Accidental release of free-fall lifeboat
Bulk carrier Blue Bosporus
English Bay, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 01 December 2020, the crew on the bulk carrier Blue Bosporus were carrying out a free‑fall lifeboat drill at Anchorage 12 in English Bay, British Columbia, when the wire rope slings holding the lifeboat failed and it fell approximately 14 m to the water. There were 2 crew members in the lifeboat at the time. Both crew members were seriously injured and were transferred to hospital. The forward starboard side of the lifeboat’s hull was damaged. There was no pollution.
1.0 Factual information
1.1 Particulars of the vessel
| Name of vessel | Blue Bosporus |
|---|---|
| International Maritime Organization number | 9370185 |
| Flag | Panama |
| Type | Bulk carrier |
| Deadweight tonnage | 78 819 |
| Gross tonnage | 41 668 |
| Length overall | 225.0 m |
| Moulded breadth | 32.24 m |
| Design draft | 14.38 m |
| Draft (at the time of the occurrence) | 4.84 m (forward), 7.03 m (aft) |
| Built | 2007 |
| Builder | Sanoyas Hishino Meisho Corporation |
| Crew complement | 20 |
| Registered owner | Falcon Shipholding Inc. |
| Ship manager | Apollonia Lines S.A. |
| Classification society | Nippon Kaiji Kyokai |
| Issuing authority for International Safety Management certification | Nippon Kaiji Kyokai |
1.2 Description of the vessel
The Blue Bosporus is a bulk carrier built in 2007 (Figure 1). The accommodation is located aft and has 5 decks, including the navigational bridge deck and decks A to D. The wheelhouse, located on the navigational bridge deck, is equipped with all navigational equipment required under the International Convention for the Safety of Life at Sea (SOLAS).Footnote 1,Footnote 2 The vessel is fitted with a rescue boat and a free-fall lifeboat.Footnote 3

1.2.1 Free-fall lifeboat
The lifeboat (type GARS 6-7, build number FF70) was made in 2007 by Shigi Shipbuilding Co. Ltd. (Figure 2). It weighs 3240 kg when empty and has 25 seats. Each seat has a restraining harness.
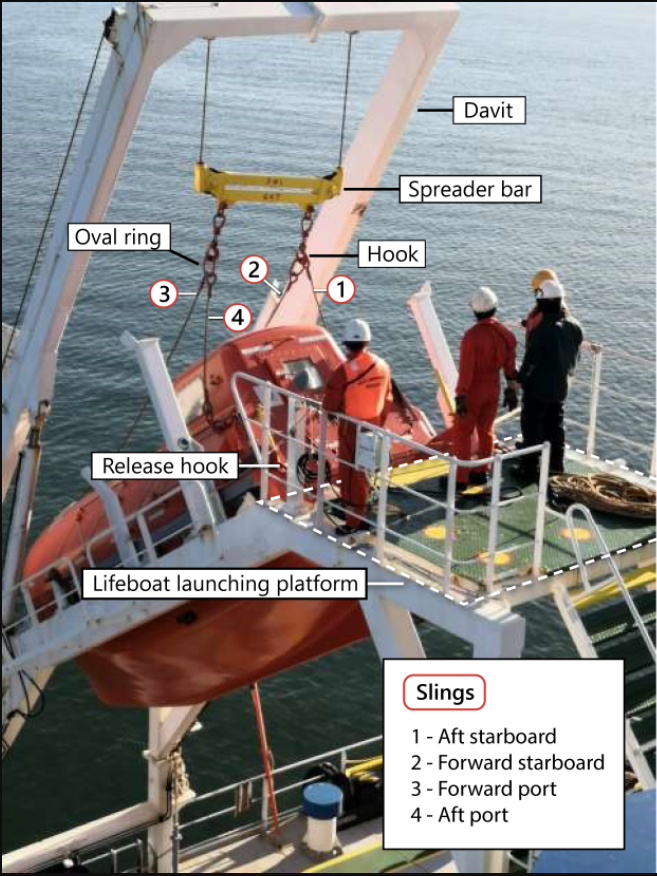
The lifeboat is stowed about 6 m above the main deck level on a raised launching structure located aft on the Blue Bosporus (Figure 2). When the vessel is at an even keel, the lifeboat is positioned with its bow down toward the vessel’s stern at an angle of 35° to the waterline.Footnote 4 The lifeboat is secured to the launching platform by a release hook that is attached to the platform.
The lifeboat can be free-fall launched by manually activating a release handle located inside the lifeboat, which hydraulically retracts a piston that unlatches the release hook. The release hook has an external safety pin to prevent its accidental release. A secondary back-up release mechanism is fitted should the primary release handle and pump fail.
The lifeboat can also be lowered and retrieved using a davit. The davit is typically used to lower the lifeboat during drills and tests and was being used to lower the lifeboat at the time of the occurrence.
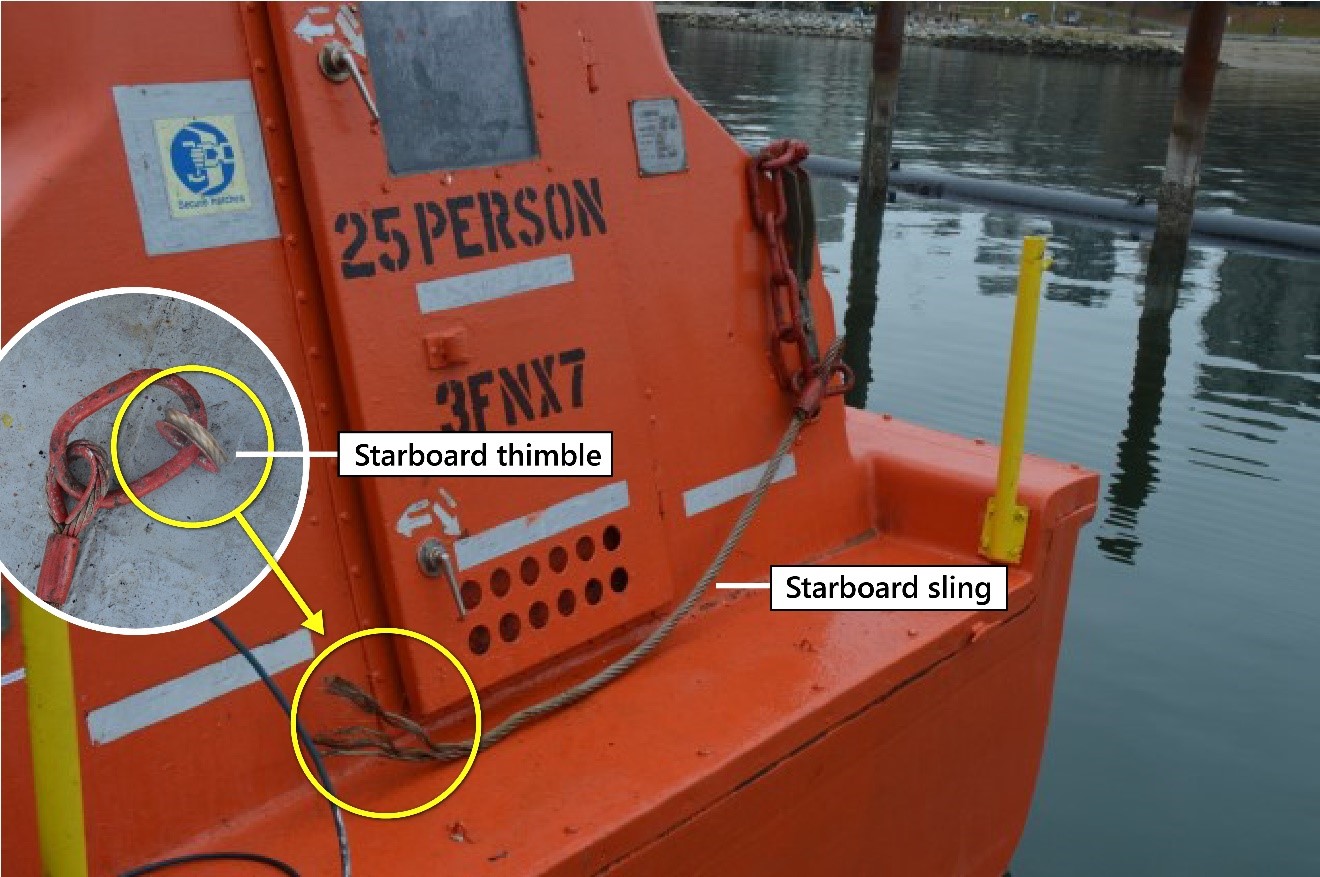
Before lowering the lifeboat using the davit, the lifeboat must first be attached to the davit using 4 wire rope slings (slings) (Figure 2). The lower end of each sling is attached to the lifeboat with a shackle. The upper end of each sling is permanently coupled to an oval ring; the oval ring is then connected to a hook on the spreader bar. The investigation could not determine how or where the slings were stowed when not in use.
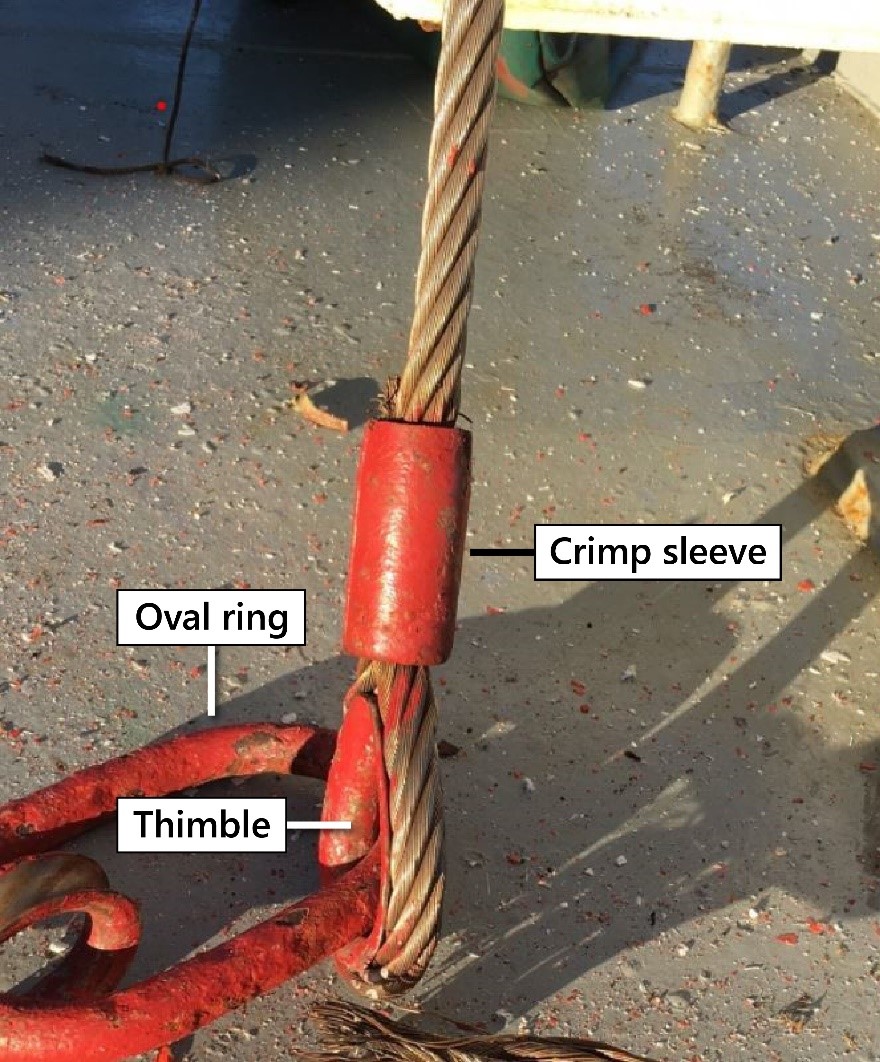
The slings in use at the time of the occurrence consisted of wire ropes with an eye at either end. The eye was formed by threading the wire rope around a thimble and then securing the wire in place using a crimp sleeve (Figure 3). A crimp sleeve is a type of mechanical splice that can be crimped using a hydraulic machine or hand tools. In this case, the crimp sleeves were crimped using a hydraulic machine during manufacture.
1.3 History of the occurrence
On 01 December 2020, while the Blue Bosporus was at Anchorage 12 in English Bay, British Columbia (BC) (Appendix A), a lifeboat drill was planned according to the vessel’s drill schedule. During the drill, the lifeboat was to be lowered to the water using the davit and taken for a test run.
Around 1300,Footnote 5 the master obtained permission to conduct the drill from the Vancouver harbour master and Victoria Traffic. At 1303, an announcement was made over the vessel’s public address system informing the crew that the lifeboat was to be lowered and taken for a test run in the water. At 1305, all crew members on the Blue Bosporus mustered at the lifeboat station, with the exception of the second officer who remained on the bridge on anchor watch. The master went from the bridge to the aft section of D deck, where he could observe the drill from a distance of about 15 m.
The chief officer, who would normally supervise the drill, had not supervised a free-fall lifeboat drill on the Blue Bosporus since joining the vessel 2.5 months earlier. As a result, the chief officer asked the third officer to prepare the lifeboat for release as well as supervise the 2 able seafarers who were also part of the drill. The third officer and the 2 able seafarers proceeded to the launching platform. The fourth engineer also proceeded to the launching platform, but left after confirming that engineering assistance was not needed.
Meanwhile, the chief officer stood by on the main deck waiting for the lifeboat to be lowered so that he could board the lifeboat with another crew member and take it for the test run. The bosun stood by the davit controls on the main deck.
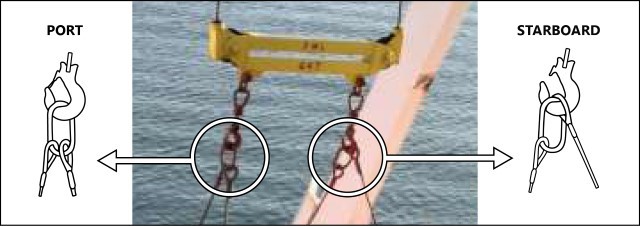
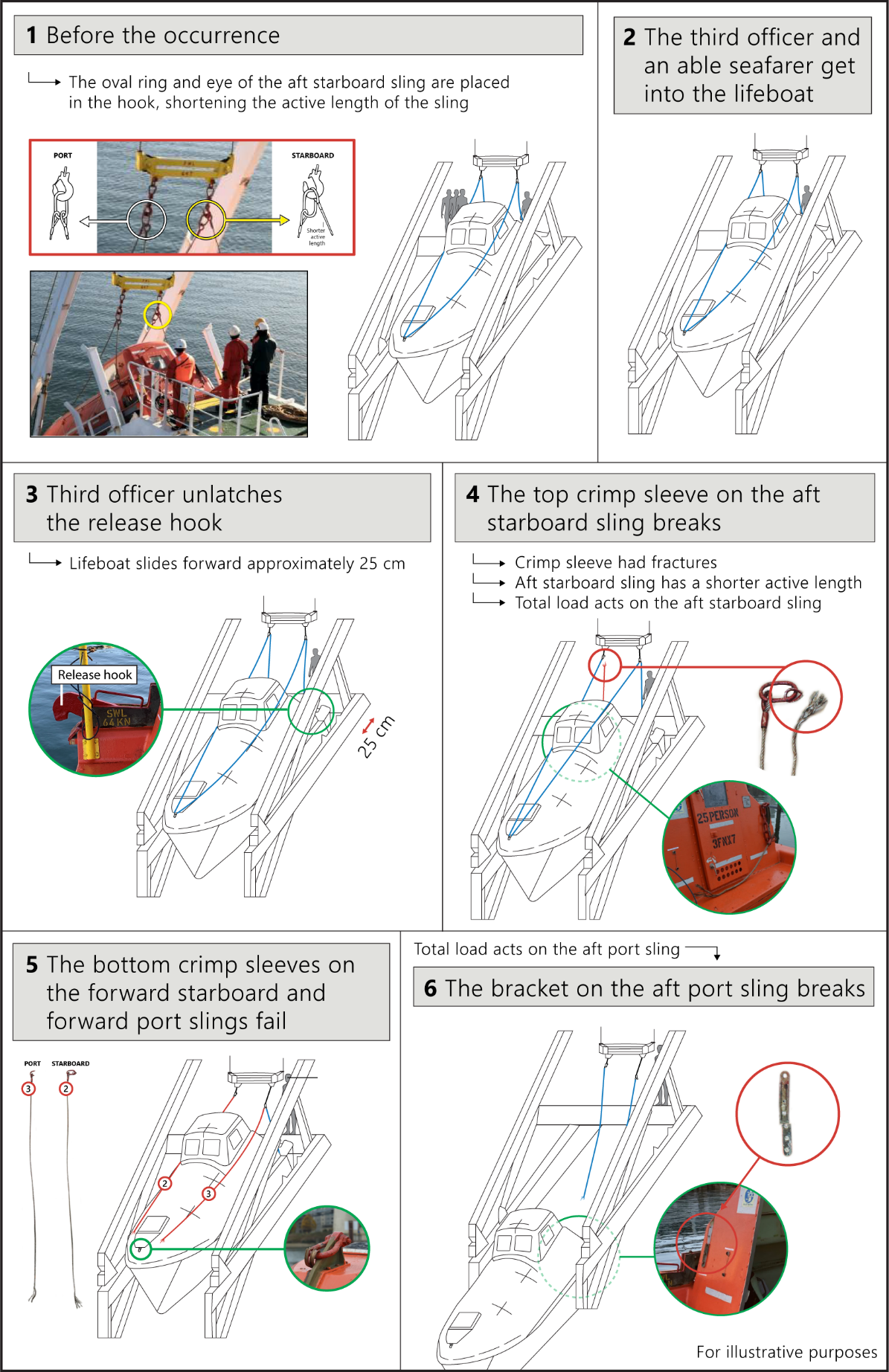
The third officer used hand signals to communicate with the bosun to lower the davit so that the lifeboat’s slings could be connected to the hooks on the spreader bar. Once the hooks were within reach, the launching crew took the oval rings and attached them to the hooks on the spreader bar. On the port side, the crew placed the oval ring into the hook. On the starboard side, they placed the oval ring and the eye of the aft starboard sling into the hook, shortening the sling length (Figure 4).Footnote 6
Once the slings were connected, the third officer tested the tension in the slings by pushing them forward with his hand. The third officer then signalled to the bosun to lift the lifeboat slightly in order to increase the tension on the slings.
At 1310, the third officer informed the master, via very high frequency radiotelephone, that the lifeboat was ready to launch. The master gave the third officer permission to continue with the launch, and the third officer removed the safety pin. The third officer directed one of the able seafarers to monitor the release hook and inform him when it was unlatched. The other able seafarer opened the lifeboat door from outside and stepped aside to let the third officer enter.
The third officer entered the lifeboat and stood beside the coxswain’s chair facing toward the bow of the lifeboat. He then moved the release handle up and down 8 to 10 times in order to build up the hydraulic pressure needed to unlatch the release hook (Figure 5).

During this time, the able seafarer who had opened the lifeboat door climbed onto the small platform at the stern of the lifeboat and then into the lifeboat to observe the third officer unlatch the release hook. The other able seafarer remained on the launching platform.
Once the hydraulic pressure was sufficient, the release hook unlatched, and the lifeboat slid forward approximately 25 cm. At this point, the aft starboard sling failed, followed by the 2 forward slings. The bracket holding the aft port sling onto the lifeboat broke off as well. The lifeboat fell about 14 m into the water.
Figure 6 illustrates the sequence of events.
At 1313, the crew on the Blue Bosporus brought the lifeboat alongside using the attached messenger line. The chief officer climbed down a ladder to check the condition of the 2 crew members inside and found that both had sustained injuries. The master requested shore-side assistance immediately. Both crew members were transported to the Canadian Coast Guard base in Kitsilano, BC, and then taken to hospital.
1.4 Injuries
One of the crew members in the lifeboat sustained serious injuries to his legs. The other crew member in the lifeboat sustained a serious injury to his hand.
1.5 Damage
The fibreglass beneath the forward starboard side of the lifeboat’s hull was damaged when the lifeboat hit the water.
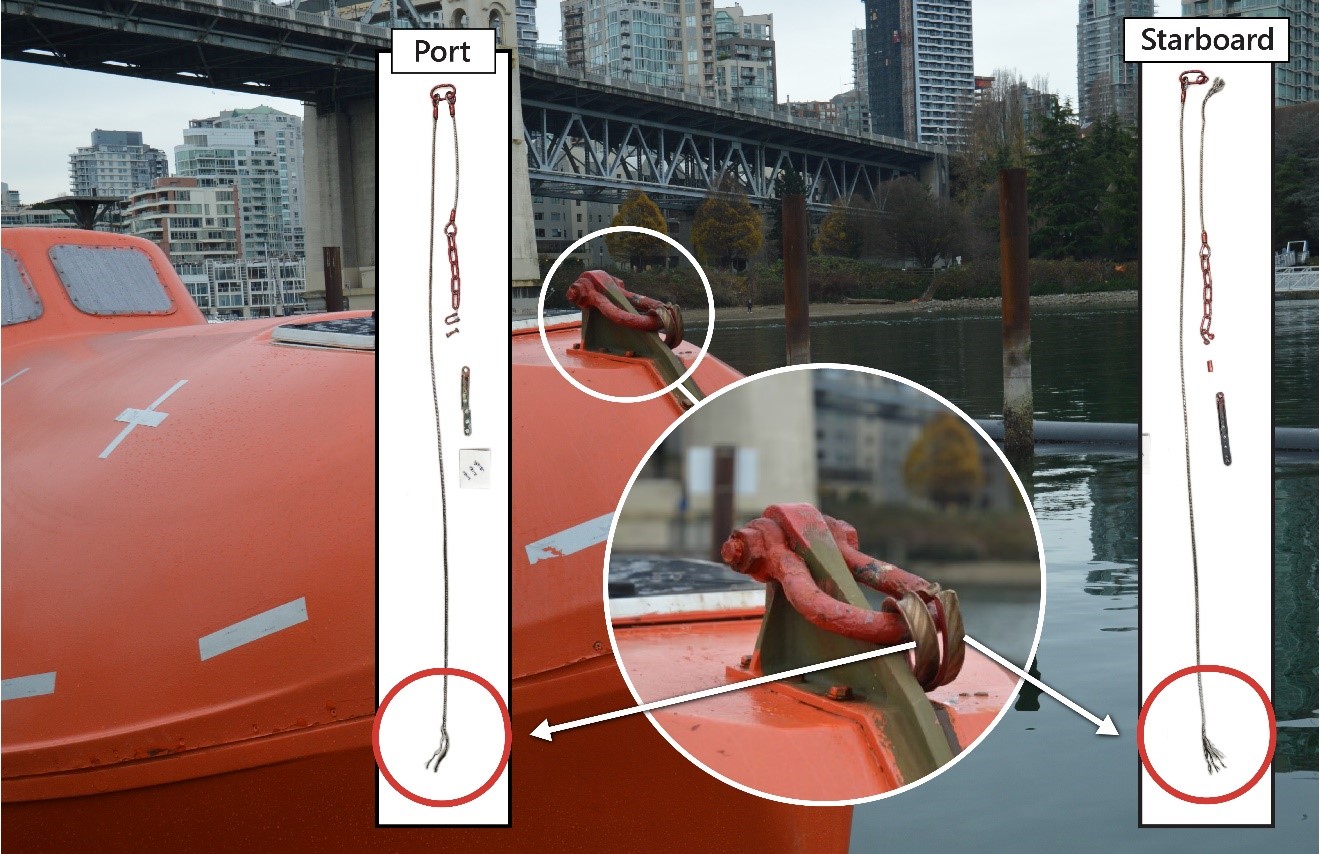
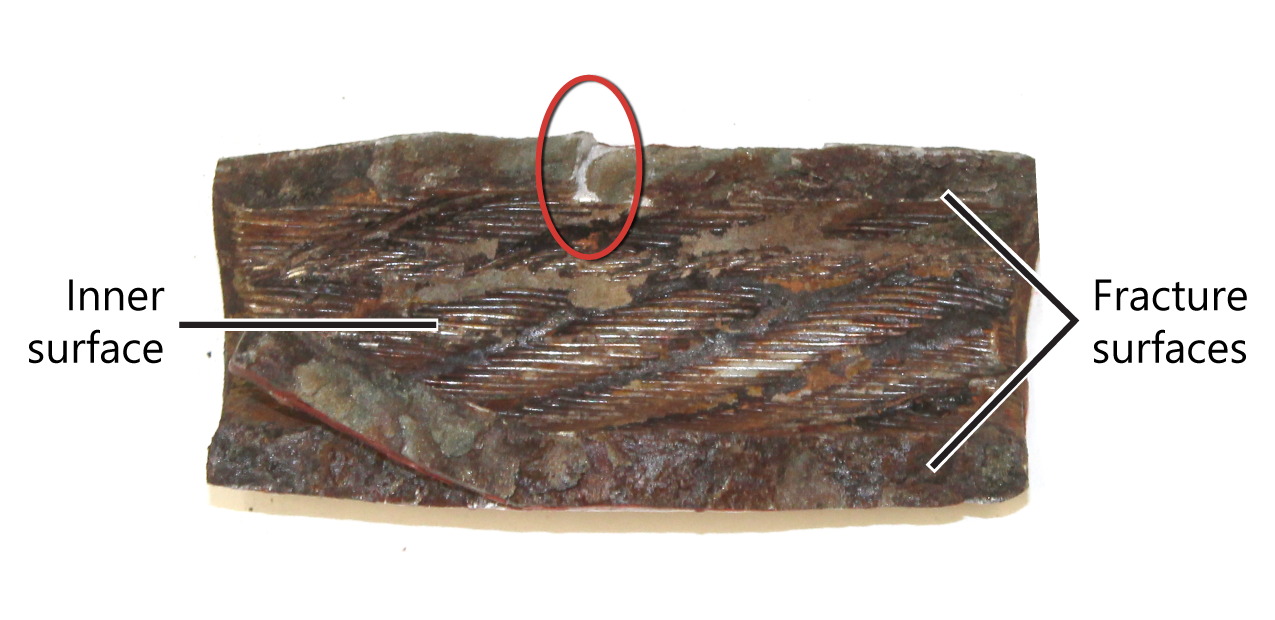
The crimp sleeve on the upper end of the aft starboard sling broke off, and the wire rope detached from the thimble (Figure 7). A portion of the broken crimp sleeve was retrieved. It was cracked in half.
Both of the crimp sleeves that attached the 2 forward slings to the lifeboat broke off and the wire ropes detached from their thimbles (Figure 8). These crimp sleeves were lost in the water.
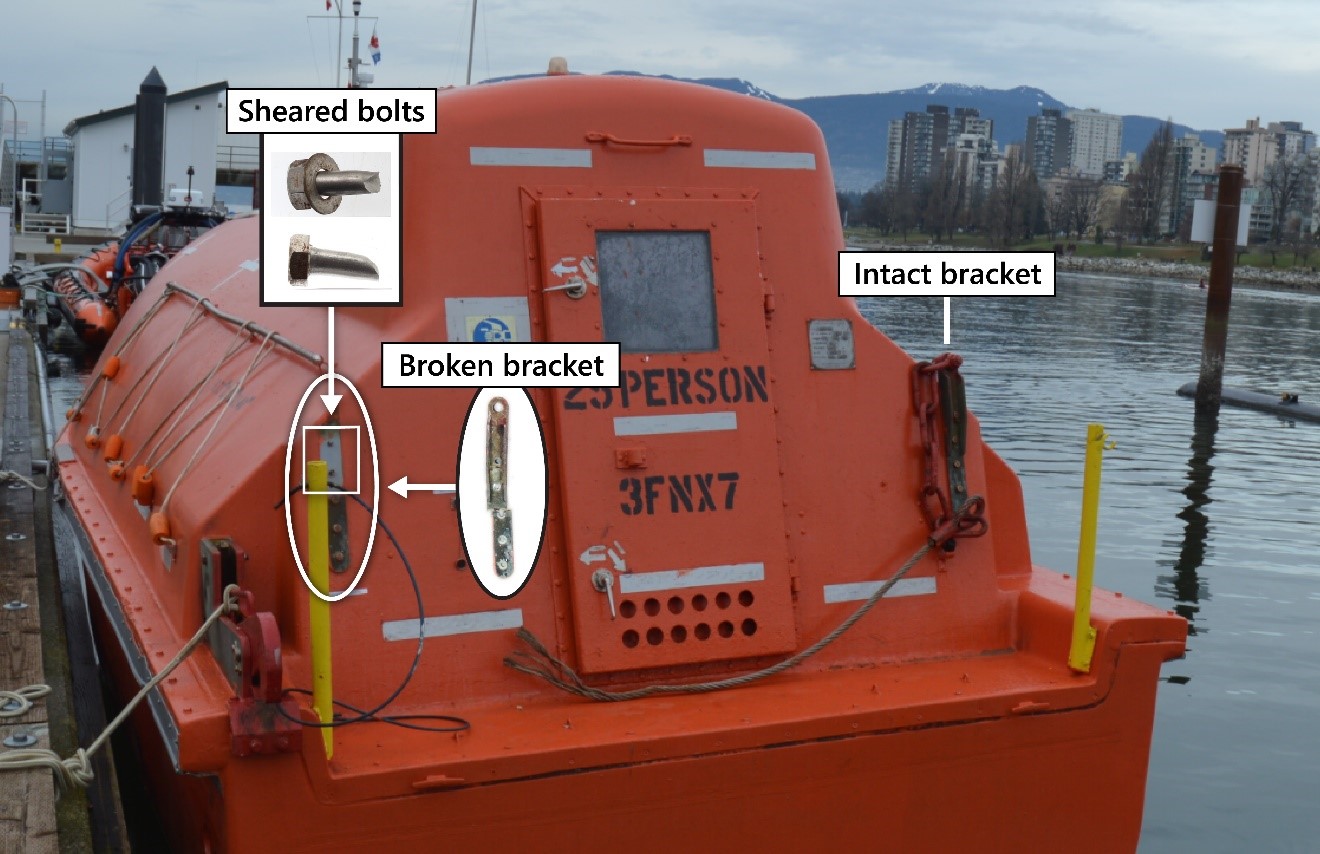
The aft port sling remained intact, but the bracket that attached the sling to the lifeboat broke off (Figure 9). The bolts that were securing the bracket to the lifeboat were retrieved and were found to have sheared off (Figure 9).
1.6 Environmental conditions
At the time of the occurrence, the tide was slack with a current of about 2 knots and the wind was north-northwesterly at 4 knots. The swell height was 0.2 m. It was daylight and the skies were clear, with visibility reported as 15 nautical miles. The air temperature was 9 °C, and the water temperature was also 9 °C.
1.7 Vessel certification
The Blue Bosporus was crewed, equipped, and certified in accordance with International Maritime Organization (IMO) regulations. As required by the International Management Code for the Safe Operation of Ships and for Pollution Prevention (the ISM Code), the vessel held a valid safety management certificate.Footnote 7 The vessel was classed with Nippon Kaiji Kyokai (known as ClassNK), and its safety management certificate, issued by ClassNK, was last audited on 07 July 2019.
1.8 Personnel certification and experience
The master held a Master Mariner certificate of competency issued by the Republic of the Philippines in 2008 and endorsed by the Republic of Panama in 2020. He had worked as a master on bulk carriers since 2008 and had joined Apollonia Lines S.A. on 16 March 2020 as master on the Blue Bosporus. Two free-fall lifeboat drills, including this one, had been carried out since he had become master on the Blue Bosporus.
The chief officer held a Master Mariner certificate of competency issued by the Republic of the Philippines on 08 March 2017 and endorsed by the Republic of Panama in 2019. He had worked as a chief officer on bulk carriers since 2018 and had been working for Apollonia Lines S.A. since 2019. He joined the Blue Bosporus on 15 September 2020 as chief officer. The occurrence drill was the first free-fall lifeboat drill in which he had participated on the Blue Bosporus.
The third officer held a Master Mariner certificate of competency issued by the Republic of the Philippines in 2019 and endorsed by the Republic of Panama in 2020. He had worked as a third officer on different types of vessels since 2010 and had been working for Apollonia Lines S.A. as third officer on the Blue Bosporus since 16 March 2020. Before the occurrence drill, the third officer had participated in one other lifeboat drill on the Blue Bosporus (held on 11 August 2020), during which he was responsible for preparing the lifeboat with 2 able seafarers under the supervision of the chief officer at the time.
One of the able seafarers held an Able Seafarer Deck certificate issued by the Republic of the Philippines in 2015 and endorsed by the Republic of Panama in 2020. He had worked as an ordinary seafarer on bulk carriers owed by Apollonia Lines S.A. since 2016 and had been working as an able seafarer for Apollonia Lines S.A. since 15 March 2020. He joined the Blue Bosporus on 16 March 2020. Before the occurrence drill, he had participated in the 11 August 2020 Blue Bosporus lifeboat drill, during which he assisted the third officer along with another able seafarer.
The other able seafarer held an Able Seafarer Deck certificate issued by the Republic of the Philippines in 2014 and endorsed by the Republic of Panama in 2019. He had worked as an able seafarer on bulk carriers since 2016 and had been working for Apollonia Lines S.A. since 2019. He joined the Blue Bosporus on 15 September 2020. The occurrence drill was his first lifeboat drill on the Blue Bosporus.
1.9 TSB post-occurrence inspection
Following the occurrence, the TSB laboratory examined the slings and the recovered crimp sleeves, as well as the brackets and bolts used to secure the aft slings to the aft portion of the lifeboat.
1.9.1 Slings
The 4 wire ropes of the slings were made of austenitic stainless steel. The investigation could not determine the exact grade of this material; however, it is more complex than basic AISI (American Iron and Steel Institute) 304 grade and contains small additions of copper, molybdenum, and aluminum. The wire ropes were in good condition, with no broken wires, wear, or corrosion observed.
1.9.1.1 Crimp sleeves
The crimp sleeves on the slings were also made of an austenitic stainless steel similar to AISI 304 grade steel. They were about 9 cm in length and were painted. After the occurrence, some of the crimp sleeves remained on the slings. The TSB recovered these crimp sleeves, as well as a broken portion of the aft starboard crimp sleeve (Figure 10).

The TSB laboratory removed most of the paintFootnote 8 from these crimp sleeves using commercial paint-stripping paste. A close visual examination of the crimp sleeves identified that the sleeves on the aft port sling had small cracks, the largest of which was approximately 1 cm in length. The cracks extended inward from the outer edges of the crimp sleeves. Similar cracks were visible on the broken portion of the aft starboard crimp sleeve. Figure 11 shows some of the cracks on one end of the aft starboard crimp sleeve.
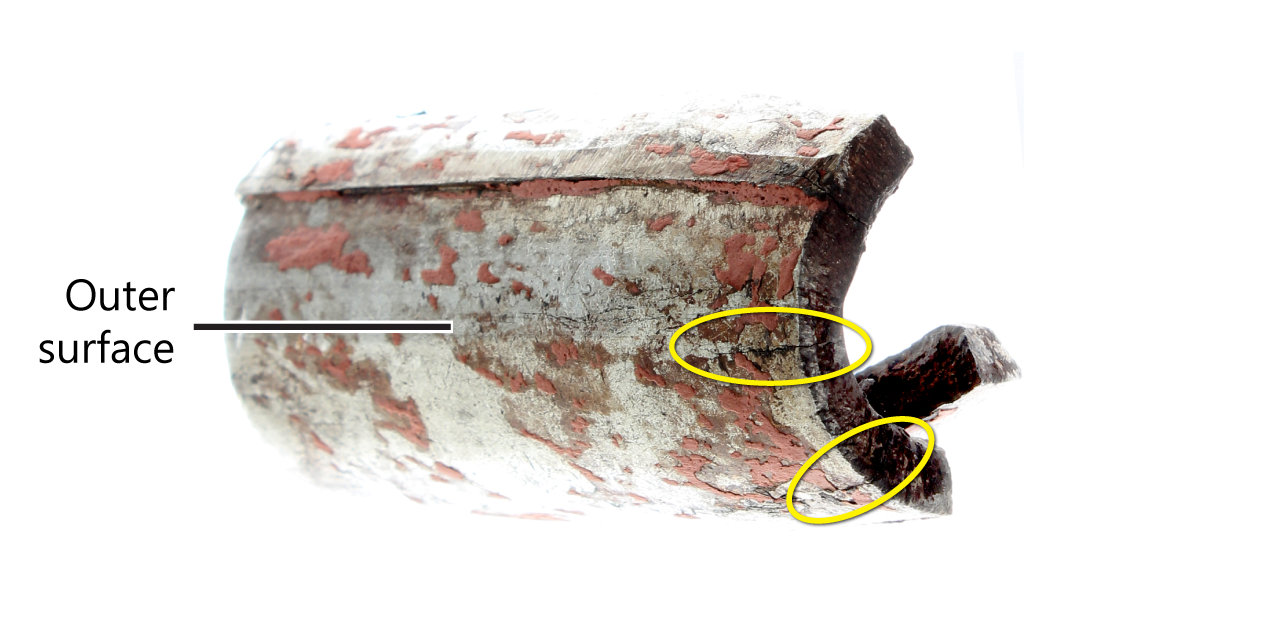
The TSB laboratory also examined the inner surface of the aft starboard crimp sleeve and the fracture surfaces created when it broke. Over 90% of the fracture surface on the upper side of the sleeve had an aged, corroded appearance. There was a small region of fresh fracture (circled on Figure 12) where a ledge about 3 mm high was visible. The ledge had formed when 2 cracks propagated on different levels. The fracture surface on the lower side of the crimp sleeve (Figure 12) also had an aged, corroded appearance.
The fracture surfaces were examined using a scanning electron microscope. The majority of the surfaces were covered by a thick corrosion scale with a dried mud appearance. Analysis of this scale showed that it consisted primarily of chromium oxide, with traces of sodium, chlorine, calcium, and sulphur. These elements are consistent with corrosion resulting from contact with sea water or humid sea air. Some corrosion was also observed on the inner surface of the crimp sleeve.
1.9.1.2 Stress-corrosion cracking
The results of the laboratory examination indicated that the failure of the crimp sleeves was due to intergranular stress-corrosion cracking. Stress-corrosion cracking is a type of cracking induced by a combination of stress and a corrosive environment. The cracks can result from stress that is either directly applied or residual. In the case of mechanical splices such as crimp sleeves, residual stress may result from the original pressure applied on the crimp sleeve to crimp it to the wire. Crimp sleeves may also come under directly applied stress if they are load-bearing. Stress-corrosion cracking is a progressive failure process that develops over time, but it may eventually cause the sudden and catastrophic failure of a component. Intergranular stress-corrosion cracking is a variant of this process that occurs when the cracks follow grain boundaries in the material. It is typical for austenitic stainless steel.
1.9.2 Aft bracket and bolts
The brackets used to attach the aft slings to the lifeboat were made of aluminum bronze. Aluminum bronzes have a strength similar to low alloy steels, and they are typically resistant to corrosion. Post-occurrence examination of the bracket indicated that it had bent significantly and had fractured at the middle bolt hole.
The bolts were made of austenitic stainless steel similar to the AISI 300 series. Post-occurrence examination of the bolts by scanning electron microscope showed signs that the bolts sheared off as a result of overstress applied when the bracket bent and broke.
1.10 Examination and operational test of lifeboat
According to SOLAS requirements, a lifeboat must be examined and undergo an operational test administered by certified personnel from the manufacturer or from an authorized service provider annually. Lifeboats must also undergo more comprehensive operational testing and examinations every 5 years.Footnote 9
Before the occurrence, Apollonia Lines S.A. had contracted a lifeboat servicing company approved by the Panama Maritime Authority and ClassNK to examine the lifeboat on the Blue Bosporus on 01 November 2020, while the vessel was in drydock. During the examination, the lifeboat servicing company used a checklist to verify the condition of the lifeboat and its various components, including the engine, rudder, release hook system, davit system, and winch system. The checklist did not include verification of the condition of the slings or restraint systems (see section 1.11.5.1). The examination identified no deficiencies, and the lifeboat servicing company issued a certificate of inspection for the lifeboat.
During the examination, the lifeboat servicing company also conducted a dynamic load test that involved suspending the lifeboat from a shore crane using the lifeboat’s slings. The test was performed with weights totalling 5830 kg inside the lifeboat, representing 1.1 times the total mass of the lifeboat when loaded with its full complement of persons and equipment. The slings were attached to the shore crane davit in the manner specified by the manufacturer’s operating instructions, resulting in an approximately even distribution of the load of the lifeboat. The test was completed without incident. There was no record as to whether the slings had ever been load-tested individually.
After witnessing the testing procedure and verifying the lifeboat servicing company’s certificate of inspection, the ClassNK surveyor issued a safety equipment certificate during the renewal survey.
1.11 Safety management system
The ISM Code provides an international standard for the safe management and operation of ships and for pollution prevention. SOLAS Convention vessels are required to establish a safety management system (SMS). An SMS involves individuals at all levels of an organization and promotes a systematic approach to hazard identification, risk assessment, and risk mitigation. It includes a set of documents that a vessel owner or authorized representative prepares with masters and crew to establish procedures, plans, and instructions for managing risk.
1.11.1 Planned maintenance of lifeboat
Apollonia Lines S.A. had a section in its SMS on servicing, maintenance, and testing of lifeboats, launching appliances, and on-load release gear. It included generic checklists for maintenance routines to be carried out weekly, monthly, quarterly, semi-annually, annually, and every 5 years. The checklists for the planned maintenance routines were being completed, as required, by vessel crew and shore staff on the Blue Bosporus. Apart from the semi-annual checklist, which included an item requiring all wire and ropework on the lifeboat to be checked, none of the planned maintenance checklists specifically directed the crew to check the condition of the slings.
1.11.2 Lifting gear and portable appliances maintenance
The SMS included a section about the maintenance of lifting gear and portable appliances. This section specified that all slings must be marked with their safe working load and have a certificate indicating the safe working load or minimum breaking load to which the item has been tested.Footnote 10,Footnote 11
The lifeboat slings were not stamped with a safe working load and had no accompanying certificates or records of inspection. In addition, there were no markings on the slings to indicate who had manufactured them or when.
1.11.3 Inspection of wires and ropes
The SMS included a section about the inspection and replacement of wires, ropes, mooring lines, and mooring tails. This section stated that records should be maintained to indicate the inspection and replacement dates for wires, ropes, and tails. The SMS guided crew to use a wires and ropes inspection log (Appendix B) to document rope inspections. The log required that crew enter the following information for wires and ropes:
- Wire composition and type
- Diameter and length
- Certificate number and year
- Service entry date
- Date of last maintenance
- Renewal interval (years)
- Renewal date
- Present condition (good, replace)
The log noted that wires must be replaced when necessary due to deterioration or according to the number of years shown in the “Renewal Interval” column. For all of the wires and ropes listed in the log, the renewal interval was 5 years. The note also said that inspections were required to be carried out every 6 months.
The log listed the vessel’s mooring lines, the wire ropes used for the on-board cranes, the shipboard ladders, the free-fall lifeboat davit, the rescue boat davit, and the wires and chains on the hatch covers. The log did not list the lifeboat slings.
In the case of mooring lines, the SMS specified that every time a mooring rope or wire is used for mooring operations, it should be examined visually before and after use for wear or distortion, and any defects found are to be reported to the chief officer. All inspection details were to be recorded in the planned maintenance system. The SMS did not specify the same for other wires and ropes.
The SMS also specified that when the vessel was at sea, the vessel’s synthetic mooring ropes must be stowed below deck to avoid prolonged exposure to the elements and sunlight. The ropes were to be coiled on wooden gratings to permit air circulation and drainage. They were not to be stowed near boilers or heaters or against bulkheads or on decks that might reach high temperatures. The SMS did not specify stowage requirements to protect other wires and ropes.
In 2019, the crew completed the wires and ropes inspection log every 3 months. The last wires and ropes inspection log before the occurrence was completed on 30 September 2020.
1.11.3.1 Internal audit
Apollonia Lines S.A. had a process for making an annual internal audit of its SMS. One of the items on the internal audit checklist required the auditor to check the records of regular inspection and testing of lifting devices, including wire slings, cranes, portable and beam chain blocks, pad eyes, and lifting beams. The last internal audit before the occurrence had been conducted on 30 June 2020, when this item was checked as complete. The lifeboat slings were not part of this audit checklist.
1.11.4 Familiarization
During familiarization,Footnote 12 the existing knowledge, skills, and experience of an incoming operator are applied to the specifics of an unfamiliar vessel. When boarding a vessel operated by Apollonia Lines S.A. for the first time, incoming crew members are required to complete a familiarization and handover checklist with the outgoing crew member they are replacing.
The checklist for deck officers and ratings covers
- safety procedures and equipment;
- an initial briefing;
- duties, responsibilities, and job-specific procedures;
- emergency procedures; and
- SMS manual familiarization.
The familiarization and handover checklist is designed to be completed in about 12 hours. However, in 2020, the time allotted to complete the familiarization and handover checklist was reduced to about 6 hours to limit contact between incoming and outgoing crew members in order to reduce the risk of transmission of COVID-19.Footnote 13
1.11.5 Lifeboat drills
The SMS included a procedure for simulated launching of the lifeboat. There were also 2 other documents on the Blue Bosporus that included information about simulated launching of the lifeboat: the lifeboat manufacturer’s manual (stored on the bridge), and the davit manufacturer’s instructions for simulated launching (stored next to the coxswain’s seat in the lifeboat).
The company’s SMS procedure for simulated launching stated that “[…] free-fall lifeboat drills should be carried out as per the manufacturer’s instructions […].”Footnote 14 The SMS procedure for a simulated launching involved ensuring that the restraining devices are installed, unlatching the release hook, allowing the lifeboat to travel down the ramp to the distance specified in the manufacturer’s instructions (5 to 20 cm), and then returning the lifeboat to its stowed position. It did not include a procedure that involved lowering the lifeboat into the water using the davit. The crew had therefore developed a practice for drills with davit launching that did not use an additional restraining device, though the device was recommended by the lifeboat manufacturer’s manual. The practice involved attaching the slings to the spreader bar, entering the lifeboat, operating the release handle while standing beside the coxswain’s seat, and then exiting the lifeboat once the release hook unlatched and the lifeboat had moved forward about 20 cm. At this point, the lifeboat was lowered to the water using the davit. This practice had been used successfully during the previous lifeboat drills on 01 January 2020, 06 March 2020, and 11 August 2020.
During the 11 August 2020 drill, the chief officer at the time went to the launching platform with the third officer and 2 able seafarers where he supervised the preparations. The third officer and the 2 able seafarers prepared the lifeboat for davit launching. When it was time to unlatch the release hook, the chief officer entered the lifeboat and activated the release handle without first having secured himself into the coxswain’s seat. The third officer observed this process and did the same during the occurrence.
1.11.5.1 Additional restraining devices
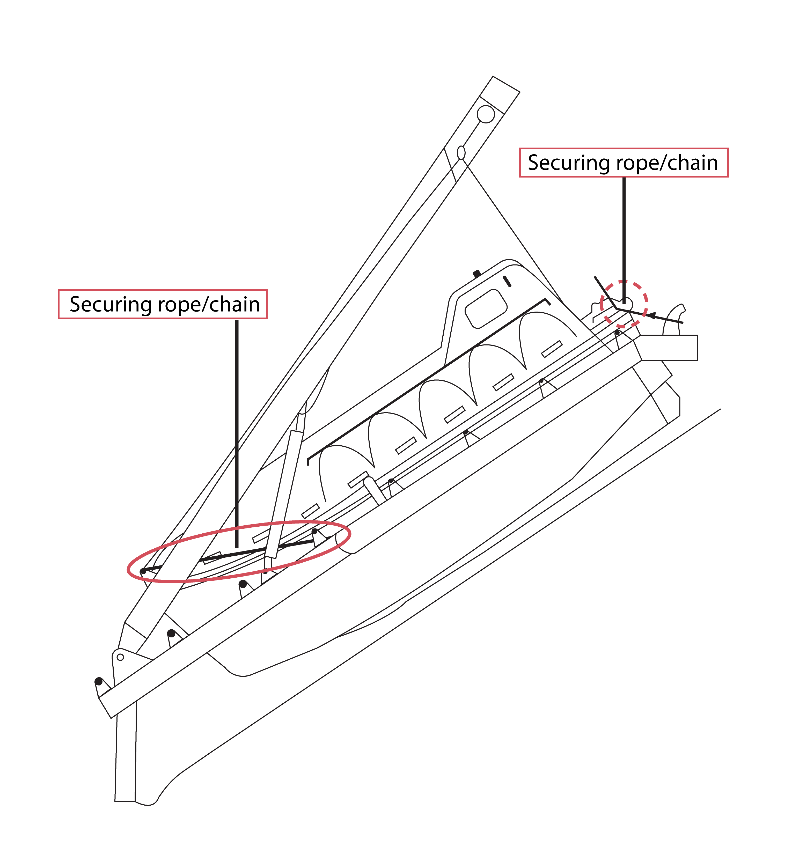
The lifeboat manufacturer’s manual specifies that during a release test without launching (i.e. a simulated launching), the lifeboat should be additionally secured with applicable ropes or chains. The securing points for these ropes or chains are different from the points used for the slings. The manual recommends that the ropes or chains be secured from the forward hoisting shackle downwards and aft to the launching way on either side of the lifeboat and/or through cut-outs in the aft release arrangement to shipside retaining devices (Figure 13). This provides additional restraining devices with secondary securing points in the event that the slings fail.
The davit manufacturer’s instructions did not mention the additional restraining devices. The SMS procedure specified the simulated launching should be carried out as per the lifeboat manufacturer’s instructions and the procedure in the SMS. The SMS procedure was a verbatim copy of guidance from an IMO circular issued in 2009, which described a typical simulated launching sequence and indicated that crew should “ensure that the restraining device(s) provided by the maker for simulated launching is (are) installed and secure […].”Footnote 15 It did not explicitly mention the additional restraining devices identified in the lifeboat manufacturer’s manual. There was also nothing in the SMS to identify whether additional restraining devices were available on the Blue Bosporus and where they were stored.
1.11.5.2 International Maritime Organization circulars on lifeboat drills
In 2009, the IMO issued a circular regarding measures to prevent accidents with lifeboats. The circular mentioned an unacceptably high number of accidents in which crew were being injured, sometimes fatally, during lifeboat drills.Footnote 16 The circular recommended that when a lifeboat is free-fall launched as part of a drill, it “should be carried out with the minimum personnel required to manoeuvre the boat in the water and to recover it.”Footnote 17
In 2017, the IMO issued another circular regarding drills using lifeboats. This circular also recommended that free-fall lifeboat drills be carried out “with the minimum personnel required to manoeuvre the boat in the water and to recover it,”Footnote 18 and reiterated that restraining devices provided by the manufacturer should be installed.
In response to these circulars, Apollonia Lines S.A. verbally informed its crews that they were required to exit the lifeboat after having unlatched the release hook, before the lifeboat was lowered to the water using the davit. The SMS procedure for simulated launching did not reflect this guidance.
1.12 Supervision
Supervision is a key aspect of safety during drills. When a supervisor is required to take an active role in a drill, the supervisor’s attention becomes divided between supervision and specific tasks at hand, resulting in a restricted capacity to oversee the whole operation effectively.
Because there is so much information available in the environment, it is necessary for people to filter out less important information in order to attend to the important information. However, while people can switch their attention rapidly from one information source to another, they can attend well to only one information source at a time. Trying to multi-task leads to a decrease in performance on each task.
When supervising a lifeboat drill from the lifeboat launching platform, the supervisor’s function is to oversee the crew performing the drill. This is usually the role of the chief officer. The second officer, third officer, and the 2 able seafarers are responsible for preparing and launching the lifeboat. The master is responsible for the overall conduct of the drill.
On the day of the occurrence, the chief officer asked the third officer to prepare the lifeboat for release as well as supervise the 2 able seafarers on the lifeboat launching platform. The request was made because the second officer was not present for the drill, and the chief officer had joined the vessel 2.5 months earlier and was unfamiliar with the specifics of a lifeboat drill on the Blue Bosporus. The third officer’s workload then involved directing the 2 able seafarers assigned to the drill, while performing critical tasks himself. The third officer was therefore required to switch his focus between his own tasks and his supervisory role directing and monitoring the 2 able seafarers.
1.13 Similar occurrences
The TSB has investigated several occurrences involving lifeboat launching appliances and is aware of others that have occurred internationally (Appendix C).
1.14 TSB Watchlist
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada’s transportation system even safer.
Safety management is a Watchlist 2020 issue. As this occurrence demonstrates, despite Apollonia Lines S.A. having an audited SMS, it was missing key safety information, such as a complete procedure for a drill that involved lowering the lifeboat to the water using the davit. The ongoing audits of the SMS on the Blue Bosporus had not identified this gap.
|
ACTIONS REQUIRED Safety management will remain on the Watchlist for the marine transportation sector until:
|
1.15 TSB laboratory report
The TSB completed the following laboratory report in support of this investigation:
- LP014/2021 – Examination of Failed Lifeboat Launching Assembly
2.0 Analysis
The Blue Bosporus’s lifeboat unexpectedly fell after the slings that were attaching it to the davit failed. The analysis will focus on the condition of the slings, the way the slings were attached to the hooks, Apollonia Lines S.A.’s safety management system (SMS), and the use of additional restraining devices.
2.1 Condition of slings
The slings were used about every 3 months to secure the lifeboat to the davit during drills. Once the release hook was unlatched, only the slings prevented the lifeboat from freefalling, making the condition of the slings critical to the safety of any individuals in the lifeboat.
The eyes of the slings were secured with crimp sleeves that had weakened over time as a result of intergranular stress-corrosion cracking. The cracks likely resulted from a combination of exposure to the elements, residual stress placed on the crimp sleeves when they were originally crimped onto the sling wires, and load-bearing stress placed on them each time they were used to hold the weight of the lifeboat.
Finding as to causes and contributing factors
The crimp sleeves on the Blue Bosporus’s lifeboat slings had weakened over time as a result of intergranular stress-corrosion cracking.
2.2 Attachment of slings to hooks
The slings were intended to be attached to the hooks in a way that allowed the shock load created by the release of the lifeboat to be absorbed by all 4 of the slings in an approximately equal manner.
However, in this occurrence, the launching crew members unknowingly deviated from the instructions outlined in the manufacturer’s manual when they placed both the oval ring and the eye of the aft starboard sling into the starboard hook. This caused the active length of the aft starboard sling to be shorter than the other slings. As a result, when the lifeboat was released, the shock load concentrated entirely on the aft starboard sling.Footnote 19 This sling was held together by a weakened crimp sleeve which, in combination with the concentrated force, caused the sling to fail.
Once the aft starboard sling failed, the shock load shifted to the other slings, causing the crimp sleeves on the 2 forward slings to also fail. The load then shifted to the remaining aft port sling and its sleeve which, although cracked, remained intact. However, the bolts and the aft port bracket could not withstand the load and were pulled off the lifeboat by the force on the aft port sling.
Finding as to causes and contributing factors
The manner in which the slings were attached to the hooks caused the load to concentrate on the aft starboard sling. This, in combination with the weakened crimp sleeves, caused the sequential failure of the slings and the aft port sling bracket.
2.3 Safety management system
Risk management under an SMS is a continuous process of identifying hazards, analyzing and mitigating risks, and verifying that mitigation measures are effective. Although Apollonia Lines S.A. operated under an audited and certified SMS, the investigation identified some gaps in safety management related to procedures to verify the condition of the slings and to conduct a davit-launched lifeboat drill. Gaps in the supervision of the drill were also identified.
2.3.1 Verification of slings
Because the slings were integral to the safety of occupants inside the lifeboat during drills, it was critical that Apollonia Lines S.A. have maintenance routines, replacement schedules, and documentation in place to verify the slings’ adequacy.
Although Apollonia Lines S.A. had regular maintenance routines in place to verify the condition of the lifeboat and its launching appliances, the checklists for these routines did not prompt the crew to specifically check the condition of the slings. The lifeboat davit and launching appliances had last been inspected and tested in November 2020, 1 month before the occurrence, by a lifeboat service company approved by the classification society. However, the checklist used during this inspection did not prompt a visual inspection of the slings, and the small cracks in the crimp sleeves went unidentified. As well, during the dynamic load testing of the lifeboat in drydock, the slings were correctly attached to the hooks, so there was no shock load acting on any individual sling.
Apollonia Lines S.A. had a wires and ropes inspection log to track key safety information about lifting equipment on the vessel, including service entry date, renewal intervals, and renewal dates. However, the slings were not included in this log. Although on-board internal audits verified records of regular inspection and testing of various on-board lifting appliances, they did not verify that every lifting appliance on the vessel was documented in the wires and ropes inspection log. Without any vessel documentation about the slings, it was not possible to determine how long the slings had been in use.
Internationally, there are requirements for lifting appliances and loose gear used during dock work. As part of these requirements, items are required to be inspected before use, regularly tested, and marked with a safe working load. However, these requirements apply specifically to dock work and do not address lifting appliances associated with life-saving equipment. Although the International Convention for the Safety of Life at Sea requires lifeboats to undergo periodic examinations and operational tests and requires verification of various components associated with lifeboats, life rafts, and fast rescue boats, it does not specifically address slings associated with free-fall lifeboats. This means that there is no international requirement for free-fall lifeboat slings to be verified periodically, inspected before use, and marked with the safe working load.
Finding as to risk
In the absence of any international guidance requiring free-fall lifeboat slings to be verified periodically, inspected before use, and marked with a safe working load, there is a risk that this critical equipment will be overlooked during inspections or its safe limits will be exceeded, leading to an accident.
2.3.2 Crew practice during the lifeboat drill
Apollonia Lines S.A.’s SMS contained 1 procedure related to free-fall lifeboat drills. This was a procedure for simulated launching. The crew did not have a complete procedure for a drill that involved launching the lifeboat into the water using the davit. This type of drill included additional steps that were not covered by the procedure for simulated launching.
Although the first steps of the simulated launching described in the SMS, including the use of additional restraints as recommended by the manufacturer, could apply to launching the lifeboat into the water using the davit, the crew had to rely on their own judgment to complete the remainder of the launching steps. Incomplete procedures may lead to confusion and adaptation as the crew is likely to improvise based on what seems the most efficient to them, not based on what is the safest.
Without a complete procedure, the crew followed an undocumented practice for conducting the drill. The practice involved a crew member entering the lifeboat, operating the release handle, and then exiting the lifeboat once the release hook unlatched and the lifeboat had moved forward, at which point the lifeboat would be lowered to the water using the davit. The practice had been used successfully in the previous drill on 11 August 2020, in which the third officer and one of the able seafarers were participants. It was then repeated by the third officer during the occurrence drill.
However, this practice exposed the crew members involved in the drill to risk because it did not adequately protect against premature release, or address the need for the crew to secure themselves in the lifeboat before unlatching the release hook. There had been no assessment of the risk associated with standing unsecured in the lifeboat when it was suspended by its slings. Notwithstanding the instructions in the lifeboat manual and davit manual guiding crew members to secure themselves in the lifeboat, the crew involved in the occurrence drill did not recognize the risk of standing unsecured in the lifeboat, nor was there anyone supervising them who was aware of this risk.
Finding as to causes and contributing factors
Without a complete procedure for conducting a drill that involved launching the lifeboat using the davit, the crew had developed an informal practice that did not address the risk of standing unsecured in the lifeboat, which led to the serious injury of 2 crew members when the lifeboat fell.
In 2009 and 2017, the International Maritime Organization issued circulars indicating that lifeboat drills should be conducted with the minimum personnel required due to a high number of accidents. While Apollonia Lines S.A. verbally told its crew to conduct drills without the crew inside the lifeboat when it was being lowered into the water using the davit, this guidance was not documented in a procedure.
2.3.3 Supervision
Supervision is a key element of safety. To be effective, it must be performed by individuals with sufficient experience and training to recognize risks to safety. The effectiveness of supervision is increased when a supervisor’s role is dedicated only to supervising, which avoids distraction due to multi-tasking.
Although the lifeboat drills usually included the chief officer as supervisor and the second officer as a participant, in this occurrence, the third officer was performing their tasks as well as his own. The third officer had been part of a lifeboat drill only once before on this vessel. He was performing and supervising the drill based on his memory of the previous drill. Because the third officer was performing the roles of the other 2 crew members as well as his own, his attention was divided. The 2 able seafarers involved in the drill also had little experience with free-fall lifeboat drills on the Blue Bosporus. One had participated in the 11 August 2020 drill alongside the third officer, and the other had never participated in a lifeboat drill on the Blue Bosporus before. The relative inexperience of the 2 able seafarers increased the level of supervision required.
All 3 of the crew members involved in the drill had joined the vessel in 2020, when Apollonia Lines S.A. had reduced the time spent on familiarization in order to limit contact between incoming and outgoing crew members and thereby reduce the risk of COVID-19 transmission. Since the familiarization time was reduced, critical information had to be presented more quickly and more superficially than usual, leaving less time for the incoming crew to understand and memorize the information. Increased supervision was required to compensate for any gaps in familiarization.
Because supervision was provided by an officer who had limited prior involvement in lifeboat drills on the Blue Bosporus and whose attention was divided between his own tasks and those of 2 other crew members, opportunities to identify hazards that affected the safety of the drill were reduced. The incorrect configuration of the aft starboard sling in the hook, the precarious position of one of the able seafarers, and the risk of being unsecured inside the lifeboat went unnoticed.
Finding as to risk
If supervisors are required to take an active role during safety critical tasks such as lifeboat drills, their attention will be divided and they will be less able to attend to all aspects of the task, increasing the risk that safety critical items will not be identified in time to prevent an accident.
2.4 Additional restraining devices
Although the lifeboat manufacturer’s manual recommended the use of additional restraining devices consisting of ropes or chains during a simulated launching, the davit manufacturer’s manual did not mention this. The vessel’s SMS mentioned the use of additional restraining devices by reference to manufacturer guidance only. Moreover, there was no information in the SMS as to whether additional restraining devices were available on the Blue Bosporus and, if so, where they were stored.
An additional restraining device ensures redundancy and thereby safeguards against single-point failure. In a case such as this, where the slings unexpectedly failed, an additional restraining device can provide an extra defence to protect crew members.
Finding as to causes and contributing factors
There was no additional restraining device in use to protect the crew on the Blue Bosporus from falling when the slings failed.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- The crimp sleeves on the Blue Bosporus’s lifeboat slings had weakened over time as a result of intergranular stress-corrosion cracking.
- The manner in which the slings were attached to the hooks caused the load to concentrate on the aft starboard sling. This, in combination with the weakened crimp sleeves, caused the sequential failure of the slings and the aft port sling bracket.
- Without a complete procedure for conducting a drill that involved launching the lifeboat using the davit, the crew had developed an informal practice that did not address the risk of standing unsecured in the lifeboat, which led to the serious injury of 2 crew members when the lifeboat fell.
- There was no additional restraining device in use to protect the crew on the Blue Bosporus from falling when the slings failed.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- In the absence of any international guidance requiring free-fall lifeboat slings to be verified periodically, inspected before use, and marked with a safe working load, there is a risk that this critical equipment will be overlooked during inspections or its safe limits will be exceeded, leading to an accident.
- If supervisors are required to take an active role during safety critical tasks such as lifeboat drills, their attention will be divided and they will be less able to attend to all aspects of the task, increasing the risk that safety critical items will not be identified in time to prevent an accident.
4.0 Safety action
4.1 Safety action taken
4.1.1 Apollonia Lines S.A.
Apollonia Lines S.A. took the following steps after the occurrence:
- replaced the failed sling assembly, including the failed lifting brackets, with a newly manufactured, load tested, and certified sling assembly and brackets;
- included the lifeboat sling assembly in the Blue Bosporus’s wires and ropes inspection log;
- sent safety management system circular 05/2020 to all vessels operating under Apollonia lines S.A. the day after the accident. This circular requested that an extra safety meeting be carried out with all crew participating in order to update them on the occurrence and avoid a recurrence.
The circular reminded crews to ensure that
- all information about the maintenance of lifeboats and associated equipment is available on board;
- all personnel carrying out inspections and maintenance of lifeboats and associated equipment are fully trained and familiar with their duties;
- the maintenance of lifeboats and associated equipment is carried out in adherence with approved practices;
- health and safety requirements are applied to drills in the same way that they are to real procedures;
- lifeboat drills are conducted in accordance with applicable International Convention for the Safety of Life at Sea (SOLAS) regulations;
- any personnel carrying out maintenance or repair are qualified for the job;
- lifeboat inspections are regular and thorough;
- all equipment is easily accessible and durable in rough conditions; and
- all tests for safety and life-saving equipment are conducted to International Maritime Organization guidelines.
In addition, Apollonia Lines S.A.
- carried out an unscheduled internal audit of the Blue Bosporus on 05 and 06 December 2020;
- completed an incident investigation report, which was sent to all vessels and masters operating under Apollonia Lines S.A.;
- established that the slings and wires associated with the lifeboat be replaced during the lifeboat’s 5-year dynamic load testing regardless of their condition; and
- established an annual safe working test of the slings by an authorized lifeboat technician.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A ‒ Area of the occurrence
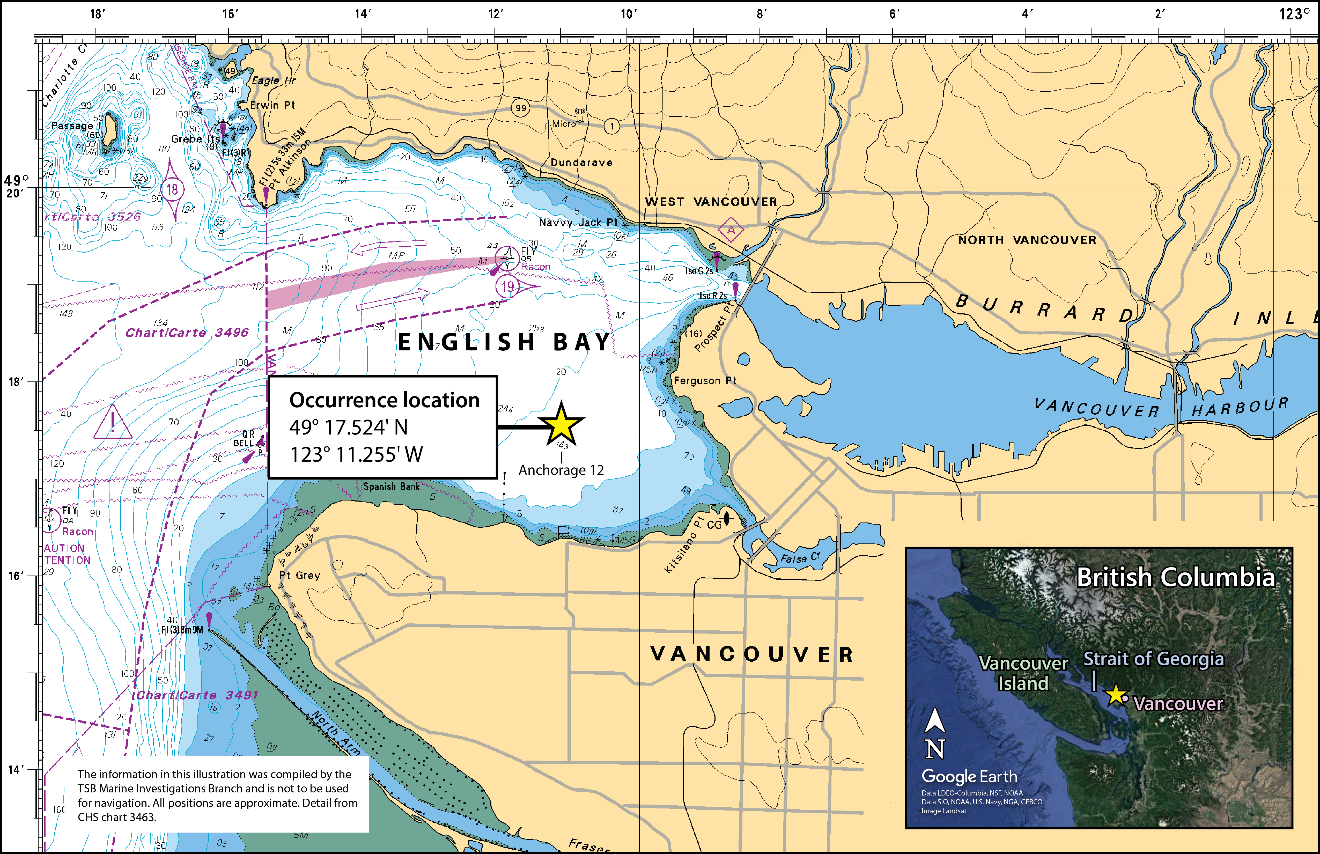
Source of inset image: Google Earth, with TSB annotations
Appendix B ‒ Wires and ropes inspection log from 30 September 2020 inspection
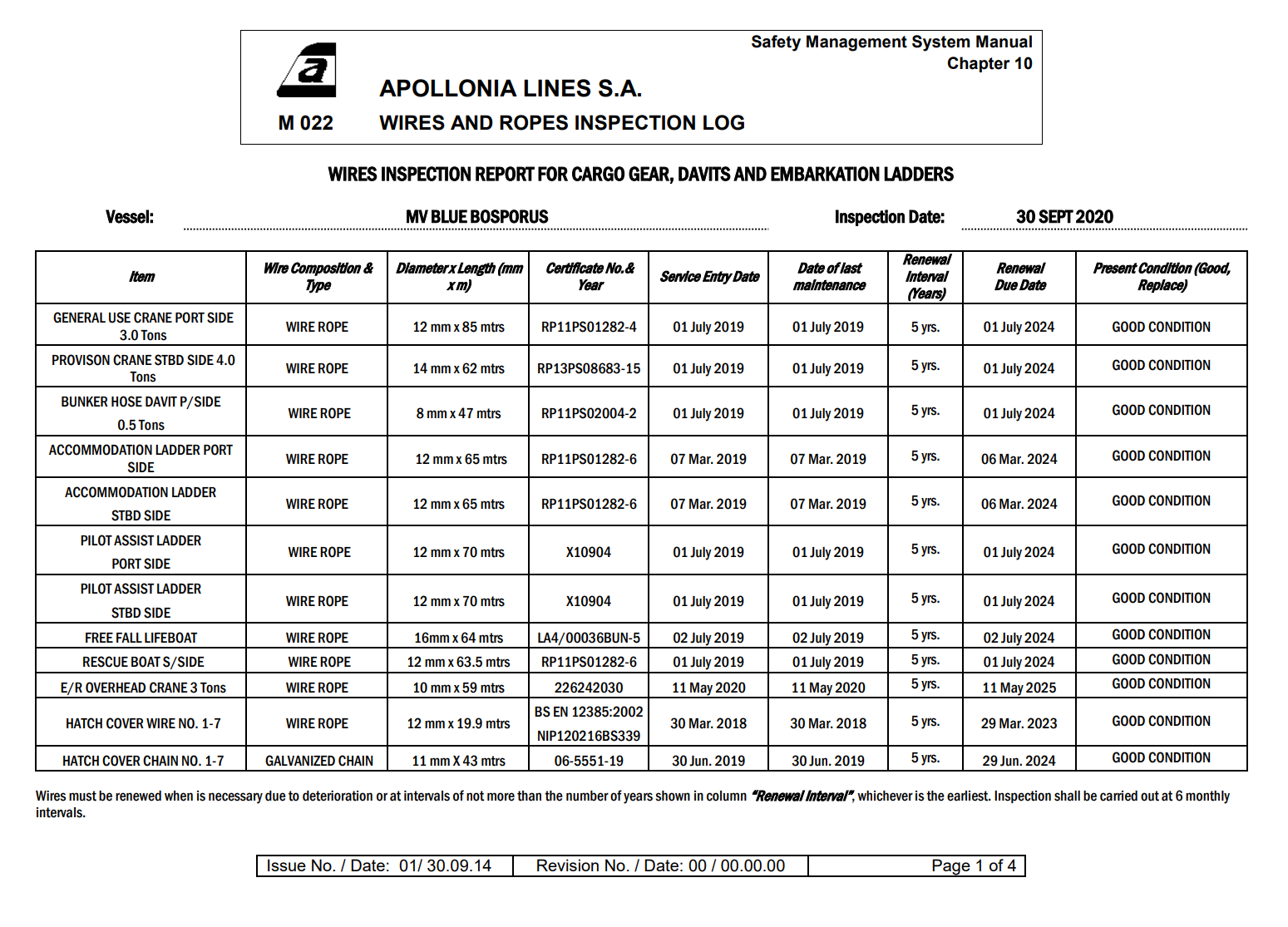
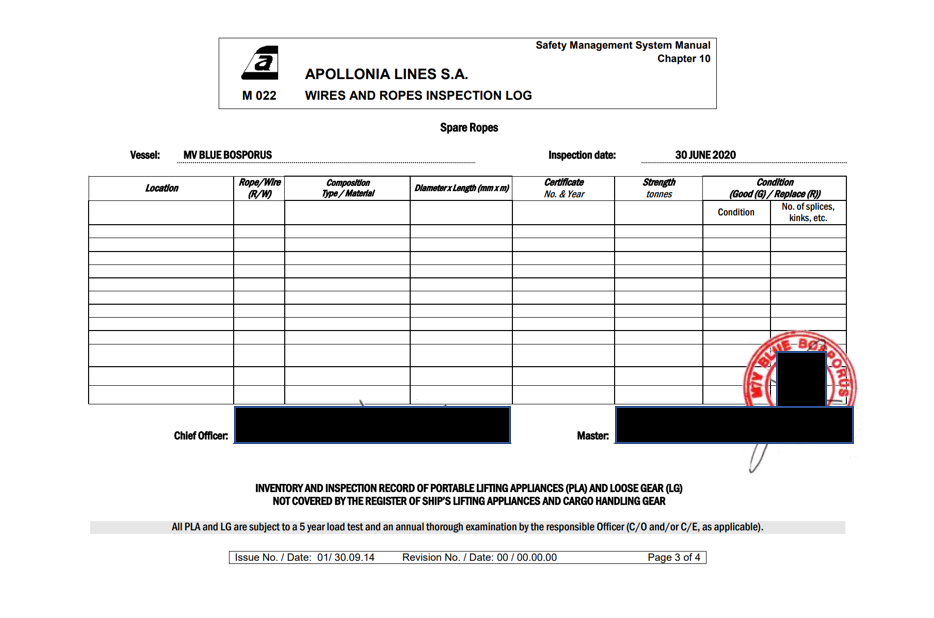
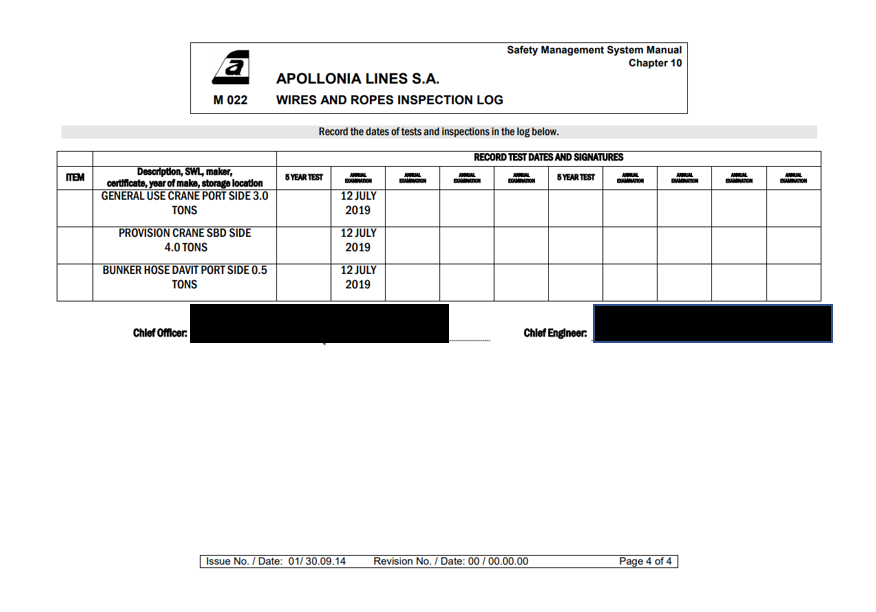
Source: Apollonia Lines S.A.
Appendix C – Similar occurrences
International occurrences
On 08 July 2021, following an occurrence involving a failed wire rope termination that resulted in extensive damage to equipment, the U.S. Coast Guard issued a safety alert addressing the importance of verifying the condition and manufacturing of wire rope terminations in various systems that use wire rope in a load-handling capacity (e.g., life-saving appliances, cranes, lifting slings).Footnote 20
In January 2020, in response to serious accidents involving lifting slings encased in plastic sheathing on free-fall lifeboats, the Port State Control committee established under the Tokyo Memorandum of Understanding issued a safety bulletin. The safety bulletin noted that the use of plastic sheathing can restrict visual inspection of the wire ropes and prevent routine maintenance and surveys from being carried out effectively. The bulletin also noted that investigations into the failure of slings had found that the slings parted under normal operational load as a result of significant weakening from undetected internal corrosion, even though regular inspections were reportedly being carried out.Footnote 21
On 14 April 2014, following a lifeboat occurrence involving the bulk carrier Da Dan Xia, where the lifeboat fell while it was being recovered as a result of the failure of its lifting slings, the Transport Accident Investigation Commission (TAIC) for New Zealand conducted an investigation. The TAIC found that corrosion had gone undetected because of the presence of plastic sheathing that encased the wire rope, meaning neither the crew nor the various surveyors tasked with inspecting the launching system could inspect and maintain the rope as required. TAIC recommended that the manufacturer of the lifeboat and lifting slings cease the practice of using plastic sheathing and inform owners and operators with this system of the dangers.Footnote 22
On 15 April 2011, following a lifeboat accident during a launching drill that involved 2 fatalities and 1 serious injury, the China Maritime Safety Administration submitted a “lessons learned” document to the International Maritime Organization that highlighted safety issues related to the connection between the lifeboat and the davit falls (in the area of the suspension block and the swivel screw). The lessons learned document indicated that “specific requirements are provided for lifeboat maintenance by SOLAS. However, in the actual process, some equipment has been ignored by all relevant parties or has not drawn enough attention, resulting in a greater safety risk in the use of lifeboats.”Footnote 23
Canadian occurrences
M18P0144 (Spirit of Vancouver Island) ‒ On 19 June 2018, the starboard forward rescue boat on the passenger ferry Spirit of Vancouver Island slipped off the hook during hoisting after completion of a repair on its davit. At the time, there were 7 people on board the rescue boat. The rescue boat fell into the water, and damage to both the rescue boat and its davit hook were reported. No injuries were reported.
M18P0087 (Queen of Cumberland) ‒ On 18 April 2018, the crew on the roll-on/roll-off passenger ferry Queen of Cumberland were using an on‑board davit to hoist the vessel’s rescue boat out of the water during a drill when the hoist cable parted. The cable parted as it came out of the davit sheave and became pinched between the top of the sheave flange and the cable keeper. There were 2 crew members in the rescue boat at the time. The rescue boat and the 2 crew members fell approximately 11 m to the water. Both crew members were injured, one of them seriously, and the rescue boat was damaged.
M17A0391 (Northern Ranger) ‒ On 11 October 2017, the starboard lifeboat on the passenger ferry Northern Ranger was undergoing operational testing at the dock when its forward release hook failed. While the crew members were lifting the lifeboat to the vessel’s embarkation deck, the forward release hook suddenly released and the lifeboat swung downward, bow first, and hung over the water from the aft release hook and fall. Four crew members were on board the lifeboat at the time of the occurrence. All 4 crew members were recovered, and their injuries were treated in hospital.
M06L0063 (Sea Urchin) ‒ On 22 May 2006, the starboard lifeboat was being recovered on the bulk carrier Sea Urchin when the aft hook-release gear mechanism opened. The forward mechanism, unable to take the full load, also opened. The lifeboat then fell 11 m, stern-first, into the sea, fatally injuring 1 of the 5 crew members on board.
M00W0265 (Pacmonarch) – On 26 October 2000, the crew began launching the port lifeboat on the Pacmonarch for a run ashore. The lifeboat was of the davit-launched, totally enclosed type, and was fitted with on-load release hooks. Four crew members boarded the lifeboat while 2 others on the vessel removed the securing pins at the davits to prepare for the launch. Soon after the davits hit their stops and the lifeboat was about 15 m above the sea, the aft hook separated from the aft suspension ring of the falls. Suspended from the forward hook, the lifeboat swung downwards, at which point the forward hook opened and the lifeboat fell stern-first into the sea. Three of the 4 people in the lifeboat were fatally injured.