Non-main-track train collision
Canadian National
Hump assignment
Mile 145.20, Sprague Subdivision
Symington Yard, Winnipeg, Manitoba
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 13 February 2007, a Canadian National hump yard assignment was performing switching operations at Symington Yard (Mile 145.2 of the Sprague Subdivision) in Winnipeg, Manitoba. While travelling westward at approximately 6 mph on track ER-08, the hump yard assignment sideswiped Canadian National train L53241-13, which was outbound on track ER-04. Four cars from the hump assignment derailed. A total of nine cars were damaged. No dangerous goods were involved and there were no injuries.
Ce rapport est également disponible en français.
Factual information
The accident
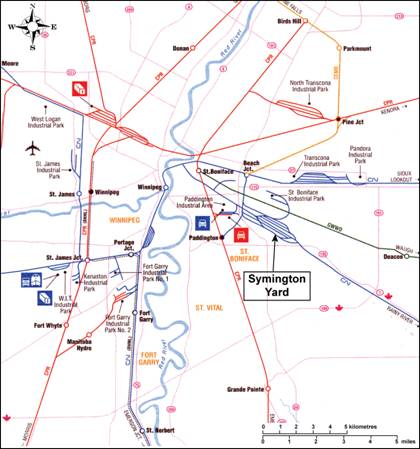
On 13 February 2007, a Canadian National (CN) hump yard assignment (the assignment), controlled by a single Beltpack® operator (the operator), was performing routine switching operations at Symington Yard in Winnipeg, Manitoba (see Figure 1).
At approximately 1400 central standard time,Footnote 1 the operator, who was controlling a four-unit locomotive consist, entered the east end of track ER-08 and coupled to a cut of approximately 100 cars. During the coupling process, a company motor vehicle, driven by a co-worker, arrived and stopped alongside the lead locomotive. Assuming that the operator would be riding the point of the movement to the next switching location, the driver offered the operator a ride to the next location. The operator turned, walked towards the motor vehicle and initiated the train movement using the operator control unit (OCU) of the Beltpack®. The operator then entered the motor vehicle and the driver drove eastward in advance of the movement. While travelling in the motor vehicle, the operator continued to control the assignment.
Shortly after the movement was first initiated, the operator and driver, who were monitoring the assignment using the motor vehicle mirrors, realized that the movement was travelling away from them in the westward direction, instead of the intended eastward direction. The operator immediately placed the OCU into the stop position. Shortly after the movement came to a stop, the operator was notified that his assignment had collided with outbound train L53241-13 (the train).
Train L53241-13, which was made up of 3 locomotives and 108 cars, was approximately 6600 feet in length and weighed 14 727 tons. At the time of the occurrence, the train was on track ER-04 and was departing Symington Yard in the westward direction. The train crew members had not experienced any problems until they were informed that a hump assignment had collided with their train.
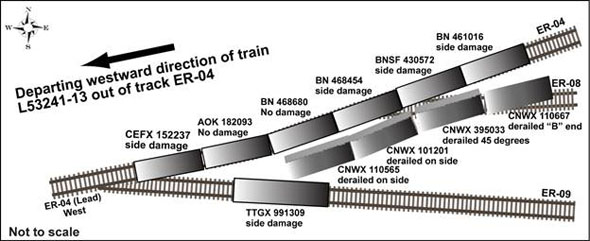
Subsequent inspection determined that, as a result of the train collision, four empty covered hopper cars at the west end of the assignment had derailed. The first two derailed cars (CNWX 110565 and CNWX 101201) were on their side, the third car (CNWX 395033) came to rest at a 45-degree angle and the fourth car (CNWX 110667) was upright with the “B” end derailed. On the outbound train, three covered hopper cars loaded with grain (BN 468454, BNSF 430572 and BN 461016) and one empty covered hopper car (CEFX 152237) sustained side damage during the collision. In addition, a stationary empty auto rack car (TTGX 991309), which was part of a cut of cars stored in adjacent track ER-09, was damaged (see Figure 2).
At the time of the occurrence, the sky was clear and the temperature was −27°C . The wind was 11 km/h producing a wind chill of approximately −30°C.
On 10 February 2007, conductors at CN went on strike across CN's rail network in Canada. Most conductors returned to work on 26 February 2007 when the strike was suspended. The conductors were legislated back to work on 18 April 2007. To maintain ongoing train operations during the strike, management personnel assumed the operating positions for the conductors.
Crew information and qualifications
The hump assignment was being controlled by a single Beltpack® operator. The operator was a rules-qualified CN manager who was filling in for operating crews during the strike. Before the disruption, the operator had worked for three years as a motive power planner. Although the operator had no previous Beltpack® experience, he had worked four shifts of switching at a different yard in the previous three years and, in 2004, he had worked for 30 days as a hostler helper during a previous strike. On 31 January 2007, in preparation for the strike, the operator had received an abbreviated two-day Beltpack® training course.
The crew on the departing train consisted of a locomotive engineer and a conductor. The locomotive engineer had 20 years' experience. The conductor was a CN manager who was filling in during the strike. Both crew members were rules-qualified.
All crew members met fitness and rest requirements in accordance with existing regulations.
Recorded information
A review of the Beltpack® event recorder download revealed the following:
1414:36 – The assignment coupled onto the standing cut of cars in track ER-08 at a speed of 1.19 mph in a forward direction (westward).
1414:40 – The assignment stopped in track ER-08.
1418:46 – The operator requested a speed of 1.75 mph, which initiated the westward forward movement of the assignment.
1419:14 – The operator requested a speed of 4.00 mph.
1419:16 – The operator requested a speed of 8.00 mph.
1419:32 – The operator requested stop, which initiated braking action on the assignment. The assignment was travelling at 5.95 mph when braking was initiated.
1419:41 – With continued braking action, the speed of the assignment decreased to 2.97 mph.
1420:00 – The assignment stopped. The assignment had travelled a distance of 264 feet from the time the westward movement was initiated.
Track information
At Symington Yard, the east receiving yard is located on the south side of the yard and has nine tracks. This area of the yard is controlled by yard signals and a traffic coordinator in the L Tower. Track ER-04 is the lead track and was the departure track for the train. Track ER-08 is approximately 6500 feet long and intersects track ER-04 at the west end.
In the vicinity of the accident site, the track consisted of 100-pound continuous welded rail, which was laid on double-shouldered tie plates and secured to No. 2 softwood ties with four spikes per tie plate. The rail was box-anchored every third tie. The ballast was crushed rock with a diameter of 1 to 1 1/2 inches. The track was generally in good condition.
Beltpack® operations
Beltpack® technology provides railways with an efficient means of operating yard locomotives using a remote control device. In the late 1980s, this technology was introduced in Canada and was approved by Transport Canada (TC) for yard switching and humping operations. Since its introduction, Beltpack® has become the primary means for locomotive and train control in yard operations.
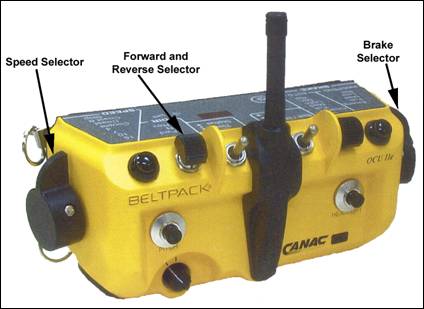
During Beltpack® operations, the operator uses an OCU, which is a small three- to five-pound box attached to the operator's safety vest (see Photo 1). By transmitting radio commands to the locomotive, the OCU permits the operator to remotely activate a number of locomotive controls. The commands are received and processed by a computer on board the locomotive that initiates the appropriate response. The Beltpack® OCU is equipped with a speed selector, a reverse selector and brake selector, which includes an emergency brake feature.
In Canada, Beltpack® operations are performed by conductors. Switching movements operated using Beltpack® normally involve two conductors—one conductor positioned at each end of the movement. At other times, as in this occurrence, one Beltpack® operator performs all the duties.
Section 6 of the CN General Operating Instructions (GOIs) governing Beltpack® operations defines a Beltpack® operator as an operating employee who, through training, experience and knowledge, is qualified to perform switching operations and provide engine movement signals using the Beltpack® technology. The GOIs further state:
Beltpack operation requires full compliance with all Canadian Rail Operating Rules (CROR) and GOI.
While CN had a GOI for Beltpack® operations, it did not have a written instruction or guideline for Beltpack® operators to verify that a movement was travelling in the intended direction. In comparison, Canadian Pacific Railway (CPR) incorporates the manufacturer's job aid, entitled “CANAC Remote Control Locomotive System” (dated 07 June 2005), as a Special Instruction to its GOIs. Section 1.10 states the following:
Immediately after commanding direction and speed, the controlling employee must visually verify that the movement is responding in the requested direction.
Use of motor vehicle to assist with Beltpack® switching operations
CN will occasionally use a motor vehicle to assist with Beltpack® switching operations. When a ride is provided to a Beltpack® operator, it is not uncommon for the operator to control the movement while in the motor vehicle. Currently, neither CN nor TC has guidelines or written procedures governing the use of a motor vehicle to assist with switching operations. In addition, no formal risk assessment was performed before allowing this deviation to normal Beltpack® switching procedure.
In this occurrence, the Beltpack® operator was controlling the movement from the front seat of a motor vehicle driven by another person. The motor vehicle was in advance of and facing away from the assignment. In the switching activities performed by this operator before the occurrence (that is, two 12-hour shifts in the previous two days), the operator had always ridden the point of the movement and had not been assisted by a motor vehicle.
The TSB investigated another accident at Symington Yard where a motor vehicle was used to assist with Beltpack® switching operations. On 17 February 2004, a 15-car derailment occurred when a yard switch was not properly aligned and verified during Beltpack® switching operations (TSB report R04W0035). As a result of this investigation, the Board determined that the location of the Beltpack® operator in a motor vehicle, in advance of and facing away from the movement, left the movement unmonitored and increased the severity of the derailment.
Beltpack® and yard training for unionized employees
For experienced unionized operating employees who are conductor-qualified, which includes training in CROR and Qualification Standards for Operating Crews (QSOC), CN provides 7 to 10 days of Beltpack® training. This training program consists of 3 days of classroom instruction and between 4 to 7 days in the field to become familiar with the Beltpack® equipment.
For less-experienced unionized operating employees who are conductor-qualified, CN provides a 33-day Beltpack® and yard training program. This training program includes 3 days of classroom instruction, 7 days in the field to become familiar with the Beltpack® equipment and 23 days in the field for general yard training working under the direction of a Beltpack®‑qualified yard conductor. Should an employee fail to qualify after completing this 33‑day program, CN will normally provide additional training as required.
Beyond initial Beltpack® training, CN does not provide regular refresher training. The provision of refresher Beltpack® training is not required under the current rail regulations.
Beltpack® and yard training for managers
Not all CN managers were qualified to assume operating roles during the strike. To prepare for the strike, CN provided an abbreviated two-day Beltpack® training course to groups of up to eight management personnel who were identified as potential Beltpack® operators. These managers were selected for the abbreviated training because they were already conductor‑qualified and had some previous operating experience. The two-day course consisted of a day of classroom instruction followed by a half day in the field to become familiar with Beltpack® equipment followed by a test.
The Beltpack® operator in this occurrence was a manager who was given the abbreviated two‑day course. While the operator was conductor-qualified, he did not have any experience working as a Beltpack® operator. During the training course, the operator did not receive any instructions or guidance to visually verify that a movement was responding in the requested direction.
For those management personnel who were CROR-qualified and QSOC-qualified, but had never received any hands-on operational training, CN provided up to two days of basic rail operations instruction on freight car air brake components, knuckles, documentation, written authorities, switching, etc. Because these managers did not receive any training in local operating procedures, they were provided with job aids and contact phone numbers when assistance was needed.
Regulatory overview
TC's Regulation CTC-1987-3 Rail, effective 12 March 1987, outlines the minimum QSOC. This regulation states that a railway company shall establish and provide the necessary training to satisfy the regulation. TC is the regulatory authority that ensures that all core training subjects are contained in the railway's training material. After the initial review and approval of the material, the regulator is not required to conduct further review. According to the regulation, conductors must qualify in six core subjects and in an additional component on passenger evacuation procedures. Conductors are not required to qualify in the locomotive operation and train handling components. Railways must re-qualify conductors every three years. However, the regulation does not apply to Beltpack® operation because there is no requirement outlining the training necessary to operate a Beltpack®. Subsequently, there is no requirement for conductors trained in Beltpack® operations to receive hands-on supervised experience.
In preparation for the strike, CN provided TC with a list of company officers who were qualified in CROR and QSOC. However, many of these officers had little or no practical operating experience. TC did not require CN to outline the practical training provided to the officers to prepare them for assuming operating roles. However, CN met with TC before the strike and provided the regulator with information on its training plans. During the strike, TC conducted daily conference calls with CN to address any issues of rule compliance and it also increased its monitoring presence at Symington Yard.
Locomotive Configuration for Hump Assignment
The locomotive consist for the assignment was arranged in the hump set configuration normally used at Symington Yard (see Photo 2). In a hump set, the locomotives are set up as follows:
- The east locomotive (controlling unit) has the long nose trailing.
- The middle two units are slave units (that is, traction motor units with no locomotive cab).
- The west locomotive (trailing unit) has the long nose leading. (Note: In this occurrence, this locomotive was coupled to the cars in track ER-08.)

At Symington Yard, the east direction is designated as reverse and the west direction is designated as forward. Therefore, the Beltpack® OCU is configured such that, for the hump set to travel eastward, the reverse direction is selected on the OCU. Similarly, for the hump set to travel westward, the forward direction is selected on the OCU.
Symington Yard Accidents from 2001 to 2007
A review of the TSB database was conducted for non-main-track train collisions that occurred at Symington Yard from 2001 to 2006. In the six years preceding the labour disruption, between February 10 and 26, there was only one non–main-track train collision recorded at Symington Yard. During the 2007 strike between February 10 and 26, two non-main-track train collisions occurred at Symington Yard.
Analysis
There were no equipment or track defects present that were considered causal in this occurrence. The analysis will focus on the need to verify the direction of travel during Beltpack® operations, the use of a motor vehicle during switching, locomotive cab configurations, and the training of non-operating management personnel for service in operating positions.
The accident
The Beltpack® event recorder download indicated that, after coupling to the cut of cars in track ER-08, the operator did not request a change of direction. Consequently, the Beltpack® OCU was inadvertently left in the forward position (westward). While the operator intended the movement to proceed in the reverse (eastward) direction, the accident occurred when the assignment made an unintentional westward movement and collided with a departing westbound train. The omission of the change of direction on the OCU coincided with the arrival of a motor vehicle and the offering of a ride to the operator. By accepting the ride, the operator did not have to ride the point of the movement and be exposed to the cold weather. This was a deviation from the operator's previous experience because he had never been assisted by a motor vehicle while performing Beltpack® switching operations. This deviation in process likely distracted the operator, which led to the omission of changing the direction of travel on the OCU.
It took 46 seconds for the operator and the driver of the motor vehicle to realize that the movement was travelling in the wrong direction. While they both attempted to confirm the movement's direction of travel using the vehicle mirrors, visual perception may have been slightly distorted by the mirror, making it difficult to determine the direction of travel, particularly from a distance. Similar to previous TSB investigation R04W0035, the location of the Beltpack® operator in a motor vehicle, in advance of and facing away from the movement, also led to difficulty in monitoring the movement. These monitoring difficulties likely delayed the operator's decision to stop the movement, therefore increasing the time and distance the movement travelled in the unintended direction.
Canadian National Training in Preparation for the Strike
In preparation for the strike, the operator was given an abbreviated two-day Beltpack® training course. During this training, there were no instructions given regarding the confirmation of direction of travel, local switching procedures, or hump set configuration. Furthermore, CN's GOIs contain no instruction to verify the direction of travel when using a Beltpack®. Insufficient training, combined with the operator's limited practical experience, likely contributed to the omission of confirming the direction of travel immediately after initiating the Beltpack® command.
In contrast, CN's Beltpack® and yard training for unionized employees with operating experience consists of a seven- to ten-day course, which includes both classroom and field work. For new unionized employees with no operating experience, CN provides 33 days of Beltpack® and yard training, which includes classroom, field, and on-the-job training with a qualified Beltpack® operator. When compared to the training CN provided to unionized employees with similar experience, the level of training that CN managers received was minimal.
During the labour disruption, there were two non-main-track train collisions at Symington Yard. While the sample size is small, the number of collisions is higher than the six-year total for the same time period. The higher collision rate at Symington Yard during the strike suggests that the reduced level of training provided to managers in preparation for assuming operating roles increased the risk for adverse consequences to occur.
Verifying direction of travel
After coupling onto the cut of cars in track ER-08, the operator did not initiate the OCU command to place the movement in the eastward direction (that is, reverse). After the movement resumed, the operator did not verify the direction of travel until after he was in the motor vehicle. Had the operator visually verified the direction of the movement immediately after initiating the movement, the accident would likely have been averted.
CN's Beltpack® training material and the GOIs section pertaining to Beltpack® operations contain no instructions relating to the need to verify direction of travel after a Beltpack® movement has been initiated. The lack of written instructions and training to confirm the direction of travel after initiating a Beltpack® movement increases the risk of movements travelling in an unintended direction.
Vehicle-assisted Beltpack® wwitching operations at Symington Yard
During yard switching, a motor vehicle is occasionally employed as a tool to expedite yard operations. However, when a motor vehicle is used, it does not relieve operating employees of the responsibility to comply with rules or instructions. While it is not a common practice for Beltpack® operators to ride in a motor vehicle while controlling train movements, it does occur periodically at Symington Yard. Despite only periodic use, this is the second accident investigated by the TSB in the past three years at Symington Yard in which the Board determined that the use of a motor vehicle to assist with Beltpack® switching operations was a causal factor.
Using a motor vehicle to assist during Beltpack® operations is not inherently unsafe. However, this occurrence and the previous accident demonstrate that deviations to a normal work process can potentially distract an operator, which can minimize existing safety defences. Once the error of failing to ensure that the movement was travelling in the intended direction had been made, the placement of the vehicle ahead of the movement, rather than alongside the point of the movement, eliminated an additional opportunity to observe the direction of travel. In both occurrences, the placement of the vehicle ahead of the movement made monitoring difficult and increased the severity of the derailment.
While CROR and CN's GOIs contain numerous switching and yard operation procedures, neither regulatory nor company guidelines have been established for vehicle use during Beltpack® operations. The lack of regulatory or company guidelines for the use of a motor vehicle when assisting with Beltpack® operations increases the risk for errors and accidents to occur.
Locomotives with long nose leading
Normal locomotive cab configuration has the short nose leading and the long nose trailing when travelling in the forward direction. This configuration allows operating personnel to determine direction of travel visually. In comparison, hump assignment locomotives for switching operations are configured with the short nose leading on both ends of the consist.
This hump assignment configuration, which has a symmetrical visual appearance, does not allow one to visually determine the direction of travel based only on the physical appearance of the hump set.
CN's Beltpack® training for managers in Symington Yard did not cover the locomotive cab configuration and its significance when configured within a normal hump set. This would have normally been learned through on-the-job training. In this occurrence, it is unlikely that the physical orientation of the hump set played a role in the selection of direction. However, the use of a controlling cab with long nose leading in a locomotive consist increases the potential for confusion in the selection of direction, especially among inexperienced operating personnel.
Findings
Findings as to causes and contributing factors
- The accident occurred when the hump assignment made an unintentional westward movement and collided with a departing westbound train.
- The operator control unit (OCU) for the Beltpack® was inadvertently left with the direction command in the forward position when the movement was initiated.
- The Beltpack® operator was likely distracted by the arrival of a motor vehicle, which led to the omission of changing direction on the OCU.
- The location of the Beltpack® operator in a motor vehicle, in advance of and facing away from the movement, and the use of vehicle mirrors to monitor the movement made it difficult to determine the direction of travel. These factors delayed the operator's decision to stop the movement, therefore increasing the time and distance the movement travelled in the unintended direction.
- Insufficient training, combined with the operator's limited practical experience, likely contributed to the omission of confirming the direction of travel immediately after initiating the Beltpack® command.
Findings as to risk
- The higher-than-average accident rate at Symington Yard during the labour disruption suggests that the reduced level of training provided to managers in preparation for assuming operating roles increased the risk for adverse consequences to occur.
- The lack of written instructions and training to confirm the direction of travel after initiating a Beltpack® movement increases the risk of movements travelling in an unintended direction.
- The lack of regulatory or company guidelines for the use of a vehicle when assisting with Beltpack® operations increases the risk for errors and accidents to occur.
Other finding
- The use of a controlling cab with long nose leading in a locomotive consist increases the potential for confusion in the selection of direction, especially among inexperienced operating personnel.
Safety action taken
On 22 March 2007, Transport Canada (TC) issued a Notice and Order under Section 31 of the Railway Safety Act. The Notice and Order stated in part:
Canadian National Railway not allow or permit Employees or Supervisors for a non-operating background to work in any job category of an operating employee unless said supervisor has received a minimum of 10 days of classroom training respective of the duties and rules of an operating employee and a minimum of 20 days of on the job training in the job category of an operating employee.
After meeting with Canadian National (CN), reviewing the proposed training program, and validating the qualifications of CN's operating personnel, TC rescinded the Notice and Order.
In November 2007, CN issued a System Bulletin indicating that Beltpack® operators must visually verify that the movement is responding in the requested direction immediately after commanding a direction and speed.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .