Striking of Wharf
Passenger Vessel Beaumont Hamel
Portugal Cove
Newfoundland and Labrador
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
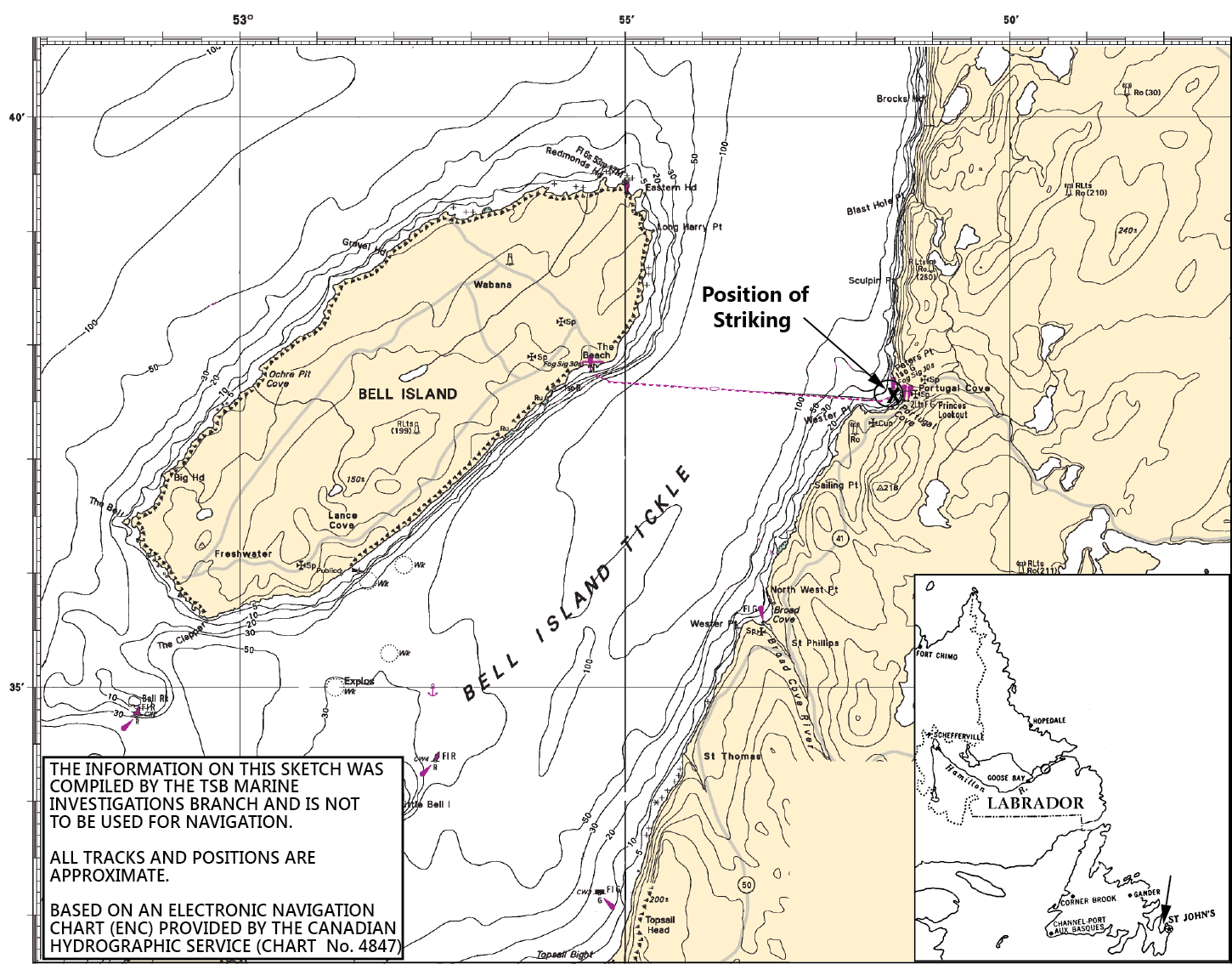
On 30 May 2012, at 1000 Newfoundland Daylight Time, the passenger ferry Beaumont Hamel experienced an electrical failure, resulting in loss of propulsion and steering while approaching Portugal Cove, Newfoundland and Labrador, and struck the wharf. The vessel sustained damage to the bow visor, and caused minor damage to the wharf. One minor injury was reported.
Factual information
Particulars of the vessel
| Name of Vessel | Beaumont Hamel |
|---|---|
| Official number | 803729 |
| Port of registry | St. John’s, Newfoundland and Labrador |
| Flag | Canada |
| Type | Roll-on/roll-off passenger ferry |
| Gross tonnage | 831 |
| LengthFootnote 1 | 53 m |
| Draught | Forward: 2.4 m Aft: 2.4 m |
| Built | 1985 |
| Propulsion | 2 x 600 kW electrically driven propellers mounted on steerable pods (pod thrusters) |
| Maximum capacity of vessel | 106 passengers, 33 vehicles |
| On board at the time of occurrence | 103 passengers, 27 vehicles |
| Crew | 9 |
| Registered owner and manager | Department of Transportation and Works, Newfoundland and Labrador |
Description of the vessel
The Beaumont Hamel was built in 1985 by the Department of Transportation and Works of Newfoundland and Labrador (DTW) as a prototype pod propulsion passenger ferry. The 53-m vessel has an open vehicle deck that can be boarded from either end, using ramps. The stern is open, and the bow is enclosed by a bow visor that can be raised and lowered. The vessel has a bow thruster that is normally used for docking and undocking.
The vessel is powered by 3 generator sets. Each generator set is comprised of a diesel main engine coupled to its own electrical alternating current (AC) generator. For the purpose of identification, these generator sets are numbered 1, 2, and 3. In normal operations, 2 generator sets operate in parallel to power 2 pod thrusters. Propellers are mounted on 360º rotatable pod thrusters, providing both propulsion and steering. The vessel can operate using only a single pod thruster powered by 1, or 2, of the generator sets.

The vessel is fitted with an electrical safeguard system, whereby each pod thruster has a shutdown circuit to ensure that at least 1 pod thruster remains available for propulsion. When 2 generator sets are operating in parallel, and 1 trips offline, the shutdown circuit activates, cutting power to 1 of the pod thrusters, and thus preventing an overload of the remaining generator set. However, if both generator sets trip simultaneously, the electrical system shuts down.
The vessel is fitted with an emergency generator; however, it does not provide propulsion, as it powers neither the bow thruster nor the pod thrusters. In the absence of electrical power, the pods can be manually steered from within the thruster compartment.
History of the voyage
At the time of the occurrence, the Beaumont Hamel was 1 of 2 vessels each operating between 12 and 18 hours a day to provide a scheduled service between Bell Island and Portugal Cove, Newfoundland and Labrador (Appendix A). The crossing of almost 3 nautical miles takes approximately 20 minutes.
On 30 May 2012, at 0550,Footnote 2 the vessel departed Bell Island for the first run of the day, using No. 1 and No. 3 generator sets. Later that morning, the master communicated with shore management, and submitted a requisition to hire a contractor to “troubleshoot and repair control problem with No. 2 generator.” Electrical instability on No. 2 had been reported to the bridge the previous evening. Instability had also been noted on 24 May. The vessel continued on the regular schedule of the MV Flanders.Footnote 3 At 0900, the electrical contractor boarded at Portugal Cove to address the electrical instability on the No. 2 generator set. Once the contractor was on board, the vessel remained in service, departing from Portugal Cove using No. 1 and No. 3 generator sets.
Halfway through the crossing, the engine room contacted the bridge, and requested that the master reduce power. The engine room put No. 2 online to monitor it under normal operating conditions. No. 2 and No. 3 were online when the vessel docked at Bell Island. No instability was noted during the crossing.
The vessel loaded, and departed from Bell Island around 0930. Monitoring of No. 2 continued during the 20-minute crossing to Portugal Cove. Although there was no electrical instability noted on No. 2 and No. 3, a greater fuel demand was observed on the No. 2 generator set. There was no indication on the bridge of the Beaumont Hamel to show which generator sets were in operation.
At 1000, the vessel was approaching the wharf in Portugal Cove at reduced speed, using No. 2 and No. 3 generator sets, when they both tripped offline simultaneously. The simultaneous trip caused a complete loss of power, and the vessel blacked outFootnote 4 approximately 50 m from the wharf. With no immediate means of propulsion or steering, the vessel continued toward the wharf, striking it at 1001.
Three minutes later, No. 1 and No. 3 were put online, and were used to dock the vessel. The Beaumont Hamel was taken out of service following the occurrence, and extensive repairs and adjustments were effected.
Transport Canada (TC) Marine Safety and Security attended the vessel on 30 May to authorize the temporary repairs for transit to St. John's. On 11 June, TC inspected the repairs to the bow visor door. At the request of DTW, a surveyor from Lloyd's Register attended with the TC Marine Safety Inspector (MSI), since the vessel's owner had applied for delegation to this recognized organization. On 14 July, TC attended sea trials on the vessel, and witnessed adjustments to the electrical system. The vessel resumed operations on 19 July, 51 days after the occurrence.
Damage to the vessel
The vessel sustained the following damage to the bow visor, between frames 76 and 77:
- A section of hull plating, approximately 2 m², was dented and sheared at the top of the indentation, 100 cm below the forecastle deck elevation (Photo 2).
- The centreline girder of the visor was deformed at the stem, and was buckled for approximately 1 m aft (Photo 3).
- The hull stringer, several deck beams, and flange brackets were also deformed in the area of the indentation (Photo 3).


Damage to the wharf
The damage to the Portugal Cove terminal was limited to the wooden cap rail around the edge of the concrete wharf (Photo 4). The damage had no effect on the ferry services.

Injuries
One passenger reported aggravation of a pre-existing injury following the accident. There were no other injuries reported.
Certification
Vessel
The vessel was crewed, equipped, and certified in accordance with existing regulations. Although not required by regulation, the DTW voluntarily complied with the International Safety Management (ISM) code. At the time of the occurrence, the DTW held a full-termFootnote 5 periodic document of compliance (DOC) issued by Lloyd’s Register.
Personnel
The master held a Master, Near Coastal certificate with no tonnage restriction, had been employed by the DTW since 1989, and had served as a master on the Beaumont Hamel since 2005.
The chief officer held a Master Mariner certificate, had been employed as a chief officer for the DTW since 2002, and had worked on the Beaumont Hamel since 2005.
The chief engineer held a Third-Class Engineer, Motor Ship certificate, had been employed as a chief engineer with the DTW since 1986, and had worked as chief engineer on the Beaumont Hamel since 2009.
The second engineer held a Third-Class Engineer, Motor Ship certificate, had been employed by the DTW since 1997, and had worked on the Beaumont Hamel since 2007. This individual had also worked as both a second engineer and a chief engineer throughout the fleet.
Environmental conditions
At the time of the occurrence, the vessel recorded good visibility and a northerly wind at force 6 on the Beaufort scale.Footnote 6 At 1000, the tide was low, at 1.3 m above chart datum.
History of blackouts
The Beaumont Hamel had sustained blackouts since it came into service in 1985, including 1 on its delivery voyage. There have been 8 such blackouts reported to the Transportation Safety Board (TSB), 3 of which have occurred since 2009. Additionally, over the years, the vessel experienced blackouts that were not recorded or reported.
On the Beaumont Hamel, a blackout impacts both the propulsion and steering capabilities of the vessel, making the reliability of the electrical system paramount. While steering on conventional vessels relies on the rudders with significant surface area, a pod steering system relies on propeller thrust. On the Beaumont Hamel, the emergency steering was considered redundant, because the vessel had 2 pod thrusters.Footnote 7 However, in the absence of electricity, the pod thrusters do not generate propulsion, which eliminates the redundancy. As a result, when the Beaumont Hamel experienced a blackout, it effectively had no means of emergency steering.
Following each of the Beaumont Hamel’s blackouts, repairs were undertaken to address various mechanical deficiencies that were thought to be causal. Maintenance included, but was not limited to:
- modifications to the engine speed control system in 2006;
- an overhaul of the fuel-supply system in 2009;
- an upgrade of the vessel’s engine control system in 2010; and
- a replacement of the fresh-water pump on No. 2 main engine in 2011.
Other repairs were undertaken; however, limited documentation prevented the development of a comprehensive history with respect to the vessel's maintenance. Following the blackout on 22 April 2009, a TC MSI visited the vessel, and issued a Marine Safety Notice (SI-07) indicating that the “vessel was not to carry passengers until reason for blackout during thruster preferential [sic] trip was determined and corrected.” The SI-07 required that the corrective action be verified by a TC MSI. To address the SI-07, an electrical contractor was engaged and subcontracted the evaluation of the fuel system. The subcontractor replaced a single fuel line feeding all generator sets with 3 new fuel lines to feed each generator set. No repairs were made to the vessel's electrical safeguard system. On May 14 2009, a TC MSI tested the vessel's electrical safeguard system, and verified that it functioned as intended.
Over the years, the repairs following the vessel's blackouts focused on mechanical failures that were thought to be causal. There was no documentation available to indicate that the effectiveness of these repairs had been evaluated by the DTW. Following this occurrence, DTW hired an electrical contractor to determine and correct the cause(s) of the blackouts. The contractor identified and corrected a number of mechanical and electrical issues that may have contributed to the loss of power on 30 May. The electrical safeguard system was initially targeted, and the preferential trip underwent extensive testing. However, no problems were identified with the preferential trip during the testing. The contractor determined that “the most probable cause of the loss of power incident was that radio frequency interference caused both circuit breakers to open.”Footnote 8
The Gallipoli, a diesel electric passenger vessel of comparable age and of similar electrical design, experienced 2 blackouts: 1 in 1999 and 1 in 2006. In 2011, 2 new vessels, the Hazel McIsaac and the Grace Sparkes, were constructed for the DTW on electrical plans similar to that of the Beaumont Hamel. Neither of the new-build vessels has diesel electric propulsion like the Beaumont Hamel, nor do either share the problem of repeated blackouts.
Department of Transportation and Works of Newfoundland and Labrador
The DTW employs over 2000 people across the province, and provides a range of transportation services, including provincial ferry service on 15 routes serving over 40 communities.Footnote 9 At the time of the occurrence, the DTW owned 10 vessels, of which 8 were crewed and operated by the DTW directly. The assistant deputy minister (ADM) is responsible for the overall management of the intraprovincial ferry services.Footnote 10
Safety management system
While no marine operation is entirely free of risk, there are numerous ways to identify, assess, and mitigate risks. One internationally recognized method is a safety management system (SMS). A SMS ensures “a structured, consistent and risk-driven method to identify and close critical safety gaps, adopt safety best-practices, and clearly demonstrate commitment to, as well as accountability and due diligence for, safety.”Footnote 11
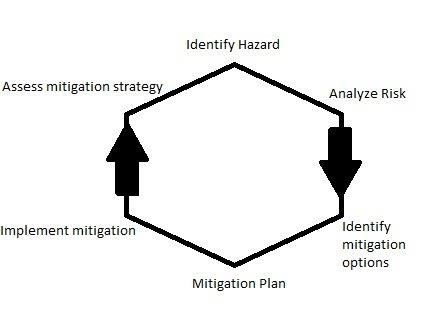
A SMS provides a formal framework for identifying and mitigating risk. Risk management under a SMS is an ongoing cycle that helps vessel operators identify, analyze, mitigate, and follow up on existing and potential risks (Figure 1). Each stage of the risk-management cycle should be supplemented with documentation that is “kept in a form that the company considers most effective.”Footnote 13 Documentation is necessary to enable tracking and to analyze the effectiveness of past risk assessments and mitigation strategies. This systematic process for managing risks ensures that individuals at all levels of an organization have the knowledge and tools needed to make sound decisions during both routine and emergency operations.
Although the benefits of SMSs have long been recognized by the marine community, a SMS is not required on all types of vessels. Canadian regulations did not require the Beaumont Hamel to have a SMS, and because the vessel was certified for domestic voyages only, the vessel was not subject to the International Convention for the Safety of Life at Sea (SOLAS). As such, the vessel was not required to comply with the International Management Code for the Safe Operation of Ships and for Pollution Prevention (ISM code).Footnote 14
The ISM code governs almost all of the international shipping community. It provides an international standard for the safe management and operation of ships and for pollution prevention. In order to comply with the ISM code, a ship must have a working SMS, consisting of the following:
- Commitment from top management;
- A procedures manual that documents what is done on board the ship during normal operations and in emergency situations;
- Procedures for conducting both internal and external audits to ensure the ship is following the procedures manual;
- A designated person ashore (DPA) to serve as the link between the vessel and shore staff and to verify the SMS implementation;
- A system for identifying actual practices that do not match documented practices, and for implementing associated corrective action; and
- Regular management reviews.
The TSB Watchlist identifies issues that pose the most serious risk to Canada’s transportation system, and SMS is on the TSB Watchlist. The TSB has repeatedly emphasized the advantages of SMSs in the marine industry, citing deficiencies in many occurrences. The TSB believes that TC should require all commercial vessels to have a SMS, and that all SMSs should be certified and audited. TC anticipates that Canadian regulations regarding requirements for SMSs will be prepublished in the Canada Gazette, Part I, in the second quarter of 2014. TC has confirmed that the regulations will not apply to all Canadian vessels; however, they will apply to passenger vessels carrying more than 50 people, such as the Beaumont Hamel.
Department of Transportation and Works of Newfoundland and Labrador safety management system
A SMS may not identify all risks in advance, but when a risk is identified—in advance or as the result of an accident—it should be assessed, and any necessary mitigating measures should be incorporated for the future. Risk management is a continuous cycle, not a one-time event. The SMS of the DTW had originally been certified in 2010. At the time of the occurrence on 30 May 2012, the TSB investigation determined the following risks were present in the routine operations of the DTW and Beaumont Hamel: recurring blackouts; management of public pressure; fatigue; a lack of hazardous-occurrence reporting; a lack of safety-focused investigations; limited maintenance tracking; and limited management of maintenance, given that the DTW operates an aging fleet.
Limited maintenance tracking
Historical maintenance records and failure information on safety-critical equipment is crucial from a maintenance perspective, both when assessing system performance and when planning risk-based preventive maintenance. The Beaumont Hamel kept a deck log, a radio log, and an engine log, as well as traffic sheets and a log of personnel on board.
The deck log is considered the official log, and is therefore a legal record of the vessel’s activities. As such, it should include information about weather conditions; vessel location; course; speed; and status of all critical systems, including any deficiencies. The engine-room log is a record of ship machinery parameters, performance, maintenance, and malfunctions.
In some instances, the vessel’s logbooks did not provide sufficient information to verify events on board. On shore, there was no systematic approach for tracking maintenance and following up on its effectiveness. In addition, maintenance records and other reports relating to the blackouts on the Beaumont Hamel were not consolidated and were stored in various locations, including the
- vessel’s engine-room logbook;
- maintenance log;
- deck log;
- regional manager’s office;
- shore-based financial department;
- human resources department; and
- engineering department.
There was no documentation available to indicate that the DTW had conducted follow-up testing or performed a post-occurrence risk analysis of the repairs following each blackout.
Maintenance management of an aging fleet
When a company operates an aging fleet, the downtime required for maintenance increases. The DTW acknowledged that its vessels were aging, and had an alternate vessel available to cover various ferry routes while the primary vessels were undergoing maintenance.Footnote 15 The DTW also commissioned a vessel-replacement strategy report. At the time of publication in 2006, the report stated that vessels, including the Beaumont Hamel, were “considered capable of providing an additional 10−15 years of service, [although] regular daily maintenance and equipment overhauls as needed or as recommended by manufacturers will most probably be insufficient to provide trouble-free service.”Footnote 16 The Beaumont Hamel was built in 1985, and was reaching the end of its optimal service life.
Management of public pressure
The Beaumont Hamel is 1 of 2 vessels that normally provided essential passenger service to and from Bell Island. The vessels also provided emergency medical transportation (EMT) services, and alternately covered 24-hour shifts on call. As with all vessels providing essential passenger service, there is a public expectation that service will be provided on all scheduled runs. As such, the vessel is subject to public pressure as part of normal operations. This pressure is to be expected; it must be anticipated and strategies must be in place, so that pressure to maintain service may be balanced appropriately against safety considerations.
Senior management at the DTW routinely received complaints from the public, and were therefore in a position to manage these complaints and minimize the transfer of public pressure to individuals responsible for making safety-critical decisions. However, complaints received at senior levels of government were often relayed immediately to the master or crew of the delayed vessel.
The DTW implemented a policy whereby passengers must exit their vehicles for the 20-minute crossing. However, after receiving public pressure in response to this policy, the DTW advised the crew of the Beaumont Hamel to cease enforcing the policy if passengers objected to being asked to exit the deck.
The schedule, and any change, is the responsibility of the DTW area manager, who supervises the masters. The master is ultimately responsible for making decisions that are in the best interests of the vessel's safety. Decision-making is a complex process; research into human behaviour has demonstrated that when people must solve a problem in a situation with no overarching guidelines or rules, they tend to frame the problem as a choice between gain and loss. Studies find that people tend to choose a solution with a potential high risk, rather than the solution that has a certain negative outcome.Footnote 17,Footnote 18 This tendency is referred to as negative framing bias.
In this occurrence, the master and the area manager agreed that the vessel should sail with the electrical contractor on board to troubleshoot and repair No. 2 generator set. Because a blackout was considered unlikely, it was decided to maintain the schedule rather than face the certain negative public response to a service disruption.
Crew scheduling and fatigue
Fatigue refers to the body's response to sleep loss or sleep disruption. The effects of fatigue lead to the following decrements in performance: slower reaction times,Footnote 19 reduced forward planning,Footnote 20,Footnote 21,Footnote 22 increased risk-taking, inability to solve problems in parallel, and persistence with tasks beyond a reasonable end point, among others. All of these effects may pose serious risks to safety if experienced by personnel in safety-critical positions. Fatigue-management responsibilities require both the company and the employees to manage the work schedule and working environment to minimize the risk of fatigue.
The DTW is responsible for ensuring that crew schedules, at minimum, meet the regulations for rest (6 hours of rest in 24 hours, and 16 hours of rest in 48 hours);Footnote 23 that the schedule allows for sufficient restorative sleep to be obtained; and that crew quarters and other aspects of the working environment facilitate healthy sleep. Crew members are responsible for following the rest schedule, reporting when they are unfit to work due to fatigue, and reporting aspects of the company's fatigue-management plan that are deficient. The vessel's master is responsible for monitoring and enforcing the company's fatigue-management policies and procedures. The master must also work with the crew and the company to rectify problems, so as to minimize the risk of fatigue.
The DTW has a fatigue-management plan, and acknowledged that there was a high risk of fatigue on the Bell Island route because of the rigorous schedule. The Beaumont Hamel normally operated for 12−18 hours per day, and was also required to make periodic emergency runs. The master was responsible for adjusting the work schedule following emergency runs, and routinely did so. The crew's collective agreement stipulates that crews on the Bell Island route work on a 1-week schedule, rather than the fleet-wide 2-week schedule. This change was intended to mitigate the risk of fatigue. However, even after the schedule change, crew members reported feeling fatigued at the end of a 1-week shift.
A review of the schedules for crew members on the Beaumont Hamel revealed that there were frequent departures from the minimum required 6 hours of sleep-time, as well as frequent examples of workdays extending to the point when the minimum hours of rest fell below 16 hours in a 48-hour period.Footnote 24 Furthermore, emergency crossings and extended days, resulting from traffic backups or the lack of a partner vessel on the route, disrupted the standard schedule and added additional risk of fatigue.
Poor sleeping environments that do not provide adequate space, nor appropriate control of heating, cooling, and noise, contribute to reduced sleep quality. The Beaumont Hamel was not originally designed to have the crew sleep on board; however, crew accommodations were retrofitted in the engine casing. Several aspects of the accommodation design are counter to best practices for providing an environment conducive to restorative sleep, including the following:
- Cabin bulkheads did not seal with the ceiling, allowing entrance of hallway light, as well as noise from the hallway, the adjacent cabins and from the other Bell Island vessel, including disruptions for emergency runs when the other vessel was called out.
- Cooling was achieved by opening the window, and heating was either on or off.
- The vessel was fitted with transverse bunks that have the same 3° list to port as the vessel. Some crew members were required to sleep with their heads oriented in the 3° down position.
- Cabins were small, meeting the minimum regulatory requirements for square footage, but not for volume.
The Beaumont Hamel moors at Bell Island at night, and the crew members generally remain on board, unless they live on Bell Island and wish to commute to work. Eight of the 9 crew members on the vessel at the time of the occurrence normally slept on board. Restorative sleep was difficult to obtain on the Beaumont Hamel.
Hazardous-occurrence reporting
Companies that operate under the ISM code are responsible for establishing a systematic procedure to report all hazardous occurrences. These reports are then investigated and analyzed, with a focus on safety and pollution prevention. Procedures for carrying out any necessary corrective action must also be in place.
The DTW did not have documentation available to demonstrate that consistent hazardous-occurrence reporting was taking place, nor were there established procedures within the DTW to allow for safety-focused investigations of hazardous occurrences. There were no written records of hazardous occurrences or near misses from the eastern region; specifically, there were no reports from the Beaumont Hamel. For example, blackouts that occurred but had no adverse consequences on the Beaumont Hamel's operations were not reported as required in the company SMS.Footnote 25
Investigations at the Department of Transportation and Works of Newfoundland and Labrador
When the SMS manual was written in 2010, the safety and compliance officer was the DPA and was to be responsible for accident investigation. However, this function was deleted from the DPA's purview before any investigations could occur. Accident investigations were carried out exclusively by the DTW's human resources department, with the sole purpose of determining culpability. There were no internal safety or technical investigations conducted into the blackout on 30 May.
Voyage data recorder
The TSB uses the data from a voyage data recorder (VDR) to support an investigation. In addition to bridge audio, a VDR is expected to record date, time, heading, position, speed, radio communications, radar images, weather, engine orders, and vessel responses.
The Voyage Data Recorder RegulationsFootnote 26 came into force in January 2012, requiring existing passenger vessels over 500 gross tons to carry VDRs. The Beaumont Hamel carried a VDR, as required, which was newly installed. The relief master activated the saving feature for VDR data immediately following the occurrence; however, due to a technical fault in the VDR, no data were stored. The TSB investigation could not determine why the VDR was not recording data. There was no on-board requirement to verify that the VDR was functional.
Analysis
Events leading to the striking
On 30 May 2012, the Beaumont Hamel, loaded with vehicles and passengers, was approaching Portugal Cove when both generator sets tripped offline, causing the vessel to black out approximately 50 m from the wharf. An electrical instability and fuel imbalance had been noted earlier; however, it is not known if these irregularities contributed to the simultaneous trip. There was insufficient time to restart the engine in order to regain immediate propulsion and steering, and as a result, the vessel struck the wharf. Although the post-occurrence electrical report indicated that the most likely cause of the blackout on 30 May was radio interference, the investigation did not conclusively determine the cause(s) of the repeated blackouts.
The Beaumont Hamel had been providing passenger ferry service between Bell Island and Portugal Cove for over 25 years, despite a history of recurring blackouts. The safety management system (SMS) of the Department of Transportation and Works of Newfoundland and Labrador (DTW) was not effective, allowing hazards, such as those associated with recurring blackouts, to persist unaddressed on the vessel. Other safety issues were also found to be present either on the vessel or within the DTW, including those associated with management of public pressure, management of maintenance for the DTW's aging fleet, limited maintenance tracking, fatigue, a lack of hazardous-occurrence reporting, and a lack of safety-focused investigations.
Safety management system
Maintenance tracking and assessment
Safety is enhanced when the history of a vessel and its equipment is available; this history allows for analysis of trends, and enables preventive maintenance to be carried out. Effective maintenance on a passenger vessel such as the Beaumont Hamel requires a systematic method of reporting, tracking, and assessing repairs. Without a complete written history, the task of identifying the cause(s) of the recurring blackouts and establishing links to the present occurrence was not possible.
Although the crew and contractors fixed mechanical deficiencies following each blackout, these repairs did not prevent further blackouts. Since the effectiveness of the vessel's maintenance was not assessed, efforts to address the blackouts continued to focus on mechanical deficiencies, and did not address the underlying electrical nature of the problem. The limited documentation resulting from the lack of systemic record-keeping impeded the DTW in its ability to analyze trends and perform effective preventive maintenance.
Maintenance management of aging fleet
Aging vessels require more maintenance. Although the DTW acknowledged the risks associated with an aging fleet, the Beaumont Hamel often operated under extended hours, and maintenance was sometimes deferred in order to keep the vessel in service.
Fleet renewal was included in the 2011/2012 annual report. Specifically, the report stated that “By March 31, 2012, Transportation and Works will have advanced its vessel-replacement program with the delivery and design of new ferry vessels.”Footnote 27 The DTW constructed 2 new vessels in 2011, and the design work has been completed.
Other than annual refit periods and the provision of an alternate vessel that was taken out of service in the fall of 2012, the DTW had no other risk-mitigation strategies in place to manage the increased maintenance associated with an aging fleet. Operating an aging fleet without an adequate risk-mitigation strategy in place puts the vessels, the crew, the passengers, and the environment at risk.
Management of public pressure
Necessarily, the master of a vessel must have overriding authority to determine when the safety of the vessel, crew, passengers, and environment are at risk. This means that a master must be able to make complex decisions based on factual information available at the time. The master must also be aware of the status of all critical systems. The master's decision about safety-related delays must be supported by shore management, regardless of operational demands or advertised schedules. On 30 May, the area manager supported both the master's request for an electrical contractor and the master's decision to continue to sail.
There is a fine balance between service provision and safety on passenger vessels. It is essential that management recognize the master's role in complex safety-critical decisions, and appropriately balance public pressure with safety considerations, even when these decisions may temporarily compromise service.
A decision to take the vessel out of service to test the No. 2 generator would have had a certain negative outcome: a public backlash for the service delay, especially given that the Flanders was not in service. Complaints received by senior management would likely be relayed directly to the master and crew, as had been done in the past. In contrast, testing the No. 2 generator set en route had only the potential for a negative outcome. When public expectations are not effectively managed, they may adversely affect the ability of management and employees to make safety-critical decisions. Unmitigated public pressure played a role in keeping the Beaumont Hamel in service on 30 May while the electrical contractor was on board.
Fatigue
Crew fatigue is affected by work schedule, operational requirements, sleep quality, emergency requirements, and quality of accommodations where rest is obtained. Poor sleeping environments that do not provide adequate space or appropriate control of heating, cooling, and noise contribute to reduced sleep quality, and hence provide less recuperative rest. These factors must be mitigated by management, including by the master of the vessel.
The Beaumont Hamel crew members' levels of fatigue were systematically increased at the end of their 1-week shift as a result of accumulated sleep debt, despite the adjustments to the vessel's work schedule. The mitigation strategies employed did not adequately address the risk of fatigue: they did not meet the minimum regulatory requirements, while the work schedule did not allow for sufficient restorative sleep, and the crew quarters did not facilitate restorative sleep. Fatigue-management plans that do not provide sufficient opportunity for restorative sleep increase the risk of reduced crew performance on a routine basis.
Hazardous-occurrence reporting
Since analysis of hazardous occurrences and near-misses is as significant for effective safety management as analysis of actual occurrences, there must be a method of encouraging and tracking reporting. Follow-up of hazardous-occurrence reports is required by the International Safety Management (ISM) code. While the SMS of the DTW is clear about reporting requirements,Footnote 28 no hazardous occurrence reports existed for the previous blackouts on the Beaumont Hamel. Without reports on these blackouts, crew and shore management were limited in their ability to identify trends that may have assisted in pinpointing the cause of the blackouts.
When hazardous occurrences and near misses are not reported, there is a risk that crew members, shore-side management, and contractors may be limited in their ability to identify and analyze trends, predict maintenance, and continuously improve safety in order to prevent future accidents or incidents.
Safety investigation at the Department of Transportation and Works of Newfoundland and Labrador
As per the ISM code, the company SMS should include procedures to ensure that any nonconformities, accidents, and hazardous occurrences are reported to the company, investigated, and analyzed with the goal of continuous safety improvement.Footnote 29 However, there were no safety investigations being conducted at the DTW. The role of accident investigation had been removed from the designated person ashore (DPA), and the only investigations conducted were those being carried out by the human resources (HR) department. HR investigations were focused on determining the culpability of the individuals involved, and tended to result in disciplinary action rather than safety action. When accident investigations are not safety-focused and have potential punitive consequences, there is a risk that individuals with important knowledge may not report all information for fear of repercussions, and safety deficiencies may persist unaddressed.
Voyage data recorder
The purpose of a voice data recorder (VDR) is to create and maintain a secure, retrievable record of information indicating the position, movement, physical status, and control of a vessel for the period covering the most recent 12 hours of operation. Objective data are invaluable to investigators when seeking to understand the sequence of events leading to an accident, and identifying operational problems and human factors. Reliable VDR data lead to a more accurate investigation and more timely communication of safety deficiencies and investigation reports to stakeholders and the public.
The Beaumont Hamel VDR was not recording data, and displayed an error code following the occurrence; however, there was no company SMS requirement that the VDR be checked operationally. The investigation could not determine why the VDR was not recording.
If voyage data recordings are not available to an investigation, this may preclude the identification and communication of safety deficiencies to advance transportation safety.
Findings
Findings as to causes and contributing factors
- The vessel struck the wharf after sustaining a total blackout, the cause of which could not be determined. The blackout caused the vessel to lose propulsion and steering.
- Despite mechanical repairs intended to address recurring blackouts on the vessel, this maintenance did not identify nor address the cause(s) of the blackouts, and they continued.
- Although the Department of Transportation and Works of Newfoundland and Labrador (DTW) had a safety management system (SMS) in place, the system was not effective at mitigating the operational risks posed by the recurring blackouts.
Findings as to risk
- Without a systemic method to identify, analyze, and follow up on safety deficiencies, whether an accident happens or not, there is a risk that these deficiencies will persist unaddressed.
- When public pressure is not effectively managed, it may adversely affect the ability of management and employees to make safety-critical decisions.
- Operating an aging fleet without a risk-mitigation strategy in place puts the vessels, the crew, the passengers, and the environment at risk.
- Fatigue-management plans that do not provide sufficient opportunity for restorative sleep increase the risk of reduced crew performance on a routine basis.
- When hazardous occurrences and near misses are not reported, crew members, shore-side management, and contractors may be limited in their ability to identify and analyze trends, plan maintenance, and continuously improve safety in order to prevent future accidents or incidents.
- If accident investigations are not safety-focused and have potential punitive consequences, there is a risk that individuals may not report all known information, and that safety deficiencies may persist unaddressed.
- If voyage data recordings are not available to an investigation, this unavailability may preclude the identification and communication of safety deficiencies to advance transportation safety.
Safety action
Safety action taken
The Department of Transportation and Works of Newfoundland and Labrador (DTW) has installed a computerized maintenance-management system on the Beaumont Hamel and in its company office. This system tracks corrective maintenance, send alerts about planned maintenance and, based on the corrective maintenance and the planned maintenance, can suggest preventive maintenance.
Following the blackout, the electrical contractor performed the following work on the Beaumont Hamel:
- Installation of a load-sharing alarm and power-shedding system;
- Removal of under-voltage trip coils that were unnecessarily delaying the restoration of propulsive power (both of the vessel’s pod thrusters’ circuit breakers were originally installed with under-voltage trip coils);
- Installation of an automatic start system for the standby generators;
- Adjustment to the electrical safety-system timing to ensure optimal performance; and
- Installation of a flying start system which allows a stopped pod thruster to be started, even if the propeller is freewheeling.
As well, the generator engine fuel pumps were overhauled and calibrated.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .
Appendices