" authority gradient) may present crew resource management (CRM) hazards, such as assumptions of competence or ineffective communications or cross-checking behaviours. Robust SOPs and thorough pre-flight briefings of roles and responsibilities mitigate the risks associated with a flat authority gradient.
According to the company's air ambulance SOPs:
Unless otherwise specifically assigned by the Chief Pilot, the PIC [pilot-in-command], who is the pilot-in-command for all flights by that crew, will be the pilot whose name appears highest on the latest list as published by the Chief Pilot for this purpose. Footnote 89
This crew-pairing strategy would therefore result in a natural gradient in authority. In the case of the occurrence crew, the on-duty pilot (the PIC) had been with the company the longest and had more hours on type, and was thus higher up on the Helijet pilot list. However, the first officer (the PF) was also a training captain, and had previously held the assistant chief pilot position. This closeness in seniority levels reduced the authority gradient between the 2 pilots.
The potential hazards of the recognized flat authority gradient were not addressed by the crew, and they proceeded with the flight with their own assumptions about the other crew member's knowledge, skills, and abilities, and with a level of respect that made them less inclined to question each other. Because both pilots were aware of the other's seniority, and because there was an informal practice of tailoring briefings according to the seniority of the crew and the destination, both pilots adopted a more relaxed information exchange. As a result, the crew did not review the landing plates, did not conduct comprehensive briefings, and missed multiple opportunities to correct misunderstandings.
The flat authority gradient in the cockpit was not identified and addressed by the crew, and the corresponding assumptions of crew skill and experience directly affected the quality of resource management and communication style.
2.4 Standard operating procedures
Effective SOPs are a framework for consistent and safe operations. They establish expectations and norms with respect to specific operations, and set parameters that enable detection of deviations from standard flight profiles. As required by regulation, Helijet had established SOPs for its air ambulance operations. However, these SOPs provided minimal detail in a number of areas.
2.4.1 Specifications for briefings
Effective briefings help crews identify the risks associated with an operation and develop common expectations of how those risks will be managed. SOPs must provide sufficient structure to ensure that briefings are consistently carried out while providing sufficient flexibility to ensure that they are also short and relevant to the operation.
In this occurrence, the briefings conducted by the crew did not address the risks associated with a black-hole arrival or the flat authority gradient between the 2 crew members.
Helijet's SOPs specified briefings requirements, including crew briefings before flight, IFR approach briefings, and landing briefings. The before-flight briefing procedure required the PIC to ensure that information was obtained and that a thorough pre-flight briefing was carried out that covered, at a minimum, weather, fuel load, payload, flight time, work to be carried out, and any additional duties.
SOPs from other helicopter medical evacuation (medevac) operators were reviewed during the course of the investigation. It was noted that other operators provided more detailed briefing formats and checklists to prompt crews to consider specific hazards, including light levels, and to conduct a mission risk assessment as part of their pre-flight preparation.
2.4.2 Overall night requirements
There are specific risks associated with NVFR flight that require increased awareness on the part of flight crew regarding terrain and obstacles, as well as an increased readiness to fly using reference to flight instruments. SOPs play an important role in ensuring that the crew are prepared for the conditions encountered on an NVFR flight.
Helijet's air ambulance SOPs set out few requirements specific to NVFR operations. References to night flight in the SOPs included
- instructions for use of the radar altimeter during an NVFR approach;
- limitations on use of autopilot during an NVFR departure and below 1000 feet during an NVFR approach; and
- instructions for initiating descent below minimum descent altitude at night.
A review of other air ambulance SOPs conducted as part of the investigation indicated that other operators provided more specific night flight procedures. For example, other operators provided dedicated procedures that outlined flight planning procedures, weather minima, and specifications that unaided approaches could be conducted only to illuminated areas.
2.4.3 Black-hole procedures
The airport environment at CYAZ met the accepted definition of a black hole. The aerodrome was unlit and surrounded by water and terrain with no cultural lighting. The temporary night helipad lit with Turboflares presented as a single point in space to an approaching helicopter, and offered little reference from which to judge rate of closure or descent profile.
A review of other operators' SOPs revealed that some operators provided specific black-hole procedures that included a procedure to transition from the minimum obstacle clearance altitude to the approach profile, standard calls to assist in monitoring the approach, a specific approach briefing tailored to the black-hole procedure, and clear criteria for conducting a go-around if the approach to the helipad departed from certain parameters.
When outside visual clues are insufficient to maintain control of the aircraft, the flight crew should be prepared to initiate a go-around.
Although Helijet operated into CYAZ and several other locations that had the potential to produce the effects of a black hole, the company had no specific SOPs or guidance related to black-hole environments.
Helijet's SOPs provided little guidance in a number of areas, including crew briefings, NVFR requirements, and black-hole approach and landing procedures. As a result, the flight crew conducted a visual approach without the benefit of effective SOPs, which contributed to poor decision making and coordination.
2.4.4 Regulatory requirement for standard operating procedures
Robust SOPs, founded on effective CRM principles, industry best practices, and operational experience, enhance operational safety. In CARs Subpart 705 operations, SOPs must be reviewed by TC, which gives the regulator insight into how a company is operating and how it compares to others in the sector. The review process also allows for input from the regulator when SOPs are inadequate or do not represent best practices. It may be beneficial for TC to review SOPs of multi-crew CARs Subpart 702, 703, and 704 operators during routine surveillance activities, particularly for new operators.
There is currently no regulatory process for multi-crew CARs Subpart 702, 703, and 704 operators to have company SOPs reviewed by TC. As a result, there is a risk that non-optimal procedures will be adopted.
2.5 Safety management and oversight
All transportation companies have a responsibility to effectively manage safety risks in their operations. While compliance with regulations will provide a baseline level of safety for the risks common to all operators, companies must be able to identify and mitigate the hazards specific to their operation in order to reduce risk to a level that is as low as reasonably practicable.
It is for this reason that the Transportation Safety Board of Canada (TSB), through its Watchlist and recommendations, has repeatedly called for all transportation companies to be required to implement a safety management system (SMS) and for that SMS to be audited to ensure that the processes it contains are in place and are effective. Although not required by regulation, Helijet had implemented an SMS to manage safety in its operations. At the time of the occurrence, the SMS was not yet fully developed, and it had not been assessed by TC.
This occurrence was the result of the risks associated with night operations not being effectively mitigated by the crew on the night of the occurrence, and more broadly by the company.
Helijet had been using the temporary night helipad at the Tofino airport for approximately 4 years before the occurrence. In addition, it was conducting night operations to a number of other locations where temporary helipads were used for the arrival and departure of medevac flights. In the case of CYAZ, TC had identified a number of mitigations to be implemented before night operations to the temporary night helipad could begin. However, only one of these mitigations had been implemented when night medevac flights began using CYAZ.
Landing and taking off on a helipad at night in an area with minimal cultural lighting is a challenging task, because there are few visual cues available to the pilot to help maintain orientation and to judge height and distance from the helipad.
Helijet had identified the hazard associated with the lack of cultural lighting and had provided crews with a VFR approach procedure for the temporary Tofino hospital landing site, located at CYAZ. On the landing plate for CYAZ, the section "Caution/Obstruction" stated: "Minimal ambient lighting at the airport and surrounding area. There is no runway lighting at this airport." However, there are other mitigations appropriate to landing at the temporary Tofino hospital landing site and other locations at night that were not considered or implemented by the company. These included developing specific night SOPs, providing crews with black-hole training, and having crews use night vision imaging systems. Although not required by regulations, such mitigations would have reduced the risks associated with night operations to helipads with minimal visual cues and cultural lighting, and would have been an indication of effective safety management.
The landing site at CYAZ had been established before the company's SMS was implemented, and no risk assessment of the landing site was conducted. The company did not adequately assess the hazards and risks of the new Tofino hospital landing procedures, despite the required mitigations not being fully implemented, and night medevac flights were being conducted to CYAZ, which was certified for daylight operations only. The investigation also found that, since the SMS had been implemented, few risk assessments had been carried out. The SMS manual provided minimal guidance for how risk assessments would be conducted and documented or how mitigations identified during a risk assessment would be implemented or tracked.
At the time of the occurrence, the reactive processes included in the SMS had been fully implemented and were being used for occurrence reporting. The SMS manual contained processes for filing and handling reactive safety reports. However, although the reporting system was effectively capturing specific categories of events (e.g., technical events such as engine chip lights), it was not being used to report hazards or unsafe conditions identified in the course of normal operations. As an example, approximately 1 month before the occurrence, a pilot had identified the need for additional lights to assist arriving and departing helicopters at CYAZ. Although the pilot communicated these concerns to the airport manager, they were never reported through the company's SMS. As a result, an opportunity to assess whether the requested changes would reduce the risks associated with the operations at CYAZ or the company's other temporary night landing sites was lost.
The proactive processes described in the Helijet SMS manual were not being used, and the reactive processes were limited to incident reporting. Because the processes described in Helijet's SMS were not being used effectively, the SMS did not help the company identify and mitigate the risks associated with its night medevac operations.
Successful implementation of an SMS requires a supportive organizational culture, which fosters the commitment, competence, and cognizance Footnote 90 required throughout the organization to actively participate in the SMS. In the case of Helijet, the director of safety had overall responsibility for the SMS. However, this role was combined with that of the director of flight operations. It was estimated that the director of safety / flight operations was devoting 2 hours per week to the safety role. At the time of the occurrence, other identified safety officer roles were vacant, meaning there were few additional resources that could be called upon for assistance. As a result, few risk assessments were being initiated by company managers, as outlined in the company SMS manual, and involvement in the SMS was limited to managing reactive SMS reports.
The SMS training syllabus did not have sufficient SMS-related training items. As a result, many senior safety managers did not have an adequate understanding of how to implement a formal SMS, or how to perform risk assessments. Many Helijet employees were unaware of the SMS or how to use it.
At the time of the occurrence, there was a lack of resources and training dedicated to the company's SMS, limiting its effectiveness in mitigating the risks in night operations.
The effective implementation of an SMS is a long-term process that requires a commitment to continual improvement to ensure that the processes necessary to improve safety are in place and working effectively. In previous investigations, the TSB has identified instances where an SMS was not required or where an SMS existed on paper but not in practice. As a result, the Board has issued recommendations Footnote 91 and reiterated in its 2016 Watchlist that all operators should be required to implement an SMS and that the SMS should have regulatory oversight to help ensure it is working effectively. In the case of Helijet, although the operator had voluntarily implemented an SMS, TC had not conducted any assessments of the company's SMS because the SMS was not required by regulation.
Unless all operators are required to have an SMS that is assessed by TC for effectiveness, there is an increased likelihood that the risks specific to an operator will go unidentified and unmitigated.
If identified hazards are not captured by a company's SMS, they may go unaddressed, increasing the risk of accidents.
If feedback and corrective actions are not provided to employees who report a hazard or an incident, it is less likely that employees will report further hazards and incidents.
2.6 Aircraft return to service
2.6.1 Exceedance data capture
In this occurrence, the helicopter experienced significant single-engine and combined torque exceedances, but this information was recorded only on the cockpit voice and flight data recorder (CVFDR), which is optional equipment. By design, the integrated instrument display system (IIDS) did not display any exceedances or warnings after the occurrence. After landing at CYAZ, the crew checked the IIDS maintenance page for exceedances, but none were displayed, in keeping with the design of the system. With the exceedance information unavailable in the field, the helicopter was returned to service and critical maintenance action had not been performed.
There is no standard system in the Sikorsky S-76C+ to capture transmission torque exceedances with both engines operating. As a result, the helicopter was returned to service in a non-airworthy condition.
2.6.2 Post-occurrence maintenance action
During the post-flight inspection on the ramp at CYAZ, the crew found oil on the main rotor blades and on the left side of the fuselage. Maintenance crews discovered a broken main rotor damper oil line and damage to all 4 main rotor spindles, which resulted from severe coning angles during the low-rpm state during recovery. The spindle damage was reported to Sikorsky, and the spindles and oil damper line were replaced.
At this point, Helijet was not aware of the prolonged NR droop below the normal governed range or of the torque exceedances of the helicopter, which Sikorsky would later identify as requiring a major inspection and an overhaul of its dynamic components.
2.6.3 Cockpit voice and flight data recorder
The occurrence helicopter was equipped with an optional CVFDR, which recorded the transmission torque parameter. When the helicopter was returned to Vancouver later on 15 November, the day of the occurrence, the CVFDR was secured and downloaded by Maxcraft Avionics Ltd. (Maxcraft).
On 16 November, Maxcraft provided Helijet with data that indicated the helicopter had experienced a peak single-engine torque in excess of 155%. The data provided also indicated that the manufacturer's maximum-allowable combined dual-engine transient limit of 230% torque for 10 seconds had been exceeded.
Before test-flying and ferrying the helicopter to Vancouver International Airport (CYVR) after the occurrence, Helijet maintenance crews disabled the CVFDR in an attempt to ensure that the data was not erased or overwritten. Although this action increases the likelihood that the data for the occurrence is preserved, if flight data and voice recording equipment are disabled, then critical information will not be captured if the aircraft is involved in another occurrence.
On 25 November, 10 days after the occurrence, the CVFDR was sent to the TSB Engineering Laboratory for download and analysis. The laboratory examination found that critical information contained in a service letter issued by Sikorsky had not been provided to Maxcraft by Helijet, and was not taken into consideration when the CVFDR was downloaded and analyzed. As a result, the data provided to Helijet by Maxcraft contained errors. The TSB laboratory established that a combined engine torque of 268% had occurred during the occurrence, and that the NR had reached a minimum of 77%.
If service letters issued by aircraft manufacturers are not consulted, there is an increased risk that critical maintenance tasks will not be carried out.
2.6.4 Return to service
On the day of the occurrence, after the main rotor spindles and damper oil line had been replaced, and following a successful test flight, the helicopter was deemed serviceable and flown to CYVR. The next day, Helijet returned the helicopter to active British Columbia Emergency Health Services flight operations without required maintenance to the drive system components having been carried out. If aircraft that are not airworthy are released for flight with required maintenance not completed, there is a risk that components will fail in flight, putting passengers' and pilots' lives at risk.
Sikorsky was aware that the helicopter had suffered damage to the main rotor spindles on 15 November, and that those components had been changed. However, it was not until the TSB contacted Sikorsky after the 25 November occurrence at CYVR that the manufacturer became aware of the torque exceedances and low rpm values during the 15 November occurrence. Based on this information, Sikorsky deemed the helicopter not airworthy until all dynamic components underwent inspection and overhaul maintenance procedures, and until each main rotor blade was inspected and tested for any bonding separation. If operators do not disclose the full details of occurrences to aircraft manufacturers, there is a risk that an aircraft that is not airworthy will be returned to service.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The flight was conducted under night visual flight rules without sufficient ambient or cultural lighting to maintain adequate visual reference to the surface.
- Required briefings were not conducted. As a result, by the final approach, neither crew member had developed a correct or complete mental model of the landing site.
- When the pilot flying realized that the location of the landing zone was closer than expected, the large control inputs made to adjust the descent angle and speed resulted in a hazardous approach profile.
- During the approach, both crew members were occupied with maintaining visual reference to the landing zone, and the hazardous approach profile went unrecognized.
- While a visual approach was being conducted to a temporary night helipad at an unlit aerodrome at night, positive control of the helicopter was lost.
- Helijet International Inc.'s standard operating procedures (SOPs) provided little guidance in a number of areas, including crew briefings, night visual flight rules requirements, and black-hole approach and landing procedures. As a result, the flight crew conducted a visual approach without the benefit of effective SOPs, which contributed to poor decision making and coordination.
- The flat authority gradient in the cockpit was not identified and addressed by the crew, and the corresponding assumptions of crew skill and experience directly affected the quality of resource management and communication style.
- The accepted practice of not fully briefing all approaches contributed to the ineffective crew coordination in this occurrence, reducing information exchanged between 2 senior crew members.
- Because the processes described in Helijet International Inc.'s safety management system (SMS) were not being used effectively, the SMS did not help the company identify and mitigate the risks associated with its night medical evacuation operations.
- At the time of the occurrence, there was a lack of resources and training dedicated to the company's SMS, limiting its effectiveness in mitigating the risks in night operations.
3.2 Findings as to risk
- Canadian Aviation Regulations section 602.115 does not define "visual reference to the surface," which has been widely interpreted by the industry to mean "visual meteorological conditions." As a result, night flights may be conducted with inadequate visual references, increasing the risk of controlled-flight-into-terrain and loss-of-control accidents.
- If Transport Canada continues to allow night flights to be carried out under visual flight rules with inadequate visual references, there is a risk of controlled-flight-into-terrain and loss-of-control accidents.
- If, during night visual flight rules operations, pilots continue flight in conditions where no cultural or ambient lighting exists and there is no alternate means of maintaining visual reference to the surface, there is an increased risk of controlled-flight-into-terrain and loss-of-control accidents.
- If flight crews do not receive effective training in night visual flight rules operations and the associated illusions, they are at risk of not being adequately prepared for the challenges of flying in a night environment.
- There is currently no regulatory process for multi-crew Canadian Aviation Regulations Subpart 702, 703, and 704 operators to have company SOPs reviewed by Transport Canada. As a result, there is a risk that non-optimal procedures will be adopted.
- Unless all operators are required to have an SMS that is assessed by Transport Canada for effectiveness, there is an increased likelihood that the risks specific to an operator will go unidentified and unmitigated.
- If identified hazards are not captured by a company's SMS, they may go unaddressed, increasing the risk of accidents.
- If feedback and corrective actions are not provided to employees who report a hazard or an incident, it is less likely that employees will report further hazards and incidents.
- If flight data and voice recording equipment are disabled, critical information will not be captured if the aircraft is involved in another occurrence.
- If service letters issued by aircraft manufacturers are not consulted, there is an increased risk that critical maintenance tasks will not be carried out.
- If aircraft that are not airworthy are released for flight with required maintenance not completed, there is a risk that components will fail in flight, putting passengers' and pilots' lives at risk.
- If operators do not disclose the full details of occurrences to aircraft manufacturers, there is a risk that an aircraft that is not airworthy will be returned to service.
3.3 Other findings
- There are no emergency procedures or guidance specified in Helijet International Inc.'s SOPs or operations manual for flight crew to deal with enhanced ground proximity warning system alerts or warnings.
- The operator was unaware that cockpit voice recordings are privileged under the Canadian Transportation Accident and Safety Board Act.
- At the time of the occurrence, the company was not using night-vision goggles, nor was it required to do so.
- Night medical evacuation flights were being conducted to Tofino/Long Beach Airport, which was certified for daylight operations only.
- There is no standard system in the Sikorsky S-76C+ to capture transmission torque exceedances with both engines operating. As a result, the helicopter was returned to service in a non-airworthy condition.
4.0 Safety action
4.1 Safety action taken
4.1.1 Transportation Safety Board of Canada
On 30 November 2017, the Transportation Safety Board of Canada issued a safety advisory letter addressed to the operator and Maxcraft Avionics Ltd. noting their role in the unauthorized release and communication of the occurrence aircraft's on-board recordings. The safety advisory letter reminded both entities that cockpit voice recordings are privileged under the Canadian Transportation Accident Investigation and Safety Board Act, and that any unlawful communication of these recordings is a punishable offence under the Act.
4.1.2 Helijet International Inc.
As a result of this occurrence, the operator has taken the following safety actions:
- The appropriate managers at Helijet International Inc. (Helijet) have been briefed on the procedures and protocols required to maintain privileged information with respect to downloading on-board recordings.
- Helijet expanded its annual crew resource management (CRM) course to include 18 hours of annual instruction. Flight paramedics have been encouraged to attend the training. Training pilots and the chief pilot have undergone CRM instructor training. The initial CRM course was attended by senior staff, including the chief executive officer.
- Pre-flight safety meetings have been established at the start of each shift and where required for specific flights.
- Helijet, in conjunction with the British Columbia Emergency Health Service (BCEHS), has completed a risk assessment and a risk management plan for night visual flight rules (NVFR) operations.
- Helijet conducted its own internal investigation into the root causes of the 15 November 2015 occurrence in Tofino.
- In cooperation with BCEHS aviation management, a "dispatch call to takeoff" timeline exercise was completed. From initial dispatch call, flight crews were timed to determine the period required to carefully carry out all tasks prior to becoming airborne. A revision to the standard operating procedures (SOPs) now requires flight crew to be airborne "in a timely fashion" rather than in a prescribed number of minutes.
- NVFR routes were reviewed for accuracy and regulatory compliance. Rural and remote locations that were previously serviced at night were reviewed for suitable lighting procedures. Service during the hours of darkness to several remote locations has been suspended due to their lack of cultural lighting.
- Helijet reviewed all prepared landing sites for company landing plate accuracy. Each prepared landing site was reviewed to determine whether a site visit was required and to assess risks related to obstructions, lighting, and first-responder training requirements.
- Helijet reviewed its company operations manual and SOPs for ambulance operations. SOPs referring to NVFR operations were amended to be more descriptive and prescriptive.
- The training program and syllabus have been reviewed and amended. A 20% increase in instructional time has been added, including a greater emphasis on CRM, NVFR operations, the black-hole effect, and unprepared landing sites.
- Helijet has hired a safety systems manager. Safety policy is now being revised annually and the safety management system (SMS) is now updated regularly with a new focus on risk and change management. A new SMS manual was issued; it included a new risk management and risk tolerability matrix, and a safety policy and objectives. Employee SMS training is ongoing. The emergency response manual has been revised.
- Two SMS assessments have been completed at Helijet. These were conducted by an independent auditor. The assessments found that there had been significant improvements in company culture. The safety-reporting database has also been improved and the filing of safety reports has increased.
- SMS, risk-management, and change-management training was completed for senior, middle--management, and leadership positions, and 45% of staff have received "introduction to SMS" training.
- Helijet has reviewed and closed all open SMS reports.
- BCEHS and Helijet have entered into a contractual modification agreement to upgrade the air ambulance service provided to BCEHS under the existing contract to include night vision imaging systems, namely night-vision goggles (NVGs). The NVG upgrade project is currently underway and includes purchasing NVG equipment, modifying aircraft, and training flight crews.
4.1.3 Tofino/Long Beach Airport
Tofino/Long Beach Airport has installed the necessary infrastructure for night operations, and was fully night-certified by Transport Canada on 09 January 2017.
This report concludes the Transportation Safety Board of Canada's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Global positioning system (GPS) area navigation (RNAV) global navigation satellite system (GNSS) Runway 29 approach to Tofino/Long Beach Airport
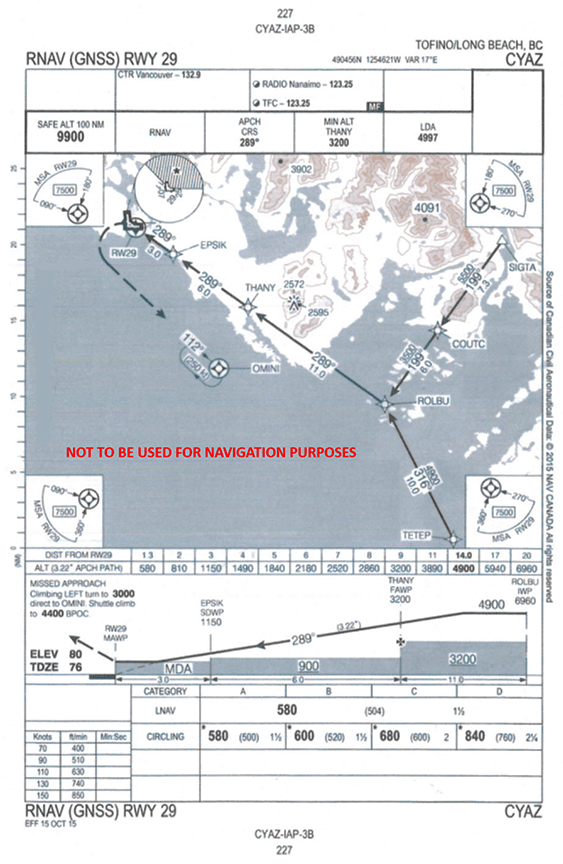
Source: NAV CANADA, Canada Air Pilot Instrument Procedures—British Columbia [CAP 2] (effective 15 October 2015)
Appendix B – Flight data from the occurrence helicopter's first approach to Tofino/Long Beach Airport
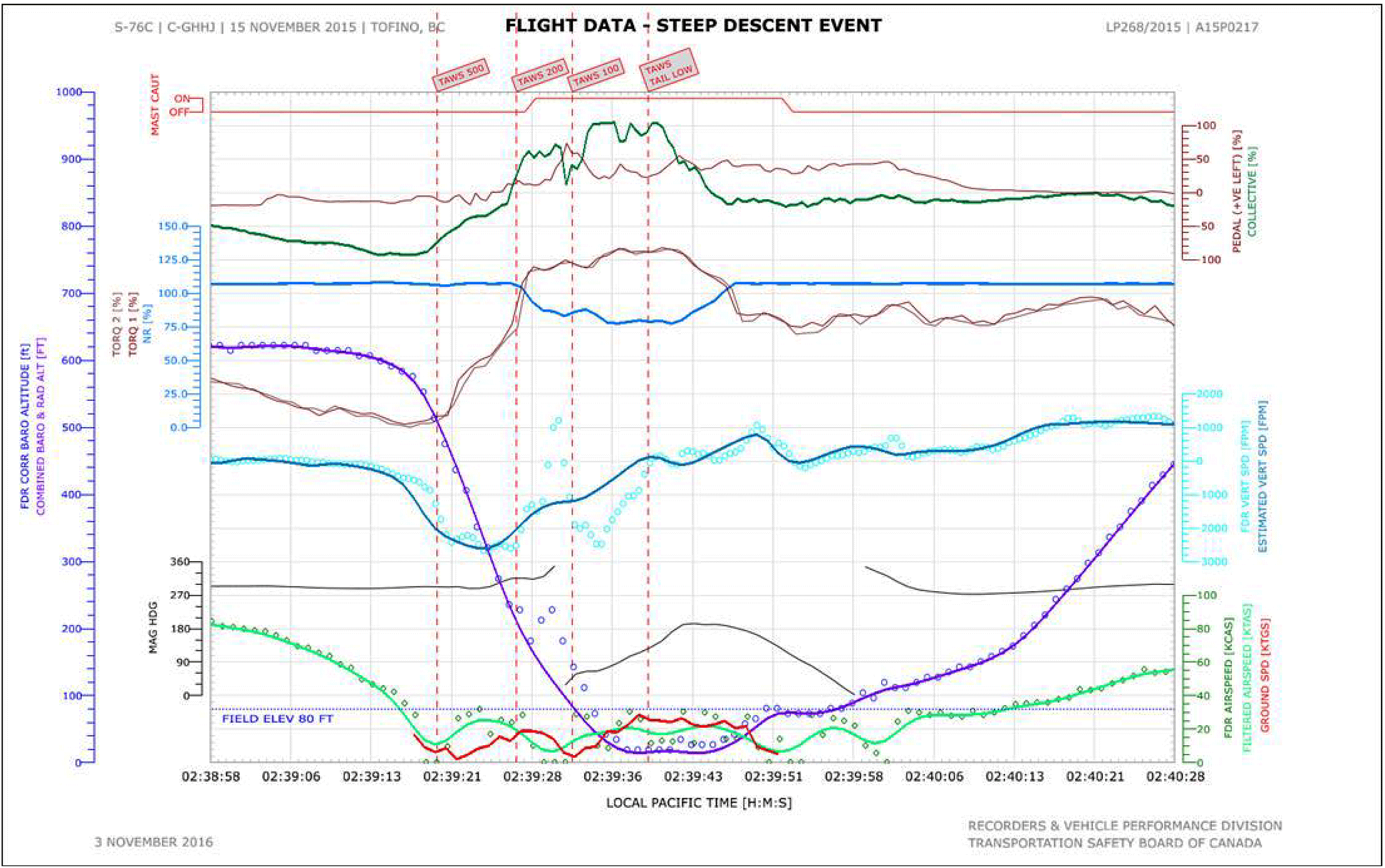
Appendix C – Occurrence helicopter powertrain limits and exceedances
| Sikorsky S-76C+ Rotorcraft Flight Manual limit description | Limit value | Actual value | Actual duration beyond limit |
|---|---|---|---|
| Rotor speed (NR): Minimum continuous Minimum transient |
106% 91% |
77% | 19 seconds 15 seconds |
| Engine torque: Maximum continuous Maximum transient |
104% 160% for 20 seconds |
134% | 19 seconds − |
| Transmission torque: Maximum continuous Maximum transient |
100% 115% for 10 seconds |
134% | 19 seconds 16 seconds |
| Power turbine speed (N2): Minimum continuous |
90.5% | 75% | 15 seconds |
Appendix D – Helijet International Inc. landing plate for Tofino hospital landing site
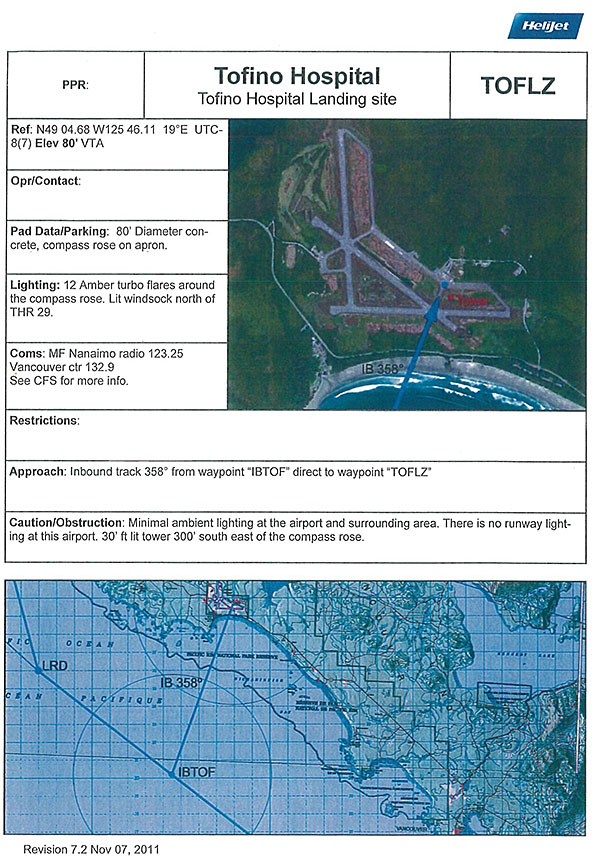
Source: Helijet International Inc.
Appendix E – Aerial and flight profile for Tofino/Long Beach Airport

Source: Google Earth, with TSB annotations
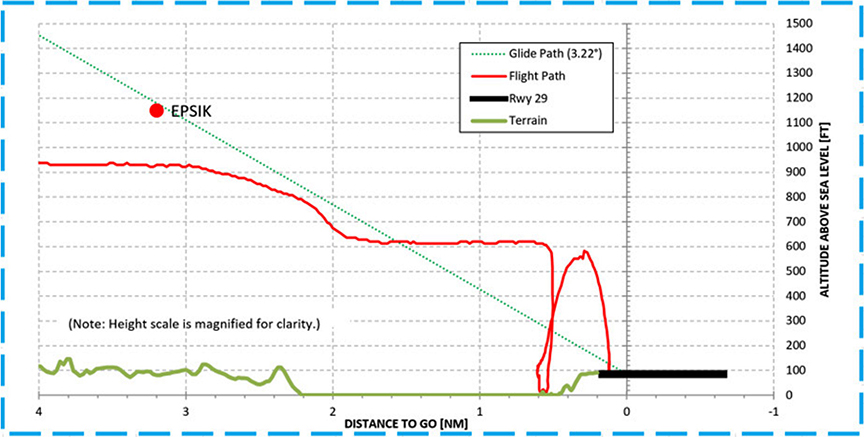
Appendix F – Flight data for both approaches in the occurrence