Runway overrun
Airmédic Inc.
Pilatus PC-12/47E, C-GIOX
Sept-Îles Airport, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 12 September 2021, the Airmédic Inc. Pilatus PC-12/47E aircraft (registration C-GIOX, serial number 1237) was conducting flight AM237 under instrument flight rules from Québec/Jean Lesage International Airport, Quebec, to Sept-Îles Airport, Quebec, with only 2 crew members on board. During final approach for Runway 09 at Sept-Îles Airport, when the aircraft was 1.6 nautical miles from the runway threshold, it was flying at 242 knots indicated airspeed. The aircraft crossed the runway threshold at 200 feet above ground level, at 180 knots indicated airspeed (ground speed of 191 knots); its rate of descent was 2000 fpm, the landing gear was in transit and the flaps were in the fully retracted position.
At 1709 Eastern Daylight Time, the aircraft landed approximately 2525 feet beyond the threshold of Runway 09, which was wet, at 159 knots indicated airspeed. Approximately 20 seconds later, the aircraft overran the runway at a ground speed of 57 knots and travelled approximately 590 feet in the grass before making a right turn around an approach light and returning to the runway. No one was injured. There was no damage to the aircraft.
1.0 Factual information
1.1 History of the flight
On 12 September 2021, the 2 pilots of the Airmédic Inc. (Airmedic) Pilatus PC-12/47E aircraft (PC-12 NG) went to the Montréal/St-Hubert Airport (CYHU), Quebec, to begin their workday at 0600.Footnote 1 That day, they were scheduled to conduct a series of 5 flights between 6 airports in Quebec (Figure 1).
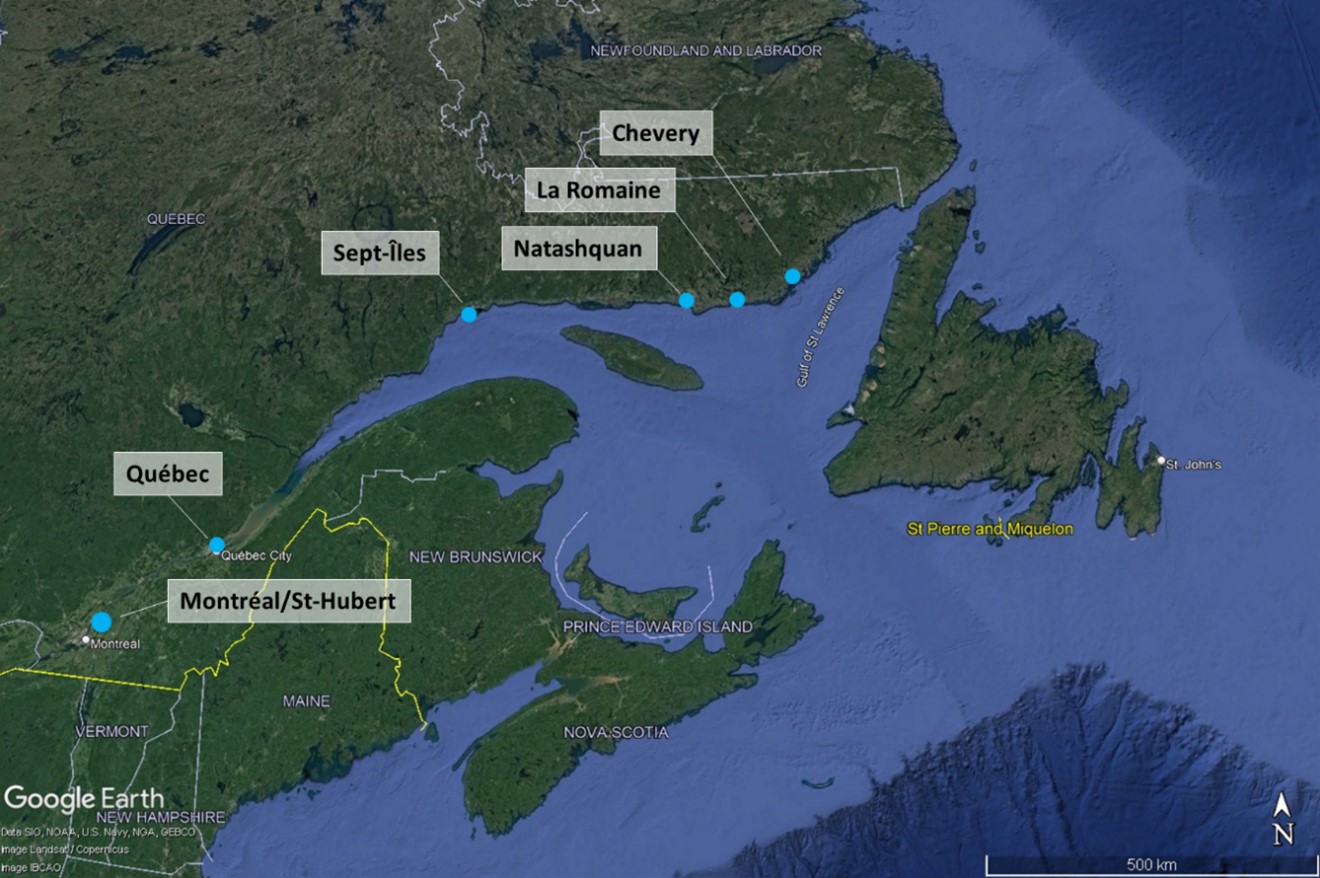
The flights were scheduled in the following order:
- from CYHU to the Chevery Airport (CYHR);
- from CYHR to the Natashquan Airport (CYNA);
- from CYNA to the Québec/Jean Lesage International Airport (CYQB);
- from CYQB to the Sept-Îles Airport (CYZV);
- from CYZV to La Romaine Airport (CTT5).
The first flight of the day (from CYHU) was scheduled to depart at 0700 and the last flight (to CTT5) was scheduled to arrive at 1745. At 0657, the crew began the series of flights under call sign AM237. The first 3 flights proceeded without incident. The aircraft landed at CYQB at 1346.
At 1600, the aircraft took off from CYQB, bound for CYZV with no passengers on board. The captain was sitting in the left seat and was the pilot flying (PF). The first officer (FO) was sitting in the right seat and was the pilot not flying (PNF).
Shortly before initiating the descent from flight level 270, the crew began its preparation for approach and landing at CYZV. The captain told the FO that he was going to show him that it was possible to conduct a late descent at a rate of descent of approximately 3000 fpm with the Pilatus PC-12.
The crew obtained the weather conditions from the information Kilo message issued by the automatic terminal information service (ATIS)Footnote 2 at CYZV, which indicated visual flight conditions with moderate rain showers, mist and variable winds from the west at 8 knots, gusting to 15 knots.
The captain told the FO that he wanted to conduct the straight-in approach to Runway 09 despite the tailwind. He then gave his approach briefing for a Runway 09 area navigation (RNAV) approach using the global navigation satellite system (GNSS) (Appendix A). The briefing indicated that the flaps would be set to 15° and the landing reference speed (Vref) would be 95 knots indicated airspeed (KIAS).
The descent was initiated at approximately 1650, and at 1703, the FO contacted the CYZV flight service specialist on mandatory frequency (MF) 118.1 MHz. The crew was informed that the winds were from 220° magnetic (M) at 6 knots.
At 1705, the aircraft crossed the ETBAR initial approach waypoint at 5078 feet above sea level (ASL), which was approximately 250 feet above the 3° approach slope, at 213 KIAS. The crew had Runway 09 in sight, and the captain decided to accelerate to conduct a high-speed final approach, decelerating just before reaching the runway. Incorrectly believing that the airspeed limit of 210 knots published on the approach chart for the IGSUK and VOKON waypoints also applied to the straight-in approach via ETBAR, the captain asked the FO to cancel the instrument flight rules (IFR) flight plan so that they could continue the approach under visual flight rules (VFR), which have no airspeed limit.
The captain then increased power without consulting the FO. The aircraft’s speed increased to 240 KIAS, the manufacturer’s maximum operating speed (Vmo). The FO called out high speed. The captain reduced power to stabilize the speed around 230 KIAS. At that point, the FO expressed his discomfort with the high speed. However, the captain stated that he was going to continue the high-speed approach. At approximately 6 nautical miles (NM) from the runway, the FO expressed his doubts that the landing would be successful, and the captain repeated that he was going to continue the high-speed approach.
At 1707:33, the aircraft crossed the DENEZ final approach fix on the 3° approach slope at 233 KIAS.
At 1708:08, the aircraft descended through 1000 feet above ground level (AGL) at 236 KIAS in clean configuration (landing gear and flaps retracted), and 17 seconds later, it descended through 500 feet AGL, for the first time, at 238 KIAS. One second later, the aircraft exceeded the Vmo of 240 KIAS and remained in overspeed for 3 seconds. The captain reduced power and the speed reached 244 KIAS before dropping back below the Vmo. Two seconds later, the captain initiated a climb to reduce the aircraft’s speed more quickly. When the aircraft was at 195 KIAS, the captain called “gear down” to have the FO lower the landing gear. At that point, the FO called out high speed, given that the maximum landing gear operating speed is 180 KIAS. The captain repeated “gear down.” The landing gear extension was initiated at 188 KIAS, 8 knots above the maximum speed of 180 KIAS. The FO then asked the captain to confirm the flap selection of 15° given that the aircraft’s speed was then around 185 KIAS, which was 20 KIAS greater than the maximum speed with flaps extended. The captain replied that the landing would be conducted without flaps.
At 1708:53, the aircraft crossed the runway threshold at 200 feet AGL, at 180 KIAS (ground speed of 191 knots); its rate of descent was 2000 fpm, the landing gear was in transit, and the flaps were in the fully retracted position.
At 1709:02, the aircraft touched down fairly smoothly on the wet runway, approximately 2525 feet beyond the runway threshold, at 159 KIAS (ground speed of 167 knots).Footnote 3 The brakes were then applied forcefully and reverse thrust was applied the way the captain normally would (i.e., in idle reverse).
At 1709:17, realizing that a runway overrun was imminent, the captain increased the reverse thrust to 48% of the maximum and, 6 seconds later, the aircraft overran the runway at a ground speed of 57 knots.
The aircraft veered slightly to the left to avoid the approach lights. After travelling 590 feet in the grass at the end of the runway, the captain reversed course to the right, around an approach light, and increased power to return to the runway. After the runway overrun, the crew informed the flight service specialist that the aircraft had not hit anything and that there was no damage. The aircraft then taxied normally to its parking stand. The crew was not injured.
1.2 Injuries to persons
There were no injuries.
1.3 Damage to aircraft
The aircraft was not damaged; however, the tires on the main landing gear showed signs of rubber reversion (figures 2 and 3).


1.4 Other damage
There was no other damage.
1.5 Personnel information
The flight crew consisted of 2 members, whose respective ratings and flight hours are described in Table 1 below.
| Captain | First officer | |
|---|---|---|
| Pilot licence | Commercial pilot licence | Commercial pilot licence |
| Medical expiry date | 01 October 2021 | 01 May 2022 |
| Total flying hours | 3187 | 1080 |
| Flight hours on type | 2867 | 280 |
| Flight hours in the 7 days before the occurrence | 11 | 17 |
| Flight hours in the 30 days before the occurrence | 68 | 67 |
| Flight hours in the 90 days before the occurrence | 226 | 227 |
| Flight hours on type in the 90 days before the occurrence | 226 | 202 |
| Hours on duty before the occurrence | 11 | 11 |
| Hours off duty before the work period | 92 | 92 |
The flight crew held the appropriate licences and ratings for the flight in accordance with existing regulations. The captain had previous experience as captain of a Pilatus PC-12 when he joined Airmedic in September 2019, and completed his training in January 2020, including a pilot proficiency check (PPC). His last PPC was carried out in January 2021. On 30 April 2021, the captain was subject to administrative and disciplinary measures by the company due to previous occurrences.
The FO had no flight experience on the Pilatus PC-12 when he joined Airmedic in 2019, where he held various positions. He had obtained his PPC in April 2021.
The crew had accumulated approximately 11 hours of continuous service at the time of the occurrence. A review of the flight crew’s work/rest schedules determined that no fatigue-related factors were present in this occurrence.
1.6 Aircraft information
The occurrence aircraft is a Pilatus PC-12/47E, commercially known as a PC-12 NG (Next Generation); it was therefore equipped with enhanced avionics and an engine slightly more powerful than its predecessors (Table 2).
| Manufacturer | Pilatus Aircraft Ltd. |
|---|---|
| Type, model, and registration | PC-12/47E, C-GIOX |
| Year of manufacture | 2010 |
| Serial number | 1237 |
| Certificate of airworthiness issue date | 19 August 2019 |
| Total airframe time | 4660.4 hours |
| Engine type (number of engines) | Pratt & Whitney Canada PT6A-67P (1) |
| Propeller type (number of propellers) | Hartzell HC-E4A-3D (1) |
| Maximum allowable take-off weight | 10 450 lb (4740 kg) |
| Recommended fuel types | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A-1 |
There were no recorded outstanding defects at the time of the occurrence. There was no indication that a component or system malfunction played a role in this occurrence.
The aircraft was configured to carry a maximum of 7 passengers. On the occurrence flight, the take-off weight was 9710.1 pounds (maximum take-off weight: 10 450 pounds) and the expected landing weight was 9185.1 pounds (maximum landing weight: 9921 pounds).The aircraft’s weight and centre of gravity were within the manufacturer’s prescribed limits.
1.6.1 Landing distances
For the purposes of this investigation, normal landing distances in the 3 flap configurations (40°, 15°, and 0°) were calculated using Pilatus Aircraft Ltd.’s “PC-12 Calculator” application. Calculations were made for the conditions of the occurrence flight, Footnote 4 but with the normal threshold crossing of 50 feet AGL, and speed stabilized at the appropriate approach speed for the configuration, a dry runway, average brake application, and no use of reverse thrust.
There are no certification data for a wet runway, and therefore no published data for wet runways (Table 3).
| Flap configuration | Final approach speed* (knots) |
Distance (calculated) from the threshold on touchdown (feet) | Landing roll (feet) | Total distance (feet) |
|---|---|---|---|---|
| F40 | 82 | 945 | 1303 | 2248 |
| F15 | 95 | 1238 | 1707 | 2945 |
| F0 | 115 | 1729 | 2385 | 4114 |
* Pilatus Aircraft Ltd. uses the term final approach speed (Vapp) in its PC-12 Calculator application and in the performance tables published in its Pilatus PC-12 pilot’s operating handbook. Airmedic’s standard operating procedures (SOPs) mainly use Vref to refer to the final approach speed.
At the TSB’s request, the manufacturer provided an estimate of the landing distance for the occurrence aircraft on a dry runway, based on the occurrence flight’s configuration and conditions (crossing the threshold at 200 feet AGL at 180 KIAS), with maximum braking in the 2 seconds after landing, first with no reverse thrust and then with maximum reverse thrust (Table 4).
| Configuration (flaps/ braking/reverse thrust) | Ground speed on touchdown (knots) |
Distance (calculated) from the threshold on touchdown (feet) |
Landing roll (feet) |
Total distance (feet) |
|---|---|---|---|---|
| F0/maximum/nil | 167 | 2525 | 4645 | 7170 |
| F0/maximum/maximum | 167 | 2525 | 3870 | 6395 |
Data from the occurrence flight were used to obtain the rate of deceleration on the runway and compare it with the rate of deceleration obtained during test flights for aircraft certification on a dry runway. This comparison led to the conclusion that the occurrence aircraft’s rate of deceleration was slightly higher than the rates obtained on a dry runway (0.25g) with no reverse thrust.
1.6.2 Deceleration in flight
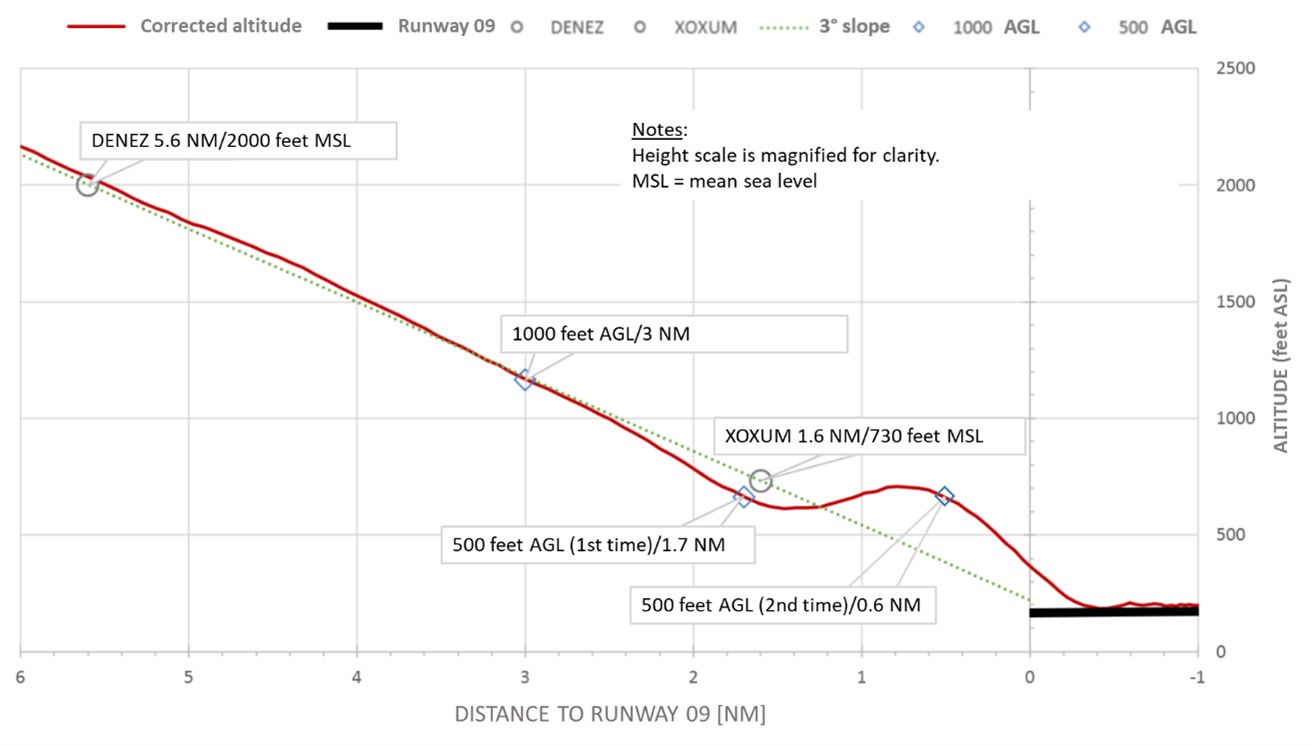
According to data from the occurrence flight, during the slight climb intended to slow the aircraft on short final, the rate of deceleration obtained was approximately 4 knots per second. Based on this rate of deceleration, the theoretical time to reach the configuration change speeds and to descend and cross the runway threshold at 50 feet AGL at the Vref was calculated to be 35 seconds (Table 5).
| Position 1 | Position 2 | |
|---|---|---|
| Distance from runway threshold | 3.0 NM | 1.7 NM |
| Time | 1708:08 | 1708:25 |
| Altitude | 1000 feet AGL | 500 feet AGL (1st time) |
| Indicated airspeed | 236 KIAS | 238 KIAS |
| Actual time to reach the runway threshold | 45 s | 28 s |
| Theoretical start of deceleration | 00:00:00 | |
| Deceleration to 180 knots and landing gear extension selection | 00:00:14 | |
| Deceleration to 165 knots and 15° flap selection | 00:00:03 | |
| Deceleration to 95-knot Vref during descent to 50 feet AGL | 00:00:18 | |
| Total theoretical deceleration time | 35 s | |
| Difference (actual time vs theoretical time) | +10 s | −7 s |
According to the same flight data, it took the aircraft 45 seconds to reach the runway from the time it crossed 1000 feet AGL, and 28 seconds from the time it crossed 500 feet AGL the first time (Appendix B).
1.7 Meteorological information
The graphic area forecast Clouds and Weather chart for the region, issued at 1328 on 12 September 2021 and valid from 1400, indicated the presence of a low-pressure system north-northwest of CYZV and a cold front to the west, which was moving eastward at 30 knots. According to wind and temperature aloft forecasts, winds from 240° true (T) at 23 knots were forecast for CYZV between 1300 and 1700 at 3000 feet ASL.
The aerodrome forecastFootnote 5 for CYZV, updated at 1056 on 12 September 2021 and valid from 1000 on 12 September until 0800 the next day, indicated the following as of 1600:
- winds from 220°T at 12 knots;
- visibility of 6 SM;
- light rain showers and mist;
- scattered clouds at 600 feet AGL;
- overcast ceiling at 2000 feet AGL.
Between 1600 and 2000, there was a 30% chance of the following conditions:
- visibility of 2 SM;
- thunderstorms, moderate rain showers and mist;
- broken ceiling at 600 feet;
- overcast cloud layer at 2000 feet with cumulonimbus.
The crew obtained updated weather conditions from the ATIS information Kilo message, which had been issued at 1600 and indicated the following:
- variable winds from 220°M to 280°M at 8 knots, gusting to 15 knots;
- visibility of 3 SM;
- moderate rain showers and mist;
- scattered clouds at 900 feet AGL;
- broken ceiling at 2000 feet AGL;
- broken cloud layer at 4000 feet AGL;
- overcast cloud layer at 7500 feet AGL;
- temperature 14 °C, dew point 13 °C;
- altimeter setting 29.59 inches of mercury (inHg).
The aerodrome routine meteorological report issued at 1700 on 12 September 2021 for CYZV was the following:
- winds from 190°TFootnote 6 at 6 knots;
- visibility of 20 SM;
- light rain showers;
- few clouds at 900 feet AGL;
- few clouds at 2000 feet AGL;
- broken ceiling at 4500 feet AGL with towering cumulus;
- broken cloud layer at 8000 feet AGL;
- temperature 13 °C, dew point 12 °C;
- altimeter setting 29.57 inHg.
At 1719, 10 minutes after landing, an aerodrome special meteorological report (SPECI)Footnote 7 was issued for CYZV, indicating the following:
- winds from 230°T at 10 knots;
- few clouds at 400 feet AGL;
- few clouds at 900 feet AGL;
- broken ceiling at 4000 feet AGL with towering cumulus;
- broken cloud layer at 10 000 feet AGL;
- temperature 14 °C, dew point 12 °C;
- altimeter setting 29.57 inHg.
1.8 Aids to navigation
Not applicable.
1.9 Communications
CYZV is located in a control zone (Class E airspace) with a radius of 5 NM, in which a mandatory frequency area (MF area) was established on frequency 118.1 MHz. The CYZV flight service station provides aerodrome advisory service to aircraft operating within the CYZV MF area.
1.10 Aerodrome information
![Illustration of the omnidirectional approach lighting system (Source: Transport Canada, Transport Canada Aeronautical Information Manual, AGA — Aerodromes [24 March 2022])](/sites/default/files/eng/rapports-reports/aviation/2021/a21q0087/images/a21q0087-figure-04.jpg)
CYZV is located approximately 4 NM east of the city of Sept-Îles, at an elevation of 180 feet ASL. It has 2 asphalt runways: Runway 09/27, which is 6552 feet long and 150 feet wide, and Runway 13/31, which is 5771 feet long and 200 feet wide (Appendix C). Runway 13/31 was closed by NOTAM from 31 August 2021 to 30 September 2021. Runway 09/27 complies with the applicable standardsFootnote 8 and includes a grass clearwayFootnote 9 that is 300 m (984 feet) long and 75 m (246 feet) wide. The runway does not have a runway end safety area, nor is one required by existing regulations.
Runway 27 (opposite end of Runway 09) has an omnidirectional approach lighting system (ODALS) (Figure 4). As described in the Transport Canada Aeronautical Information Manual,
[t]his system is a configuration of seven omnidirectional, variable-intensity, sequenced flashing lights. […] There are five lights on the extended centreline, commencing 90 m from the threshold and spaced 90 m apart over a total distance of 450 m. Two lights are positioned 12 m to the left and right of the threshold.Footnote 10
The aircraft was not damaged on the clearway, which was grassy and solid enough to support the weight of the aircraft.
1.10.1 Post-incident inspection
The captain, who had managed to avoid the ODALS before turning around to return to the runway, informed the flight service specialist that the aircraft had not hit anything and that there was no damage. Seeing that the aircraft was taxiing normally toward the apron, the flight service specialist did not immediately inform the airport operator, but did make a detailed aviation occurrence report at the time. The post-incident inspection of the installations at the end of Runway 09 was carried out the next day, when the airport operator learned that a runway overrun had occurred. No damage was found.
1.10.2 Runway surface conditions
CYZV assesses runway conditions based on Global Reporting FormatFootnote 11 criteria during published hours of operation, and only on request from a flight service specialist or an air operator outside of those hours. Given that the occurrence aircraft landed outside of the airport staff’s working hours, runway conditions were not assessed and were therefore not available to the crew for landing.
1.11 Flight recorders
The aircraft was not equipped with a flight data recorder or a cockpit voice recorder, nor was either required by existing regulations. However, the aircraft was equipped with an engine condition trend monitoring (ECTM) system that records certain data.Footnote 12 The data are sent to an external engine condition monitoring and maintenance tracking service provider. When a parameter exceedance is detected, the operator is notified and can access all of the data collected at the time of the exceedance. Airmedic was able to reconstruct the occurrence flight’s approach based on these data.
The company’s pilots knew that engine data were being recorded, but they were not aware that other data were also being recorded and were available in the event that a parameter was exceeded.
1.12 Wreckage and impact information
Not applicable.
1.13 Medical and pathological information
According to information obtained during the investigation, there was no indication that the pilots’ performance was affected by medical or physiological factors.
1.14 Fire
There was no fire.
1.15 Survival aspects
Not applicable.
1.16 Tests and research
The TSB laboratory in Ottawa, Ontario, combined the ECTM data with the NAV CANADA radar data to determine the aircraft’s flight path and condition during approach and landing. With these data, it was possible to analyze changes in speed, power and configuration during the approach, and to determine the speed and approximate touchdown point on the runway.
The laboratory produced a graphic representation of the aircraft’s vertical path in relation to the nominal 3° approach slope (Figure 5).
The TSB laboratory also produced graphs to illustrate the flight data plots (Appendix D), which helped establish significant events that occurred during the approach, with precise speeds and configurations (Appendix B).
1.16.1 TSB laboratory reports
The TSB completed the following laboratory report in support of this investigation:
- LP174/2021 – Radar Data Analysis
1.17 Organizational and management information
1.17.1 Operator
Airmedic is an air carrier based at CYHU that provides emergency medical assistance and airlift services. At the time of the occurrence, its fleet consisted of 3 helicopters and 6 airplanes (Pilatus PC-12s operated under Subpart 703, Air Taxi Operations, of the Canadian Aviation Regulations [CARs]).
1.17.1.1 Safety management system
Airmedic has a safety management system (SMS). However, given that the regulations do not require air-taxi operators to have an SMS in place, Transport Canada Civil Aviation (TCCA) does not assess or oversee SMSs put in place voluntarily.
Several TSB investigationsFootnote 13 have highlighted the need for TCCA to assess and oversee all SMSs. Furthermore, the TSB issued 2 recommendationsFootnote 14 related to SMSs and proactive safety management for all air operators. Lastly, safety management is a TSB Watchlist issue (see Section 1.18.7 TSB Watchlist).
1.17.1.2 Airmedic flight operations manual
Airmedic’s flight operations manual includes the requirements and training needed for crews to conduct non-precision approaches using the stabilized constant descent angle (SCDA) approach.Footnote 15 However, the manual does not contain any general or specific policies regarding the requirement to conduct a stabilized approach or to conduct a go-around if the approach is unstable.
1.17.1.3 Crew resource management training
Airmedic’s pilot training program includes initial and recurrent ground training on crew resource management (CRM), with case studies. Although the training covers communications, it does not specifically address how to manage deviations from standard operating procedures (SOPs).
1.17.1.4 Standard operating procedures
Airmedic’s SOPs were reviewed by TCCA, which verified that topics required by section 723.107 of Commercial Air Service Standard 723 were covered. On 28 September 2020, TCCA issued a letter of compliance to the company. SOP excerpts relevant to this occurrence are provided in Table 6.
| SOP reference | Text |
|---|---|
| 1.19 Standard Calls 1.19.1 General |
To reduce the likelihood of an incorrect interpretation of a request or command and to initiate corrective action for undesirable situations, a number of Standard Calls have been established. […] Abnormal speed Upon observing Abnormal Speed, the PNF should [emphasis added] call «Air Speed». The PF should [emphasis added] respond with «Check, correcting» and correct the speed to within the normal parameters, or if abnormal speed is necessary call «Intentional» and continue. |
| 2.29 Instrument Approach Procedures - Intermediate/Final 2.29.14 Stabilized Approach |
The Stabilized Approach configuration should be achieved no later than crossing the FAF/FAWP [final approach fix/final approach waypoint], or if there is no FAF immediately upon interception of the final approach track. Unless a stabilized approach is achieved crossing the FAF/FAWP or if there is no FAF while descending on the Final Approach Track, consideration should [emphasis added] be given to executing a «Go-around». Similarly, if one or more components of a previously stabilized approach are exceeded, consideration should [emphasis added] be given to calling a «Go-around» and executing the missed approach procedure. A Stabilized Approach configuration is defined as follows […]:
|
| 2.29.15 Stabilized Approach Criteria | The aircraft should be configured as follows passing the FAF/FAWP to meet the stabilized approach criteria:
|
| 2.29.21 Tolerances on Approach | Altitude: +100’, - 0’ Speed: +10 KTS to -5 KTS of the required speed VSI [vertical speed indicator]: 1000’ maximum starting from the procedure turn Track: LOC [localizer]: one dot on HSI [horizontal situation indicator] G/S [glide slope]: one dot on G/S ADF [automatic direction finder]: ± 5° of required track |
| 2.31 Contact/Visual Approach Procedures, VFR Circuits 2.31.1 General |
Configuration, completion of checks, Contact Approaches, Visual Approaches and VFR Circuits are treated as variations of the same type of procedure.
|
| 2.32 Missed Approach, Go-around/Balk Landing 2.32.1 Go-around - General |
During some approaches, it will become inadvisable to continue for landing. Should this occur, a "Go- around" should be [emphasis added] called and the missed approach procedure be completed. Guidance for specific conditions when a missed approach should be [emphasis added] initiated is detailed throughout these SOPs. Such guidance cannot address all circumstances. Accordingly, a "Go-around" may be initiated by either pilot whenever a landing becomes inadvisable. |
| 2.34 Landing Procedures 2.34.2 Landing Configurations & Before Landing Check |
Visual approaches: The airplane must be configured for landing and the Before Landing checklist must be completed before reaching 1000 feet AGL. |
| 2.35 Before Landing 2.35.1 Before Landing Check List |
When ready with IAS [indicated speed] ≤ 170 KIAS and decreasing, PF will call «Gear down, Landing Checks, Flaps 15» |
| 2.35.2 500 Feet Check | From this point, approach speed will be reduced from VTARGET 130KIAS to Vref and speed deviations call-out adjusted accordingly. |
| 2.36 Landing – Crew Coordination | Contact with the ground must always be made within the first 1/3 of the runway. |
1.17.1.5 Company guidelines
A few months before the occurrence, Airmedic received a passenger complaint regarding another crew that had made a deceleration manoeuvre resulting in a high rate of descent (which triggered a ground proximity warning system alert) and a mid-runway landing after a high-speed final approach.
In response to this complaint, the company met with and reprimanded the captain of that flight, and in August 2021, it issued an internal memorandumFootnote 16 to inform pilots that these types of manoeuvres were inappropriate. The memorandum explained why these manoeuvres were not to be executed. It also reminded pilots of the SOP sections that applied to that case, including Section 2.34.2. According to this section, pilots who are preparing to conduct a visual approach must configure the aircraft for landing and complete the before-landing checklist before crossing 1000 feet AGL.
1.17.2 Transport Canada Civil Aviation regulatory oversight
When Airmedic submitted an application for an air operator certificate for Pilatus PC-12 operations, TCCA ensured that all systems in place and key company personnel met regulatory requirements. Airmedic received its certificate on 30 September 2020. A new chief pilot was appointed in January 2021, followed by a new operations manager in April 2021.
As part of its regulatory oversight activities, TCCA tracked reports in the Civil Aviation Daily Occurrence Reporting System (CADORS) that pertained to Airmedic aircraft. For example, when an aircraft conducts a go-around, NAV CANADA produces an aviation occurrence report, which is sent to TCCA and added to the CADORS. TCCA then generally conducts a review with the company to understand the circumstances surrounding the occurrence. The data are collected and analyzed over several years to identify any significant changes within the same company.
At the time of the occurrence, TCCA had not performed any program validation inspections (PVI) or process inspections (PI) for Airmedic Pilatus PC-12 operations. However, after the occurrence, TCCA performed a reactive PI that resulted in 1 training-related finding and 6 observations, including one pertaining to the wording of the SOPs, which [translation] “do not provide standard calls at specific altitudes to determine whether or not stabilization criteria [read: stabilized approach criteria] are met” and which could [translation] “lead crew members to believe that they have discretion in applying stabilization criteria.” Footnote 17 In response, Airmedic submitted a corrective action plan to TCCA for the finding and observations in question.
According to the form that TCCA uses to record observations:
An observation issued by Transport Canada civil aviation (TCCA) is meant to highlight a discrepancy between the practices observed and the system, processes, or procedures described in your manuals or generally accepted safety standards or practices. It is intended to capture and communicate safety concern(s). Responding to an observation is voluntary. […] TCCA will receive and track responses, but will not approve/accept them. Observations and associated responses will be used as safety data to update the risk profile of the CAD [Canadian aviation document] holder, which in turn can have an impact on future surveillance scope and frequency determination. Footnote 18
1.17.2.1.1 Civil Aviation Safety Alert on stabilized approaches
TCCA issued Civil Aviation Safety Alert (CASA) 2015-04, the purpose of which was “to stress the importance of, and to outline the elements of a stabilized approach.”Footnote 19 The alert stated the following:
Stabilized approach criteria should be defined for all approaches and should include that:
- Approaches be stabilized by no lower than 1,000 feet (ft) above aerodrome elevation (AAE) when in instrument meteorological conditions (IMC);
- All approaches be stabilized by no lower than 500 ft AAE in visual meteorological conditions (VMC);
- A call be made upon reaching 1000 ft AAE in IMC or 500 ft AAE in VMC as to whether the approach is stabilized or not;
- The approach remain stabilized until landing;
- If an approach is not stabilized in accordance with these requirements, or has become destabilized afterwards, a go-around is required.Footnote 20
1.17.2.1.2 Review of standard operating procedures
In its Air Carrier Inspector Manual,Footnote 21 TCCA states that inspectors who review SOPs must be familiar with the aircraft type to which the SOPs apply, and must ensure that procedures contained in various company manuals do not contradict the aircraft flight manual or the flight operations manual. Lastly, TCCA inspectors must ensure that procedures comply with the regulationsFootnote 22 and are consistent with safe operating practices.
An official interpretation regarding SOP reviews was published in 2014 in TCCA’s National Aviation Safety Information Management System (NASIMS).Footnote 23 This interpretation concluded that “[w]ith such significant weightage placed on the SOP it is incumbent on TCCA to review the operator’s SOP for quality, consistency, accuracy, conciseness, clarity, relevancy and content.”Footnote 24
1.18 Additional information
1.18.1 Human factors
1.18.1.1 Decision making and situational awareness
Decision making is a cognitive process used to choose a plan of action from several possibilities. The process involves identifying issues and threats and assessing options, taking into account the associated risks. Crew decision making is carried out in a dynamic environment. It requires constant communication and consists of 4 steps: gathering information; processing information; making decisions; and acting on decisions. Decision making may be biased if the information gathering step is not done properly and if the information gathered is inaccurate; therefore, communication between the pilots of a crew is vital. Pilots must communicate available information to have the same understanding of the situation and be able to make the best decision.Footnote 25
Situational awareness is key to pilot and crew decision making. Situational awareness is the perception of the elements in the environment, the comprehension of their meaning, and the projection of their status in the future.Footnote 26 In a dynamic environment, situational awareness requires “continuous extraction of environmental information, integration of this information with previous knowledge to form a coherent mental picture, and the use of that picture in directing further perception and anticipating future events.”Footnote 27 Shared situational awarenessFootnote 28,Footnote 29 between the pilots of a crew depends on the extent to which the respective situational awareness of each pilot is similar. Crew members who have a shared situational awareness can anticipate and coordinate their actions and therefore act with cohesion and efficiency.
Pilots work in a complex environment that requires monitoring multiple sources and types of information. It has been shown that several cognitive biases, including the following, affect how information is interpreted and heeded in complex environments:
- Plan continuation bias, which is a form of confirmation bias, is described as a “deep-rooted tendency of individuals to continue their original plan of action even when changing circumstances require a new plan.”Footnote 30 Once a plan has been established and put into action, it becomes more difficult to recognize stimuli or conditions in the environment that may be cues for change than it is when no plan has been established. To recognize that a change of plan is needed and to react in time, a pilot must perceive the condition or stimulus as important enough to warrant immediate action. Plan continuation bias becomes even stronger when the task (e.g. a landing) is on the verge of being completed.
- People have a limited capacity to focus their attention and process information. As a result, they may fall into the trap of “attentional narrowing” or tunnelling. They focus on certain cues in the environment, which they attempt to process, intentionally or unintentionally diverting their attention from other cues or tasks. For example, pilots in high workload conditions may focus on certain indicators to the detriment of others.Footnote 31
- Workload depends on the number of tasks to be completed within a certain period. If the number of tasks to be completed increases, or if the time available decreases, the workload rises. Task saturation occurs when the number of tasks to be completed within a certain period exceeds pilots’ capacity to complete them, and some tasks are missed or delayed.
1.18.1.2 Mental models
A mental model is an internal structure that enables people to describe, explain, and predict events and situations in their environment.Footnote 32 When a mental model is adopted, it is resistant to change. New convincing information must be assimilated in order to change the mental model. An inaccurate mental model will interfere with the perception of critical elements or the comprehension of their importance.Footnote 33
1.18.1.3 Crew resource management
CRM is the effective use of all available resources—human, hardware and information—to conduct flights safely and efficiently.Footnote 34 CRM includes skills, abilities, attitudes, communication, situational awareness, problem solving, and teamwork. CRM is linked to the cognitive abilities and interpersonal skills required to manage a flight. These cognitive abilities include the mental processes needed to establish and maintain accurate situational awareness, solve problems, and make decisions. Interpersonal skills are linked to communications and behaviours associated with teamwork. Effective risk management in the cockpit is intrinsically linked to effective CRM.
1.18.1.4 Authority gradient
Authority gradient refers to the decision-making hierarchy between the captain and the FO. This gradient is characterized by several factors, including each person’s experience. A strong authority gradient may be a barrier to the decision-making dynamics of a crew and may discourage the FO from expressing disagreement due to their experience. In this occurrence, the captain had accumulated 2867 flight hours on type, and the FO had 280 flight hours on type. The 2 pilots had been paired up in the past with no issues reported.
1.18.1.5 Escalation of assertiveness by first officers
Assertiveness can be defined as the ability to express one’s opinions in a calm and firm manner and to not accept what appears to be incorrect. Escalation can be progressive or immediate depending on the severity of the threat. An example of a CRM communication tool is the Probing, Alerting, Challenging and Emergency Warning (PACE) model.Footnote 35 The PACE model provides pilots, especially FOs, with a series of communication strategies designed to allow for a natural escalation of assertiveness, depending on the circumstances at the time.Footnote 36
1.18.2 Airspeed limitation according to the Canadian Aviation Regulations
According to the CARs, no person shall
(b) operate an aircraft at an indicated airspeed of more than 200 knots if the aircraft is below 3,000 feet AGL within 10 nautical miles of a controlled aerodrome unless authorized to do so in an air traffic control clearance.Footnote 37
Furthermore, the CARs define a controlled aerodrome as “an aerodrome at which an air traffic control unit is in operation.”Footnote 38 The CARs also define an air traffic control unit (ATC unit) as follows:
- (a) an area control centre established to provide air traffic control service to IFR aircraft,
- (b) a terminal control unit established to provide air traffic control service to IFR aircraft while they are being operated within a terminal control area, or
- (c) an air traffic control tower established to provide air traffic control service at an aerodrome.Footnote 39
The interpretation becomes ambiguous when an aerodrome such as CYZV, which does not have an air traffic control tower, is located in Class E controlled airspace, where separation between IFR aircraft is provided by the area control centre.Footnote 40 To clarify this ambiguity, a request for interpretation was sent to TCCA.
Finding: Other
According to TCCA’s interpretation, CYZV is an uncontrolled airport because it does not have a control tower. As a result, the airspeed limitation of 200 knots stipulated in paragraph 602.32(1)(b) of the CARs does not apply.
1.18.3 Hydroplaning
Hydroplaning, also known as “aquaplaning,” occurs when a film of water forms between the airplane’s tires and the runway surface, causing a loss of traction and preventing the airplane from responding to control inputs such as steering and braking.
Reverted-rubber hydroplaning
can occur when a locked tire skids on a wet or icy runway. Frictional heating raises the tire temperature causing rubber particles to shred off the tread. These particles accumulate behind the tire, forming a dam that blocks the escape of water. The trapped water heats and turns to steam. The steam pressure lifts the tire from the surface. Footnote 41
1.18.4 Lightweight data recorders and flight data monitoring
For decades, operators of multi-engine turbine-powered aircraft defined in subsection 605.33(1) of the CARs Footnote 42 that are used to transport passengers have been required to equip their aircraft with flight data recorders. These operators can use the data for their internal flight data monitoring (FDM) and flight operations quality assurance programs. These programs help air operators with preventive safety management. Also, just having a lightweight data recorder (LDR) on board can positively influence pilot behaviour.
The development of LDRs offers the possibility to extend flight monitoring to smaller operators. Through this technology and FDM, these operators are able to oversee pilot decision making as well as compliance with SOPs and operational limitations. The CARs do not currently require the installation of an LDR on board aircraft.
On several occasions, TSB air transportation safety investigation reports Footnote 43 have pointed to the potential for LDRs and FDM to help operators proactively detect safety deficiencies before they cause an accident. In addition, the TSB has issued 2 recommendations related to LDRs and FDM (see Section 1.18.6 TSB recommendations).
1.18.5 Initiatives related to runway overruns
Runway overruns are an international concern. They have been studied by various agencies, organizations, and manufacturers to determine what is preventing an aircraft from stopping on the runway and to identify factors that might mitigate the risk of such an event occurring.
1.18.5.1 Risk factors
The Flight Safety Foundation (FSF) analyzed the data on runway overruns that had occurred over a period of 14 years, and determined that “the risk of a runway excursion increases when more than one risk factor is present. Multiple risk factors create a synergistic effect (i.e., two risk factors more than double the risk).”Footnote 44
To provide “ways for pilots and airplane operators to identify, understand, and mitigate risks associated with runway overruns during the landing phase of flight,”Footnote 45 the U.S. Federal Aviation Administration (FAA) published Advisory Circular (AC) 91-79A in 2014 (amended in 2018). The AC indicates the following:
A study of FAA and NTSB [U.S. National Transportation Safety Board] data indicates that the following hazards increase the risk of a runway overrun:
- Unstabilized approach[*];
- High airport elevation or high Density Altitude (DA), resulting in increased groundspeed;
- Effect of excess airspeed over the runway threshold[*];
- Airplane landing weight;
- Landing beyond the touchdown point[*];
- Downhill runway slope;
- Excessive height over the runway threshold[*];
- Delayed use of deceleration devices[*];
- Landing with a tailwind[*]; and
- A wet or contaminated runway.[*Footnote 46],Footnote 47
The FAA proposes a strategy that incorporates both theoretical and practical training on runway overrun risk factors to improve pilot recognition of higher-risk landing operations.Footnote 48
In the same circular, the FAA states that “[a]dhering to the SOPs and best practices for stabilized approaches will always be the first line of defense in preventing a runway overrun.”Footnote 49
1.18.5.2 Standard operating procedures
SOPs, including standard calls and checklists, are vital sources of information that provide pilots with guidelines on general use of the aircraft. They assist pilots with decision making and coordination between crew members.
To reduce the risk of approach and landing accidents, the International Civil Aviation Organization (ICAO), the FSF, the FAA, the NTSB, TCCA and the TSB have all, on numerous occasions, stressed the importance of having clear, complete, precise, and unambiguous SOPs, and the need to comply with SOPs during critical phases of flight.Footnote 50 Furthermore, from 1994 to 2022, inconsistent or missing procedures were identified in 39 (various) findings in TSB air transportation safety investigation reports.Footnote 51 The deficiencies identified were mainly associated with an absence of specific guidelines and discrepancies in procedures.
1.18.5.3 Stabilized approaches
As established in previous investigations conducted by the TSBFootnote 52 and by organizations in other countries, unstable approaches pose a high risk to flight operations, including the risk of a runway overrun.Footnote 53
1.18.5.4 On-board runway overrun awareness and alerting systems
New technological defences are now available. On-board runway overrun awareness and alerting systems (ROAAS) developed for aircraft can help reduce the number of runway overruns, particularly during landing. These systems send visual and aural alerts to pilots before touchdown if conditions indicate that landing cannot be completed within the available landing distance for the intended runway. The systems can even monitor conditions after touchdown if braking is not as effective as anticipated.Footnote 54
ROAASs have not yet been widely adopted by Canadian operators; however, some operators have informed the TSB that they are planning to install such systems in the coming years. ROAASs are not currently installed in Airmedic aircraft, and are not required by regulations.
1.18.6 TSB recommendations
On 14 May 2013, the Board issued Recommendation A13-01, which recommended that
the Department of Transport work with industry to remove obstacles to and develop recommended practices for the implementation of flight data monitoring and the installation of lightweight flight recording systems by commercial operators not currently required to carry these systems.
TSB Recommendation A13-01
On 26 April 2018, the Board replaced Recommendation A13-01 with Recommendation A18-01, which recommended that
the Department of Transport require the mandatory installation of lightweight flight recording systems by commercial operators and private operators not currently required to carry these systems.
TSB Recommendation A18-01
In its most recent response in January 2023, Transport Canada (TC) indicated that it agrees in principle with the recommendation.
Following the 2021 publication of the Notice of Proposed Amendment (NPA) on LDRs, TC received significant industry input and comments that resulted in a re-assessment of the approach and scope of the LDR requirements. TC is developing a new and revised NPA, which is planned to be published in 2023 for consultation. The revision of the NPA and additional consultation will delay the timelines for regulatory implementation as detailed in TC’s Forward Regulatory Plan.
The Board is encouraged by TC’s continued efforts to require that existing aircraft be retrofitted with LDRs and that LDRs be installed on newly manufactured aircraft. However, the Board is concerned by the potential re-scoping of the LDR requirements and further delays. Until the revised NPA is available for review, it is unclear if the previously proposed requirements will be preserved.
Therefore, the Board is unable to assess the response to Recommendation A18-01.Footnote 55
1.18.7 TSB Watchlist
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada’s transportation system even safer.
Runway overruns have been on the TSB Watchlist since 2010. From 01 January 2005 to 30 June 2022, there were on average 9.3 runway overrun occurrences per year at Canadian airports. Of these occurrences, 6.7 occurred during landing. Although the number of runway overruns varies from year to year, there is no statistically significant trend.Footnote 56
Runway 09 at CYZV does not have a runway end safety area (RESA), nor is one required by existing regulations. Before initiating the turn, the occurrence aircraft travelled approximately 600 feet in the clearway without being damaged. This occurrence shows the importance of the ground, the terrain, and the absence of obstacles beyond the end of the runway to reduce the adverse consequences of a runway overrun.
ACTION REQUIRED Despite the actions taken to date, the number of runway overruns in Canada has remained constant since 2005 and demands a concerted effort to be reduced. The issue of runway overruns will remain on the TSB Watchlist until
|
An SMS is an internationally recognized framework that helps companies identify hazards, manage risks, and make operations safer—ideally before an accident occurs. Although the issue of safety management has been on the Watchlist since 2010 and industry awareness about SMSs has slowly increased since then, TSB investigation reports continue to identify deficiencies and concerns in 3 transportation sectors.
Given that the regulations do not require air-taxi operators to have an SMS in place, TCCA did not assess or oversee the effectiveness of the SMS Airmedic put in place voluntarily.
ACTION REQUIRED The issue of safety management will remain on the Watchlist for the air transportation sector until
|
2.0 Analysis
There was no indication of an airframe, engine, or system failure during the occurrence flight. Aircraft performance was also not a contributing factor in this occurrence. The flight crew members held the appropriate licences and ratings for the flight in accordance with existing regulations, and there was no indication that their performance was degraded by physiological factors such as fatigue. Therefore, the analysis will focus on the decision to conduct and continue the high-speed approach down to 500 feet above ground level (AGL), the decision to continue the landing, and lastly, initiatives related to runway overruns.
2.1 Decision to conduct a high-speed final approach
During the approach briefing before the descent from flight level 270, the captain told the first officer (FO) that he was going to show him that the Pilatus PC-12 was able to perform a late descent at a rate of descent of approximately 3000 fpm. The automatic terminal information service message for the Sept-Îles Airport indicated visual flight conditions, moderate rain showers, and winds from the west at 8 knots, gusting to 15 knots. These conditions were favourable for a landing on Runway 27; however, the captain told the FO that he was going to conduct a straight-in approach for Runway 09 via the ETBAR initial approach waypoint, and a landing with the flaps set to 15°, with a landing reference speed (Vref) of 95 knots.
The airplane crossed the ETBAR waypoint at approximately 250 feet above the 3° approach slope at 213 knots indicated airspeed (KIAS). The crew had Runway 09 in sight, and the captain decided to accelerate to conduct a high-speed final approach, decelerating just before reaching the runway. However, given that he believed that the airspeed limit of 210 knots published on the approach chart for the IGSUK and VOKON waypoints also applied to the straight-in approach via ETBAR, he asked the FO to cancel the instrument flight rules (IFR) flight plan. The captain then increased power without consulting the FO. The aircraft’s speed reached the maximum operating speed (Vmo) of 240 KIAS. The FO called out high speed. The captain reduced power to stabilize the speed at approximately 230 KIAS. At that point, the FO expressed his discomfort with the high speed. However, the captain confirmed that he was continuing the high-speed approach. The aircraft was then 3 nautical miles (NM) from the runway at 1000 feet AGL (stabilized approach gate according to the standard operating procedures [SOPs]) in clean configuration at an airspeed of 236 KIAS.
A few months before the occurrence, a similar high-speed final approach had been conducted by another crew, and the deceleration with a rapid descent close to the runway had resulted in a passenger complaint. The company had reprimanded the pilot involved and issued a memorandum to crews to formally notify them that these manoeuvres were inappropriate and should not be conducted.
The decision to conduct a high-speed final approach, despite the company’s instructions to the contrary, was likely influenced by the fact that there were no passengers on board and by the fact that the crew was unaware of the engine condition trend monitoring (ECTM) system’s actual recording abilities. Therefore, the crew most likely assumed that the company’s management team would not be aware of the deviations from the SOPs and that there would be no risk of administrative penalties.
Finding as to causes and contributing factors
During the occurrence flight, the captain, who was paired with an FO with little experience on the Pilatus PC-12, decided to demonstrate a high-speed final approach, decelerating just before reaching the runway. As a result, the stabilized approach gate indicated in the SOPs (1000 feet AGL) was crossed in clean configuration at an airspeed of 236 KIAS.
2.2 Stabilized approach gate
When the aircraft crossed the stabilized approach gate indicated in the SOPs, it could still reach the runway threshold at 50 feet AGL at a Vref of 95 knots, in a landing configuration with flaps set to 15°, by decelerating in a climb, then descending at a high rate before reaching the runway threshold.
According to calculations made using data from the aircraft manufacturer, the normal landing distance Footnote 57 is 2945 feet with the flaps set to 15° and in the conditions of the occurrence flight. This landing distance includes 1707 feet for the landing roll with average braking conditions and no reverse thrust.
Knowing that he could land on short runways with the Pilatus PC-12, and having the runway in sight, the captain was confident that he could land within the first ⅓ of the runway (first 2184 feet) and, therefore, believed that he had more than 4300 feet of runway for the landing roll. The captain was convinced that he could stop on the wet runway, despite the tailwind.
2.3 Authority gradient and assertiveness
When the aircraft was approximately 6 NM from the runway, it was flying at an airspeed of 230 KIAS. The FO expressed his doubts that the landing would be successful, and the captain confirmed his intention to continue the high-speed approach. However, given that the captain had not communicated to the FO his intention to deviate from the SOPs—neither for the configuration at 1000 feet AGL, nor for the deceleration and aircraft configuration before reaching the runway threshold—it is likely that the FO had a different understanding of the situation. Therefore, the 2 pilots no longer had a shared situational awareness of the approach that was being executed outside of SOP-defined parameters, or of the upcoming manoeuvre to conduct the landing as described in the briefing, i.e., at a Vref of 95 KIAS with the flaps set to 15°.
The 2 pilots knew each other well, but given that the captain had 3 times more total flying experience than the FO and 10 times more flying experience on the Pilatus PC-12, the authority gradient was high for flying experience on the Pilatus PC-12. During the approach, the FO voiced his discomfort, and then his doubt about a successful landing. However, his communications were not actionable, as is the case with a go-around call. The FO felt he did not have enough experience to shift from a passive advisory role to strong enough assertiveness to convince the captain to conduct a go-around.
Finding as to causes and contributing factors
During the high-speed approach, the FO had doubts that the aircraft could land successfully; however, due to the authority gradient, he deferred to the captain’s experience and did not feel comfortable making the actionable go-around call.
2.4 Continuation of the high-speed approach
After crossing 1000 feet AGL, the high-speed (236 KIAS) approach continued for 17 seconds, until the aircraft crossed 500 feet AGL (238 KIAS) at approximately 1.7 NM from the runway. During those 17 seconds, the captain, who was focused on the approach, likely experienced attentional narrowing, hindering him from having full awareness of the speed so close to the runway.
One second later, the airspeed exceeded the Vmo of 240 KIAS and the captain immediately reduced the power to minimum. Four seconds after the reduction in power, the captain initiated a climb to reduce speed more quickly. Despite this manoeuvre, the aircraft was 28 seconds from the runway threshold, while the theoretical deceleration time required to reach the Vref of 95 knots was 35 seconds. As a result, it was no longer possible to slow the aircraft, configure it for landing, and reach the Vref of 95 KIAS, while at the same time descending to cross the runway threshold at 50 feet AGL. However, perceiving that it was still possible to land within the first ⅓ of the runway, the captain continued with the approach.
Finding as to causes and contributing factors
When the aircraft was approximately 1.7 NM from the runway, flying at an airspeed of 238 KIAS at 500 feet AGL, it was no longer possible to decelerate and continue the descent to reach the runway threshold at 50 feet AGL in a stabilized landing configuration at the Vref of 95 KIAS. However, perceiving that it was still possible to land within the first ⅓ of the runway, the captain continued with the approach.
2.5 Decision to land
Generally, a high workload tends to cause attentional narrowing. Under these circumstances, some tasks may be missed or not performed in the right order, and some critical information may not be captured or taken into account.
Given the aircraft’s high speed when it was approximately 1.7 NM from the runway at 500 feet AGL, the pilots had very little time to perform the tasks required to decelerate and configure the aircraft before landing. This high workload so close to the runway influenced the decision not to respect the airspeed limit for extending the landing gear, and to ignore the effect that the tailwind component combined with high speed can have when braking on a wet runway. In addition, given that the captain had created a mental model in which it was possible to land within the first ⅓ of the runway, his perception and understanding of the critical elements may have been clouded.
During the deceleration manoeuvre, the captain made the “gear down” call at approximately 195 KIAS, and the FO called out high speed, given that the maximum landing gear operating speed was 180 KIAS. The captain, focused on performing the tasks required for the landing, requested “gear down” again, thereby confirming to the FO his intention to land. Although the FO felt uncomfortable with the idea of continuing the approach and landing, he chose not to contradict the captain at this critical moment of flight, 0.5 NM from the runway threshold. He selected the landing gear extension at 188 knots. This action by the FO may have been interpreted by the captain as a validation of his decision. It should be noted that, at the time, the FO had very little time to analyze the situation and the options. The indication that the landing gear was extended and locked came only 7 seconds before the aircraft touched down on the runway.
Even if it had been possible to conduct a go-around without too much difficulty before reaching the runway threshold, the go-around would have resulted in the flight service specialist submitting an aviation occurrence report and, very likely, the company following up with the pilots regarding the circumstances leading up to the go-around.
Given that the captain had already faced administrative penalties from the company for previous incidents, he may have reasonably believed that he would be facing new administrative and disciplinary measures if the company learned that he had conducted this high-speed approach, deviating substantially from the SOPs. It is therefore likely that this situation influenced his decision to continue with the approach to avoid an occurrence report being filed for a go-around.
Finding as to causes and contributing factors
When the aircraft was approximately 0.5 NM from the runway at 500 feet AGL, the captain was focused on conducting the landing within the first ⅓ of the runway, and insisted on the landing gear being extended even though the aircraft’s speed exceeded the maximum landing gear operating speed at the time. The FO followed the order, and the landing gear was extended, which allowed the landing to continue .
According to the SOPs (before-landing checklist), the pilot flying calls “gear down, landing checks, flaps 15” when the airspeed is 170 KIAS or less and decreasing. In the occurrence flight, since the airspeed was approximately 185 KIAS after gear down was selected and the maximum speed with flaps extended was 165 KIAS, the FO asked the captain whether he should extend the flaps to 15°. The captain replied that the landing would be conducted without flaps. This decision was strategic within the context of his intention to land within the first ⅓ of the runway. However, landing without flaps increases the ground roll distance by approximately 680 feet on a dry runway, and only if the speed is stabilized at a Vref of 115 KIAS without flaps.
The aircraft crossed the runway threshold at 200 feet AGL, at 180 KIAS (ground speed of 191 knots), with a rate of descent of 2000 fpm, the landing gear was in transit, and the flaps were in the fully retracted position. In such a situation, even if the pilot manages the flight path for a landing within the first ⅓ of the runway, the aircraft has excessive vertical and horizontal speeds. To recognize that a change of plan is needed and to react in time, a pilot must perceive the condition or stimulus as important enough to warrant immediate action. Plan continuation bias becomes even stronger when a goal is on the verge of being achieved.
According to calculations when the aircraft crossed the runway threshold, with maximum braking on a dry runway, and no reverse thrust or flaps, the landing distance was 7170 feet, exceeding the length of the runway, which was 6552 feet. Alternatively, maximum reverse thrust provided a theoretical margin of 157 feet. However, the runway was wet.
Finding as to causes and contributing factors
The aircraft crossed the runway threshold at 200 feet AGL at an airspeed of 180 KIAS, with a rate of descent of 2000 fpm, the landing gear in transit, and the flaps in the fully retracted position. Under such conditions, it was impossible to stop the aircraft on the wet runway. However, the captain continued the approach, influenced by plan continuation bias and focused on conducting the landing within the first ⅓ of the runway .
2.6 Landing and runway overrun
Runway conditions were not available at the time of the approach. However, the crew observed that the runway was wet. The tire inspection conducted after the flight found marks which confirmed that reverted-rubber hydroplaning had occurred while the aircraft was braking on the runway. Given that braking distance increases with hydroplaning, it is reasonable to conclude that the increase in braking distance on the wet runway exceeded the theoretical margin of 157 feet available for a landing on a dry runway with maximum reverse thrust.
The touchdown was relatively smooth, occurring approximately 2525 feet beyond the runway threshold, at 159 KIAS (ground speed of 167 knots). The brakes were then applied forcefully and reverse thrust was applied in the usual way (i.e. in idle reverse). The pilot did not use maximum reverse thrust and had never done so in the past. While braking, with the aircraft hydroplaning, the runway overrun was inevitable. Therefore, the usual use of reverse thrust was only a further contributing factor to the runway overrun. In reality, it only influenced the speed at which the airplane left the end of the runway and the distance travelled in the clearway.
The captain was focused on braking and maintaining lateral control of the aircraft on the wet runway and, therefore, did not immediately perceive that the runway overrun was likely. Fifteen seconds after touchdown, at approximately 750 feet from the end of the runway, when the crew realized that an overrun was imminent, the captain increased reverse thrust. Six seconds later, the aircraft overran the runway at a ground speed of 57 knots.
Finding as to causes and contributing factors
The aircraft landed on the runway approximately 2525 feet from the threshold at 159 KIAS, i.e., a ground speed of 167 knots. Given that the excessive speed, combined with other factors, increased the landing distance, the aircraft overran the runway 21 seconds later, at a ground speed of 57 knots.
The flight data were compared with the data obtained during the certification flights conducted on a dry runway. The rate of deceleration obtained during the occurrence flight on the wet runway, with braking and usual use of reverse thrust (idle reverse), was slightly higher than the rates of deceleration obtained during the certification flight tests, with maximum braking and no reverse thrust. Before initiating the turn, the aircraft travelled approximately 600 feet in the clearway, which represents a landing distance of approximately 7142 feet. This landing distance is similar to the manufacturer’s estimated landing distance of 7170 feet on a dry runway with maximum braking and no reverse thrust. It is therefore possible to conclude that usual use of reverse thrust (idle reverse) only offset the effects of hydroplaning.
2.7 Cockpit voice recorder
During this high-speed approach, it was possible to arrive at the stabilized approach gate indicated in the SOPs at 1000 feet AGL, with a planned deceleration of about 35 seconds. Then, even if it was no longer possible to comply with the SOPs, it was still possible to begin decelerating and cross the runway threshold on the slope at 50 feet AGL, in a landing configuration at a Vref of 95 KIAS. However, the high-speed approach continued to the point where it was no longer possible to stop the aircraft on the runway.
Given that there was no cockpit voice recorder, the investigation was unable to clearly establish the 2 pilots’ activities and communications or to accurately assess the context in which the high-speed approach continued.
Finding as to risk
If cockpit voice recordings are not available to TSB investigators, it is impossible to accurately assess the pilot’s decision making, crew resource management, workload management, and SOP execution and compliance, which may limit the identification of safety deficiencies and the advancement of flight safety.
2.8 Initiatives related to runway overruns
Runway overruns have been on the TSB Watchlist since 2010 and despite the actions taken to date, the number of runway overruns in Canada has remained constant since 2005. A concerted effort is needed to reduce this number. As part of this effort, aids are now available to increase pilot situational awareness before and on the runway. Examples include on-board runway overrun awareness and alerting systems (ROAAS) for aircraft, and visual cues on the runway at certain airports. These aids show the remaining runway length and can help pilots decide on the optimal use of deceleration devices. However, these aids are not required by regulations and are not yet in widespread use.
Various agencies, organizations, and manufacturers recognize that there are generally several risk factors involved in runway overruns. The Flight Safety Foundation (FSF) determined that multiple risk factors create a synergistic effect, and that 2 risk factors more than double the risk. Of the 10 factors that increase the risk of a runway overrun, published in the U.S. Federal Aviation Administration’s (FAA’s) Advisory Circular (AC) 91-79A, 7 were present when the occurrence aircraft was landing. Although the captain was aware that the runway was wet and that there was a tailwind, he did not consider the other factors or the combination of all the factors that were present.
The FAA proposes a strategy that incorporates both theoretical and practical training to improve recognition of higher-risk landings. The pilots had not received specific training on runway overrun risk factors, and the regulations do not require it for Canadian Aviation Regulations (CARs) Subpart 703 operators.
Finding as to risk
If SOPs and training do not incorporate runway overrun risk factors, these risk factors may not be taken into consideration during approach, thereby increasing the risk of a runway overrun.
2.8.1 Stabilized approaches
In AC 91-79A, the FAA states that “[a]dhering to the SOPs and best practices for stabilized approaches will always be the first line of defense in preventing a runway overrun.” Footnote 58 For its part, Transport Canada Civil Aviation (TCCA) states that “[w]ith such significant weightage placed on the SOP it is incumbent on TCCA to review the operator’s SOP for quality, consistency, accuracy, conciseness, clarity, relevancy and content.” Footnote 59
Interpreting ambiguities and contradictions found in SOPs is not unique to the occurrence flight. From 1994 to 2022, inconsistent or missing procedures were identified in 39 (various) findings in TSB air transportation safety investigation reports. In many cases, the procedures had been reviewed by TCCA and no irregularities had been identified. These inconsistencies and deficiencies give pilots an opportunity to interpret certain situations, at times reducing the safety margins.
Airmédic Inc.’s (Airmedic’s) flight operations manual does not contain a general policy on the requirement to conduct stabilized approaches or to conduct a go-around if the approach is unstable. Airmedic’s SOPs do define the stabilized approach criteria, the calls required in the event of a deviation (speed margins and rate of descent), as well as the point where the approach “should” be stabilized. The SOPs are also clear enough regarding visual approaches: the aircraft “must be” configured for landing and the before-landing checklist “must be” completed before reaching 1000 feet AGL. However, the use of the word “should” when the approach is not stabilized may give the impression that it is a suggestion rather than a formal directive, and that continuing with the approach is at the captain’s discretion. Hence, believing that there is no formal obligation to conduct a go-around, pilots may rely on their experience and assessment of the situation at hand to determine whether a successful landing is still possible. In the occurrence flight, the captain was convinced that he could successfully land within the first ⅓ of the runway, and continued with the approach and landing.
Airmedic’s SOPs were reviewed by TCCA, which verified that topics required by the regulations were covered, and issued a letter of compliance to the company. However, TCCA did not check the quality, consistency, accuracy, conciseness, clarity, and relevance of the SOPs.
Finding as to risk
If TCCA does not assess the quality, consistency, accuracy, conciseness, clarity, and relevance of an operator’s SOPs, these procedures may not be effective, increasing the risks to flight operations.
The reactive process inspection (PI) conducted by TCCA after the occurrence resulted in an observation regarding the wording of the SOPs, which [translation] “do not provide standard calls at specific altitudes to determine whether or not stabilization criteria [read: stabilized approach criteria] are met” and which could [translation] “lead crew members to believe that they have discretion in applying stabilization criteria.” Footnote 60 To avoid a situation similar to that of the occurrence flight, some operators include an actionable go-around call in their SOPs if approach criteria are not met at the stabilized approach gate or later.
The captain of the occurrence flight, who had a high workload, was focused on the manoeuvre to be executed and was still convinced that it was possible to land successfully, was unable to take into consideration all of the runway overrun risk factors. At that point, the FO had doubts that the aircraft could land successfully after this unstable approach, but he did not have enough time to discuss the matter and convince the captain to conduct a go-around. Therefore, an actionable go-around call was the only solution to stop the landing after an unstable approach.
Finding as to risk
If SOPs do not include mandatory and actionable go-around calls when approaches become unstable, pilots may choose to continue with an unstable approach, increasing the risk of a runway overrun.
2.8.2 Management of higher-risk approaches
In August 2021, following a similar incident that took place a few months before this occurrence, the company had taken action to prevent this type of high-speed approach from happening again. However, in light of the occurrence flight, these actions did not prevent a repetition of this type of approach.
2.8.3 Lightweight data recorders and flight data monitoring
Airmedic airplanes are equipped with a system that records certain flight data that are used for engine condition monitoring. However, the airplanes are not equipped with lightweight data recorders (LDRs), nor are they required to be by regulation. Just having an LDR on board can positively influence pilot behaviour. Flight data monitoring (FDM) provides the possibility of overseeing flight operations, i.e., checking compliance with company procedures and operational limits, and identifying high-risk manoeuvres so that corrective action can be taken before an accident occurs.
For decades, operators of multi-engine turbine-powered aircraft that are used to transport passengers have been using FDM systems for preventive safety management. On several occasions, TSB air transportation safety investigation reports have highlighted the potential of LDRs and FDM systems to help other operators proactively detect safety deficiencies before they cause an accident. In addition, the TSB has issued 2 recommendations related to the implementation of FDM and the installation of LDRs.
Transport Canada (TC) has indicated that it agrees in principle with these recommendations and, in 2021, it published a Notice of Proposed Amendment (NPA) on LDRs. Following this publication, TC received significant industry input and comments that resulted in a re-assessment of the approach and scope of the LDR requirements. A new and revised NPA is planned to be published in 2023. The revision of the NPA and additional consultation will delay the timelines for regulatory implementation as detailed in TC’s Forward Regulatory Plan. Until the revised NPA is available for review, it is unclear if the previously proposed requirements will be preserved. However, within the context of proactively managing operational hazards, operators could take action without waiting to be forced to do so by regulations.
As seen in this occurrence, Airmedic has access to certain data when a parameter exceedance is detected. However, the company does not have access to data in other cases and cannot follow up, if needed.
Finding as to risk
If operators do not have LDRs and FDM systems, they may not be able to oversee compliance with policies, procedures and operational limits, increasing the risk that discrepancies or unsafe practices will go undetected and continue happening.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- During the occurrence flight, the captain, who was paired with a first officer with little experience on the Pilatus PC-12, decided to demonstrate a high-speed final approach, decelerating just before reaching the runway. As a result, the stabilized approach gate indicated in the standard operating procedures (1000 feet above ground level) was crossed in clean configuration at 236 knots indicated airspeed.
- During the high-speed approach, the first officer had doubts that the aircraft could land successfully; however, due to the authority gradient, he deferred to the captain’s experience and did not feel comfortable making the actionable go-around call.
- When the aircraft was approximately 1.7 nautical miles from the runway, flying at an airspeed of 238 knots indicated airspeed at 500 feet above ground level, it was no longer possible to decelerate and continue the descent to reach the runway threshold at 50 feet above ground level in a stabilized landing configuration at the landing reference speed of 95 knots indicated airspeed. However, perceiving that it was still possible to land within the first third of the runway, the captain continued with the approach.
- When the aircraft was approximately 0.5 nautical miles from the runway at 500 feet above ground level, the captain was focused on conducting the landing within the first third of the runway, and insisted on the landing gear being extended even though the aircraft’s speed exceeded the maximum landing gear operating speed at the time. The first officer followed the order, and the landing gear was extended, which allowed the landing to continue.
- The aircraft crossed the runway threshold at 200 feet above ground level at 180 knots indicated airspeed, with a rate of descent of 2000 fpm, the landing gear in transit and the flaps in the fully retracted position. Under such conditions, it was impossible to stop the aircraft on the wet runway. However, the captain continued the approach, influenced by plan continuation bias and focused on conducting the landing within the first third of the runway.
- The aircraft landed on the runway approximately 2525 feet from the threshold at 159 knots indicated airspeed, i.e., a ground speed of 167 knots. Given that the excessive speed, combined with other factors, increased the landing distance, the aircraft overran the runway 21 seconds later, at a ground speed of 57 knots.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If cockpit voice recordings are not available to TSB investigators, it is impossible to accurately assess the pilot’s decision making, crew resource management, workload management, and standard operating procedure execution and compliance, which may limit the identification of safety deficiencies and the advancement of flight safety.
- If standard operating procedures and training do not incorporate runway overrun risk factors, these risk factors may not be taken into consideration during approach, thereby increasing the risk of a runway overrun.
- If Transport Canada Civil Aviation does not assess the quality, consistency, accuracy, conciseness, clarity, and relevance of an operator’s standard operating procedures, these procedures may not be effective, increasing the risks to flight operations.
- If standard operating procedures do not include mandatory and actionable go-around calls when approaches become unstable, pilots may choose to continue with an unstable approach, increasing the risk of a runway overrun.
- If operators do not have lightweight data recorders and flight data monitoring systems, they may not be able to oversee compliance with policies, procedures and operational limits, increasing the risk that discrepancies or unsafe practices will go undetected and continue happening.
3.3 Other findings
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- According to Transport Canada Civil Aviation’s interpretation, the Sept-Îles Airport is an uncontrolled airport because it does not have a control tower. As a result, the airspeed limitation of 200 knots stipulated in paragraph 602.32(1)(b) of the Canadian Aviation Regulations does not apply.
4.0 Safety action
4.1 Safety action taken
4.1.1 Airmédic Inc.
Following the occurrence, Airmédic Inc. amended its standard operating procedures to reduce ambiguities and respond to observations made by Transport Canada Civil Aviation during its reactive process inspection.
4.1.2 Sept-Îles Airport
- After the occurrence, the following actions were taken:
- A procedure was put in place so that pilots are notified when there is more than ⅛ inch of rain or standing water on the runway.
- Daily inspection records now include runway condition checks.
- Airport staff are now present for all commercial flights based on the flight schedule in effect.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Sept-Îles Airport approach chart

NOT FOR NAVIGATION
Source: NAV CANADA, Canada Air Pilot (CAP), CAP 5: Quebec, effective 12 August 2021 to 07 October 2021.
Appendix B – Significant events
| Local time | Distance from threshold | Altitude (feet ASL) | Airspeed (KIAS) | Event |
|---|---|---|---|---|
| 1600:00 | N/A | N/A | N/A | Takeoff from Québec/Jean Lesage International Airport |
| 1657:21 | – | 25 291 | 191 | Descending |
| 1705:26 | 14.5 NM | 5078 | 213 | ETBAR (published altitude 4820 ft ASL) |
| 1705:50 | – | 4500 | 213 | IFR flight plan cancelled |
| 1706:00 | 13 NM | 4265 | 217 | Power increased |
| 1706:32 | 10 NM | 3477 | 240* | Vmo alert/power reduced |
| 1706:34 | – | – | 240* | – |
| 1707:33 | 5.6 NM | 2020 | 233 | DENEZ (published altitude 2000 ft ASL) |
| 1708:08 | 3.0 NM | 1173 | 236 | 1000 ft AGL; indicated airspeed: 236 knots |
| 1708:10 | – | 1121 | 236 | Position report 4 miles on final |
| 1708:25 | 1.7 NM | 684 | 238 | 500 ft AGL (1st time) |
| 1708:26 | – | 661 | 241* | Overspeed in relation to Vmo |
| 1708:27 | – | 633 | 244* | Reduction to minimum power |
| 1708:28 | 1.6 NM | 611 | 242 | XOXUM (published altitude 730 ft ASL) |
| 1708:31 | – | 592 | 232 | Altitude increased (to slow down) |
| 1708:43 | 0.6 NM | 670 | 192 | 500 ft AGL (2nd time) |
| 1708:44 | – | 651 | 188** | Selection of landing gear extension; overspeed |
| 1708:53 | 0 | 368 | 180** | Runway threshold crossed: 200 ft AGL; ground speed 191 knots |
| 1708:55 | – | 301 | 182** | End of overspeed for landing gear |
| 1708:56 | – | 271 | 177 | Landing gear extended and locked |
| 1709:01 | +2250 ft | – | 164 | Landing; ground speed: 170 knots |
| 1709:02 | +2525 ft | – | 159*** | Landing; ground speed: 167 knots |
| 1709:03 | +2800 ft | – | 157 | Landing; ground speed: 164 knots |
| 1709:17 | +5802 ft | – | 77 | Reverse thrust increased |
| 1709:23 | +6552 ft | – | 53 | End of Runway 09; ground speed: 57 knots |
| 1709:33 | +7142 ft | – | 11 | Beginning of right turn around an approach light (590 ft from end of runway) |
| 1709:42 | +7192 ft | – | 12 | Furthest position from end of runway (640 ft from end of runway) |
* Overspeed in relation to the Vmo.
** Overspeed in relation to the maximum speed with flaps extended.
*** According to the limited data available, it is estimated that touchdown occurred between 1709:01 and 1709:03. Although it was impossible to determine the exact time with certainty, for all practical purposes, it is more likely that the touchdown occurred in the middle of this period rather than at the beginning or end. Therefore, to simplify the report, touchdown is presumed to have occurred at 1709:02, approximately 2525 feet beyond the runway threshold, at 159 KIAS (ground speed of 167 knots).
Source: TSB
Appendix C – Sept-Îles Airport aerodrome chart
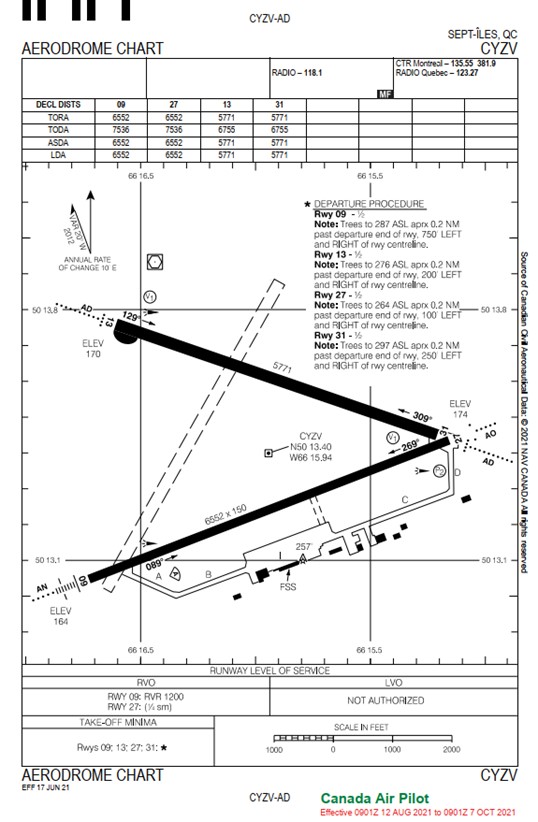
NOT FOR NAVIGATION
Source: NAV CANADA, Canada Air Pilot (CAP), CAP 5: Quebec, effective 12 August 2021 to 07 October 2021
Appendix D – Flight data plots
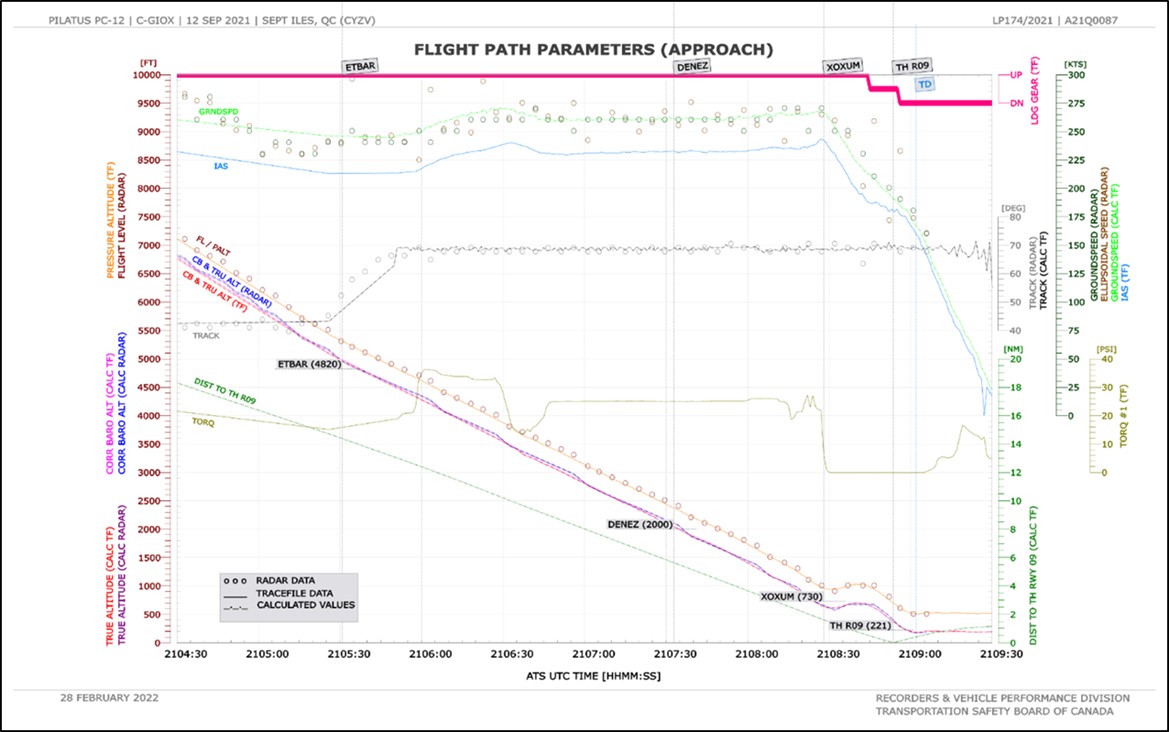
Source: TSB
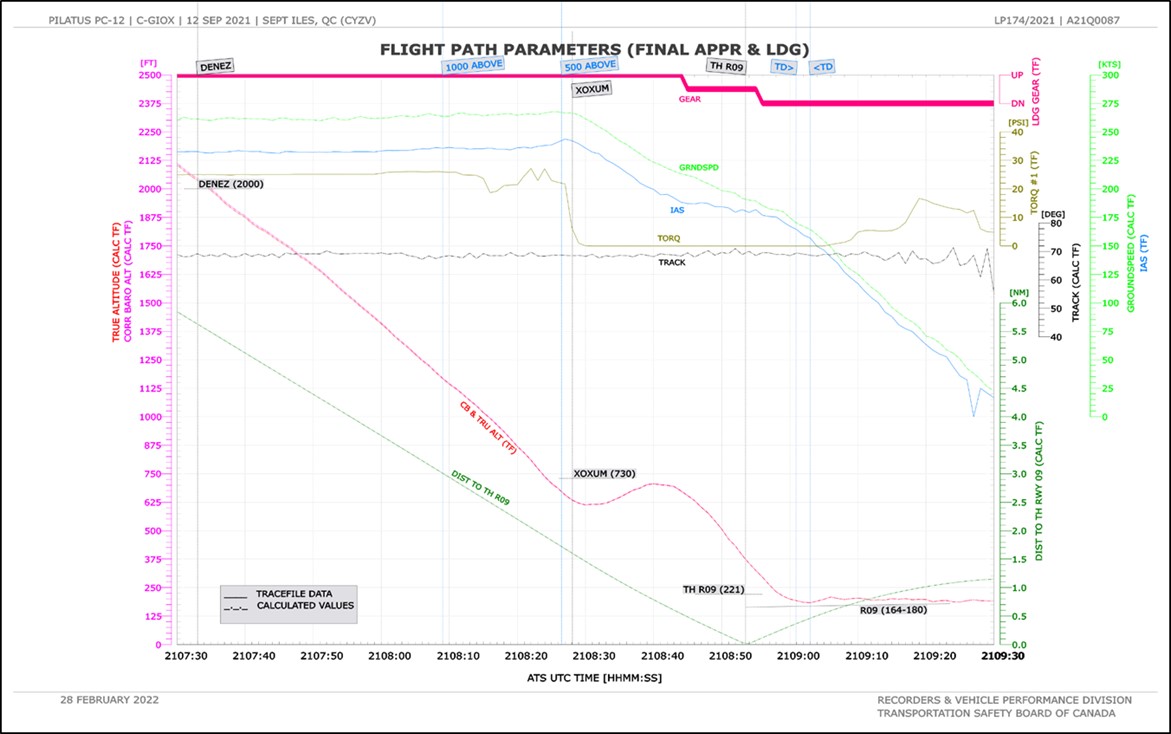
Source: TSB

Source: TSB