Heurt violent et incendie à bord
du vraquier Windoc
mettant en cause le pont 11
sur le canal Welland, Allanburg (Ontario)
Le Bureau de la sécurité des transports du Canada (BST) a enquêté sur cet événement dans le but de promouvoir la sécurité des transports. Le Bureau n’est pas habilité à attribuer ni à déterminer les responsabilités civiles ou pénales. Le présent rapport n’est pas créé pour être utilisé dans le contexte d’une procédure judiciaire, disciplinaire ou autre. Voir Propriété et utilisation du contenu. Les pronoms et les titres de poste masculins peuvent être utilisés pour désigner tous les genres afin de respecter la Loi sur le Bureau canadien d’enquête sur les accidents de transport et de la sécurité des transports (L.C. 1989, ch. 3).
Résumé
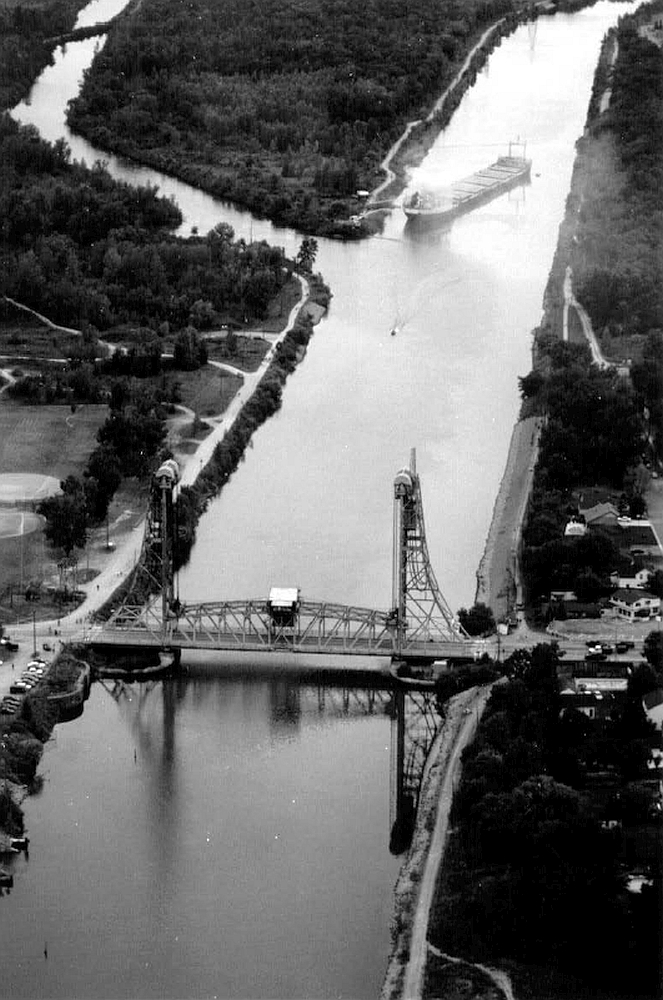
Vers 20 h 54, pendant la descente du canal Welland, en passant sous le pont 11 à Allanburg en Ontario, le vraquier Windoc a été heurté par la travée levante du pont qui a été abaissée avant que le navire ait eu le temps de passer au complet. La timonerie et la cheminée du navire ont été détruites. Le Windoc a dérivé vers l'aval, a pris feu et s'est échoué à environ 800 mètres du pont. Même si sa cargaison de blé n'a pas été endommagée, le navire a été déclaré perte réputée totale. La structure du pont a été endommagée et le canal Welland a été fermé aux navires pendant deux jours. L'accident n'a fait ni blessé grave ni pollution.
1.0 Renseignements de base
1.1 Fiche technique du navire
| Nom | Windoc (anc. Steelcliffe Hall) |
|---|---|
| Numéro officiel | 383573 |
| Port d'immatriculation | Thunder Bay (Ontario) |
| Pavillon | Canada |
| Type | Vraquier |
| Jauge bruteNote de bas de page 1 | 18 516,64 |
| LongueurNote de bas de page 2 | 218,2 m |
| Tirant d'eau | Av. : 7,95 m Ar. : 7,95 m |
| Construction | Section avant et tranche de la cargaison : Canada, 1977 Section arrière : Allemagne, 1959 |
| Groupe propulseur | Un diesel lent Burmiester & Wain à simple effet, 6 436 kW, entraînant une seule hélice à pas variable |
| Cargaison | 26 023,9 tonnes métriques |
| Équipage | 14 personnes |
| Passagers | Aucun |
| Propriétaires | N. M. Paterson & Sons Ltd., Thunder Bay (Ontario) Canada |
1.1.1 Renseignements sur le navire
Le Windoc a été construit à Hambourg en Allemagne de l'Ouest en 1959 pour servir de vraquier océanique. En 1977, le navire a subi une refonte au Canada. La partie arrière, qui logeait le groupe propulseur, l'appareil à gouverner et les emménagements, a été conservée. La partie de la coque située devant la salle des machines a été remplacée pour permettre le transport d'une plus grande quantité de cargaison sèche et la timonerie a été déplacée vers l'arrière, au-dessus des emménagements. Le navire avait six cales à cargaison.
1.2 Détails sur le pont
1.2.1 Renseignements sur le pont
Le pont 11 est un des trois ponts à travée levante qui permettent aux véhicules routiers de franchir le canal. Situé à Allanburg en Ontario, à 11,4 milles marins (M) en amont du brise-lames de Port Weller sur le lac Ontario (43°04′35″N, 79°12′38″W), le pont a été utilisé sans interruption depuis sa construction en 1932. Des pylônes placés de part et d'autre du canal soutiennent la travée et la guident lorsqu'elle est levée et abaissée. Une caméra fixe installée au sommet du pylône de l'Est permet aux contrôleurs du centre de contrôle de la circulation (CCC) de la Corporation de gestion de la Voie maritime du Saint-Laurent (CGVMSL) d'avoir une vue limitée des navires qui approchent du pont depuis l'amont (c.-à-d. venant du sud).
La travée est faite d'acier et la chaussée routière est revêtue d'asphalte. Entre les deux pylônes, la largeur du canal est réduite à 60,9 m, soit la distance entre les appuis porteurs des pylônes. La hauteur libre entre la travée levée au maximum et le niveau de l'eau du canal était de 36,5 m. L'axe longitudinal de la travée coïncide avec l'axe longitudinal du canal entre les appuis porteurs.
Le poste de commande du pontier est placé entre les poutres à treillis au-dessus de l'axe longitudinal de la travée. Les moteurs et les génératrices qui alimentent le mécanisme actionnant la travée sont placés juste au-dessus du poste de commande du pontier.
Des feux de signalisation montés de part et d'autre de la travée sur l'axe longitudinal permettent aux navires approchant de déterminer si la travée est stationnaire, en mouvement ou complètement levée.
1.3 Navigation sur le canal Welland
1.3.1 Centre de contrôle de la circulation
Le contrôle et l'organisation du trafic maritime dans le canal ainsi que la coordination des communications entre les navires et les organismes responsables du canal sont assurés par les contrôleurs du CCC. Ces derniers communiquent directement avec les navires qui circulent dans le canal sur des postes radio très haute fréquence (VHF). Ils communiquent directement par téléphone conventionnel et téléphone mobile avec le personnel de la CGVMSL qui contrôle les écluses et les ponts, afin d'assurer la coordination générale du trafic maritime. Les contrôleurs peuvent surveiller la circulation des navires en temps réel grâce à des caméras fixes ou télécommandées placées tout le long du canal. Les contrôleurs sont également chargés de l'exploitation au moyen d'une télécommande du seul pont automatisé du canal.
Pour le pont 11, il y avait trois moyens de communication possibles entre le pontier et le contrôleur du CCC : téléphone conventionnel, communications par poste VHF fixe et communications par radio VHF portative. Habituellement, les communications courantes liées au trafic maritime entre le pontier et le contrôleur se faisaient par téléphone conventionnel.
Les conversations radio et les conversations téléphoniques entre les contrôleurs et les navires, ainsi qu'entre les contrôleurs et le personnel des ponts et des écluses sont enregistrées automatiquement au CCC. Il est possible d'enregistrer sur bande vidéo les images captées par les caméras de la CGVMSL, mais l'enregistrement doit être lancé manuellement.
1.3.2 Marche à suivre pour les navires qui approchent des ponts
La marche à suivre pour les navires qui approchent d'un pont dans le canal est précisée dans Le manuel de la Voie maritimeNote de bas de page 3, dont un exemplaire se trouvait dans la timonerie du Windoc. Lorsque le nez d'un navire arrive au damier à carrés jaunes et noirs qui constitue le panneau de signalisation au sifflet, le pontier déclenche un feu jaune qui se met à clignoter. Cela indique que le pontier est conscient de l'arrivée du navire et qu'il va commencer à lever la travée du pont. Si le feu jaune ne clignote pas, le navire doit signaler sa présence au pontier par radiotéléphone VHF sur la voie désignée.
Après l'accusé de réception du pontier, les feux de signalisation de la travée du pont, qui sont rouges lorsque la travée est complètement fermée, commencent à clignoter quand le pontier lève la travée. Le navire peut continuer d'avancer vers le pont, mais il ne doit pas dépasser l'« indication de limite d'approche » tant que la travée du pont n'est pas levée au maximum, moment où le feu de signalisation tourne au vert. L'« indication de limite d'approche » était placée à 60 m du pont 11. Lorsque la travée du pont est abaissée, les feux de signalisation passent du vert au rouge continu.
Le poste de commande du pontier du pont 11 est muni d'un radar ainsi que d'un détecteur-récepteur à micro-ondes, qui est situé à Port Robinson, à environ 2,2 milles marins (M) en amont du pont 11. Ces dispositifs sont utilisés pour prévenir le pontier de l'approche d'un navire par visibilité réduite. Les deux dispositifs sont munis d'alarmes.
1.4 Chronologie des événements
1.4.1 Windoc
Le 8 août 2001, le Windoc quitte Thunder Bay avec une cargaison de blé à destination de Montréal (Québec). Le 11 août, à 17 h 48, heure avancée de l'Est (HAE)Note de bas de page 4, le navire arrive à l'entrée sud du canal, puis passe sous le pont 21 à travée levante et le pont 19A à bascule avant de pénétrer dans l'écluse 8. À 19 h 23, il quitte l'écluse, passe sous le pont 19 à bascule et commence à descendre le canal. Huit des 22 membres de l'équipage qui se trouvent à bord sont autorisés à descendre à terre avant que le navire ne reprenne sa route vers l'aval.
À 20 h 28, le capitaine informe le contrôleur du CCC sur la voie 14 du radiotéléphone VHF que le Windoc se trouve à la hauteur de Port Robinson. Le troisième officier et un timonier se trouvent dans la timonerie avec le capitaine. La vitesse moyenne du navire sur le fond est d'environ 6 noeuds entre Port Robinson et le pont 11.
Le navire descend le canal et l'équipe à la passerelle voit les feux d'approche oranges clignotants placés à 925 m du pont du côté ouest du canal, ce qui indique que le pontier est au courant de l'approche du navire. La vitesse signalée du navire est d'environ 5 noeuds. Alors que le Windoc se rapproche du pont, les feux de signalisation du pont sont rouges et clignotent, et la travée s'élève. Une fois le navire rendu à une position comprise entre 0,75 et 0,5 M du pont, les feux de signalisation deviennent vert continu et la travée levante est levée au maximum. Le navire, dont l'axe longitudinal est aligné sur les feux de signalisation du pont, s'engage sous la travée.
Alors que la moitié environ du navire se trouve sous le pont, le troisième officier constate que les feux de signalisation sont passés au rouge continu et que la travée descend. À 20 h 53, le capitaine actionne à quelques reprises le sifflet du navire. Sans s'identifier ni préciser de quel pont il s'agit, le capitaine appelle le CCC sur la voie VHF 14 pour s'enquérir de l'abaissement de la travée. Il stoppe aussitôt les machines et ordonne l'évacuation de la timonerie.
Le capitaine et le troisième officier quittent la timonerie par l'aileron de passerelle de tribord. Alors qu'ils sont en train de descendre par l'échelle d'accès externe de la passerelle, la travée du pont heurte le navire au niveau des fenêtres avant de la timonerie, rasant la timonerie et la cheminée du Windoc (voir la photo 1).

Resté à son poste dans la timonerie, le timonier se couche sur le pont, alors que la travée passe au-dessus de sa tête. Il réussit à se dégager des débris et à descendre par le puits d'escalier du rouf avant que le troisième officier ne revienne dans la timonerie pour le chercher. Lorsque le contrôleur du CCC entend un appel sur la voie VHF 14 concernant l'abaissement d'une travée de pont, il reconnaît la voix et a recours à la caméra placée au point milliaire 14,6 de la Voie maritime, à l'ouest de Port Robinson, pour regarder ce qui se passe au pont 11. Le contrôleur voit que l'arrière du navire est toujours engagé sous le pont et il constate que l'image de la caméra fixe montée sur le pylône est du pont 11 tremblote. Le contrôleur conclut donc que la travée a été abaissée sur le navire.
Après l'accident, l'alarme générale est déclenchée. L'équipage se rassemble sur le pont principal, et personne ne manque à l'appel.
Le navire dérive vers l'aval à partir du pont 11. Un incendie éclate dans le tambour-machine et se propage à la charpente des emménagements. On mouille l'ancre de tribord, mais le navire touche la berge est du canal par l'avant tribord. Le Windoc dérive ensuite vers le côté ouest du canal avant de s'échouer à environ 800 m du pont 11 (voir la photo 2).
1.4.2 Pontier
Le 11 août était un jour de repos pour le pontier qui venait de faire deux quarts de jour de 12 heures la veille et l'avant-veille. Le pontier avait pris deux comprimés Darvon-N vers 8 h ce matin-là pour soulager des douleurs au dos et il avait consommé entre deux et quatre verres de vin au dîner. Entre 13 h et 14 h, il avait reçu un appel téléphonique d'un chef d'équipe de la CGVMSL lui demandant s'il voulait faire un quart supplémentaire ce soir-là au pont 11, et le pontier avait accepté. Il n'avait pas été question de sa capacité à faire le travail au moment de la demande et cela n'a rien d'inhabituel. Selon la politique de la CGVMSL, il est interdit à un employé de se présenter au travail avec les facultés affaiblies. Après l'appel téléphonique, le pontier s'est reposé, a mangé et a essayé de dormir, mais en vain. Selon l'information recueillie, il n'a plus consommé d'alcool ni pris de médicament après avoir accepté le quart supplémentaire.
Vers 17 h 45, le pontier part de chez lui et se rend au pont 11 au volant de son véhicule. Vers 18 h 20, il arrive au pont et se rend à la travée levante. Il y rencontre le pontier du quart précédent qui lui dit qu'il s'attend à un quart occupé ce soir-là. Aucune autre information n'est échangée au moment de la relève du quart. Le pontier grimpe dans le poste de commande par l'échelle d'accès pour prendre son quart.
Vers 18 h 57, le pontier lève la travée pour la première fois du quart et il informe le contrôleur du CCC par téléphone que le navire Algocape est engagé sous le pont 11. Le pontier converse alors brièvement avec le contrôleur qui lui dit que les prochains bâtiments à franchir le pont 11 seront le navire avalant John B. Aird et deux yachts remontant. Le pontier abaisse ensuite la travée pour permettre aux véhicules de traverser le pont avant de la relever pour permettre le passage des trois bâtiments annoncés. À 19 h 41, au cours de sa dernière conversation téléphonique avec le contrôleur du CCC, le pontier informe celui-ci que les deux yachts et le John B. Aird sont en train de passer sous le pont 11.
À 20 h 50, le pontier téléphone au CCC et baragouine d'une voix inintelligible que le Windoc « arrive sous [le pont] 11 ». Le contrôleur, auquel la voix du pontier parvient via un haut-parleur, ne comprend pas bien et il demande au pontier de répéter son message. Immédiatement après cet appel téléphonique, le pontier rappelle le CCC. Lorsque le contrôleur lui répond, le pontier lui semble mêlé parce qu'il demande s'il parle à l'écluse 7. Le contrôleur du CCC répond au pontier qu'il va retransmettre le message du pontier à l'écluse 7 dont les téléphones sont défectueux.
Après l'appel de 20 h 50, le pontier commence à baisser la travée. Il a indiqué qu'il avait abaissé la travée après avoir constaté que l'arrière du navire dépassait le pont. Il ne signale pas immédiatement l'accident au CCC.
À 20 h 54, après avoir capté sur la voie VHF 14 l'appel radiotéléphonique où il est question d'une travée abaissée sur un navire, le contrôleur du CCC, qui a constaté que l'image sur son écran en provenance de la caméra fixe montée en haut du pont 11 tremblote, téléphone au pontier et lui demande s'il a abaissé la travée sur le navire. Le pontier lui répond que le Windoc a heurté le pont. Le contrôleur demande au pontier de lever la travée.
À 20 h 56, les contrôleurs du CCC reçoivent des appels leur signalant un accident et un incendie au pont 11. Les contrôleurs appellent le pontier plusieurs fois sans recevoir de réponse. Ce n'est qu'à 21 h 6 que le contrôleur réussit à parler au pontier qui se dit surpris que les services d'urgence soient en route et affirme ne pas comprendre pourquoi le personnel des services d'urgence désire le voir. Lorsque le contrôleur l'interroge expressément sur l'incendie à bord du navire, le pontier répond qu'il s'agit d'un petit feu.
À 21 h 6, un agent de police arrive au pont 11. La travée du pont est abaissée mais pas jusqu'au point de butée et l'agent se rend au poste de commande du pont pour parler au pontier. À 21 h 10, un superviseur de la CGVMSL arrive au pont 11 et grimpe jusqu'au poste de commande pour parler au pontier. Peu après, d'autres membres du personnel de la CGVMSL ainsi que les équipes d'urgence arrivent sur les lieux. L'agent de police et le coordonnateur du secteur de la CGVMSL témoignent qu'ils ont trouvé le pontier assis dans l'obsécuritéé et affirment qu'il leur a semblé secoué ou en état de choc.
Un ambulancier paramédical procède à l'examen des signes vitaux du pontier. Il demande à celui-ci de se rendre à l'hôpital pour subir d'autres examens mais essuie un refus. Vers 22 h 30, le pontier, accompagné d'une autre personne, quitte le pont pour rentrer chez lui.
Après l'accident, le pontier a totalement oublié les événements qui sont survenus entre le moment où il a pris la décision d'abaisser la travée et celui où le personnel de la CGVMSL est arrivé au pont, soit un laps de temps de 25 minutes.
1.4.3 Communications entre le pont 11 et le CCC
Les enregistrements des communications entre le pontier et les contrôleurs du CCC juste avant le heurt révèlent que le pontier avait de la difficulté à communiquer au cours de cette période. Lorsque le pontier a appelé le CCC pour faire savoir que le Windoc était sous le pont 11, le contrôleur a eu de la difficulté à le comprendre et lui a demandé de répéter le message. Un peu plus tard, lorsque le pontier a de nouveau parlé au CCC en tentant de communiquer avec l'écluse 7, il a mis du temps à comprendre qu'il s'était trompé, il avait la voix pâteuse et il a demandé au contrôleur de retransmettre son message à l'écluse 7, ce que le contrôleur a accepté de faire. Ce message a été reçu sur un téléphone main libre et, avant de raccrocher, les deux contrôleurs de service ont commenté l'état dans lequel semblait être le pontier. L'accident s'est produit moins de deux minutes plus tard.
Après l'accident, les contrôleurs du CCC ont eu deux autres conversations avec le pontier. Le contenu de ces conversations montre que le pontier ne semblait pas conscient de ce qui s'était produit.
1.5 Effets du Darvon-N
Darvon-N est le nom sous lequel est commercialisé le napsylate de propoxyphène, un analgésique narcotique qui agit sur le système nerveux central. Le Darvon-N est prescrit pour soulager des douleurs légères à modérées lorsque les médicaments moins puissants sont inefficaces ou contre-indiqués. Le Darvon-N est ingéré par voie orale et il atteint sa concentration maximale dans le plasma de l'individu en 2 à 2,5 heures. Sa durée d'actionNote de bas de page 5 est de 3 ou 4 heures.
Le napsylate de propoxyphène est métabolisé dans le foie, se transformant en norpoxyphène. La demi-vieNote de bas de page 6 du propoxyphène est de 6 à 12 heures et celle du norpoxyphène, de 30 à 36 heures. Le norpoxyphène agit aussi sur le système nerveux central, mais est beaucoup moins puissant que le propoxyphène. Les effets du propoxyphène sur le système nerveux central sont accrus par la consommation d'alcool.
1.6 Examen de la parole
On a demandé l'aide du National Transportation Safety Board (NTSB) des États-Unis pour examiner les enregistrements des conversations téléphoniques entre le pontier et le CCC afin de déterminer si celui-ci avait les facultés affaiblies au moment de l'accident. En se fondant sur l'expérience précédente de l'analyse des effets de facteurs psychologiques sur la parole, le groupe chargé de l'analyse a examiné 62 conversations téléphoniques que le pontier a eues avec le CCC entre le 18 juin et le 11 août 2001.
Deux types d'analyses ont été effectuées. Dans un premier temps, on a comparé les caractéristiques physiques de l'élocution du pontier le soir de l'accident avec un prélèvement de départ provenant des quarts antérieurs. Les éléments mesurés comprenaient la fréquence fondamentale, la latence (le temps mis pour répondre au téléphone ou pour s'exprimer soi-même au téléphone), les erreurs dans l'articulation, le débit ainsi que la prononciation de sons particuliers comme les « l » et les « s ». Le second type d'analyse effectuée par le groupe était plus qualitatif et portait sur l'examen des enregistrements au niveau de la qualité générale et du contenu le soir de l'accident ( voir le paragraphe 2.2).
1.7 Coordination des activités d'intervention par le centre de contrôle de la circulation
À 20 h 54, après avoir constaté que l'image provenant de la caméra installée sur le pont 11 tremblotait et après avoir parlé au pontier, les contrôleurs du CCC ont vainement tenté à plusieurs reprises de communiquer avec le coordonnateur de secteur sur la radio mobile et avec le Windoc par radio VHF, tout en s'occupant de la gestion du trafic maritime dans le canal.
À 20 h 56 et 20 h 57, les contrôleurs du CCC ont reçu des appels téléphoniques d'un répartiteur des services policiers de la région du Niagara demandant des renseignements au sujet d'un accident survenu au pont 11. Le répartiteur a informé le contrôleur que la police, l'ambulance et les pompiers se dirigeaient vers le lieu de l'accident. Le contrôleur n'a pas donné au répartiteur tous les renseignements sur l'accident, mais il a mentionné qu'il voyait de la fumée. Les contrôleurs pouvaient apercevoir de la fumée sur leurs écrans, mais il leur était impossible de voir le navire ou la travée.
À 21 h, les contrôleurs ont communiqué avec le coordonnateur de secteur (qui était de service en tant que coordonnateur maritime, à ce moment-là) pour l'informer de l'accident survenu au pont 11. Le coordonnateur de secteur s'est ensuite rendu au pont 11.
À 21 h 3, le capitaine du Windoc a appelé le CCC, au moyen d'une radio VHF portative, pour prévenir le contrôleur qu'il y avait un incendie à bord du navire.
Vers 21 h 5, les contrôleurs du CCC ont prévenu leurs dirigeants ainsi qu'un inspecteur de navires de la CGVMSL de l'accident.
À 21 h 8, en réponse à une question du service d'incendie, le contrôleur a répondu que le Windoc avait à son bord une cargaison de blé.
À 21 h 10, le coordonnateur de secteur de la CGVMSL a signalé au CCC son arrivée au pont 11 et est monté dans le poste de commande du pont pour parler au pontier.
À 21 h 12, un des contrôleurs du CCC a appelé un employé de la CGVMSL à l'écluse 8 pour lui demander de se rendre au pont 11, mais sans pouvoir lui dire de quel côté du canal il devait se rendre. Dans l'intervalle, le service d'incendie a appelé le contrôleur du CCC pour s'enquérir de la situation du pont. Le contrôleur a répondu que la communication avait été établie avec le pontier et que la travée du pont était levée d'environ 10 pieds.
À 21 h 13, l'inspecteur de navire de la CGVMSL a appelé le contrôleur du CCC pour demander de quel côté du canal il devait se rendre. Le contrôleur qui a parlé à l'inspecteur a déclaré qu'il lui était impossible de voir le navire mais qu'il croyait que celui-ci se trouvait plus près du côté est du canal.
À 21 h 23, le capitaine du Windoc a appelé le CCC pour dire qu'il craignait une explosion et faire savoir qu'il allait demander à ses équipes de lutte contre l'incendie d'évacuer l'arrière du navire. Le capitaine a aussi indiqué qu'il croyait que les pompiers devraient être en mesure d'arroser l'arrière du navire depuis la berge ouest du canal.
À 21 h 25, le contrôleur du CCC a retransmis au service d'incendie la suggestion du capitaine mais sans mentionner son inquiétude quant au risque d'explosion; il a fait état lorsqu'il a rappelé le service d'incendie six minutes plus tard.
À 21 h 27, l'inspecteur de navires, après son arrivée sur les lieux, a appelé les contrôleurs du CCC pour demander qu'on prenne des dispositions afin de lui envoyer une petite embarcation pour l'amener au navire. Un contrôleur a appelé le bateau-pilote de Port Colborne pour lui demander de se rendre au pont 11. Toutefois, le bateau-pilote estimait qu'il ne pourrait arriver sur les lieux avant 23 h environ. De plus, le bateau-pilote dont le tirant d'air était d'environ 22 pieds, ne pourrait passer sous le pont pour atteindre le Windoc. La CGVMSL ne voulait pas lever la travée avant qu'on ait procédé à une inspection minutieuse du pont et des structures de soutien. Les contrôleurs ont commencé à appeler d'autres navires se trouvant dans les parages ainsi que le personnel de la CGVMSL pour trouver une embarcation. On leur a alors appris que le service d'incendie de St. Catharines possédait des embarcations qui avaient été déployées pour aider à lutter contre l'incendie. Ils ont également appris que la CGVMSL avait dépêché une petite embarcation.
À 22 h 32, le service d'incendie, après avoir réussi à trouver un point de lancement approprié, a mis à l'eau ses embarcations.
À 22 h 53, le centre des Services de communications et de trafic maritimes (SCTM) de Sarnia (Ontario) de la Garde côtière canadienne (GCC) a appelé le CCC pour s'enquérir d'un bulletin de nouvelles mentionnant un accident survenu au pont 11 qu'il venait de recevoir du Centre d'intervention en cas de déversement (CID) du ministère de l'Environnement de l'Ontario.
Le contrôleur a informé les SCTM que la CGVMSL avait pris en charge l'intervention. Il n'y avait ni blessés ni pollution et aucun rapport d'accident n'avait été diffusé. Auparavant, un des contrôleurs avait appelé une station radio locale pour laisser un message faisant état de la fermeture du pont 11 au trafic routier à la suite d'un accident.
À 23 h, le service d'incendie a appelé le CCC pour demander si la CGVMSL allait prendre des mesures pour se prémunir contre une éventuelle fuite de mazout du navire et demander si le ministère de l'Environnement de l'Ontario avait été prévenu de l'accident. Après qu'un des contrôleurs se fut entretenu avec l'inspecteur de navires de la CGVMSL, il a été décidé de déployer, par mesure de prudence, un barrage de rétention des hydrocarbures. Le contrôleur a appelé un fournisseur local de matériel d'intervention, mais sans obtenir de réponse. Ce fournisseur possédait une permanence téléphonique après les heures ouvrables, mais le contrôleur a raccroché avant que son appel ne soit transmis à la permanence téléphonique.
À 23 h 9, le bateau-pilote est arrivé au pont 11 et des ingénieurs de la CGVMSL sont montés à bord pour inspecter le dessous de la travée.
À 23 h 10, un contrôleur a d'abord appelé le service d'incendie, puis les SCTM et le CID afin d'obtenir un barrage de rétention des hydrocarbures, mais sans succès.
À 23 h 16, un agent de la Direction du sauvetage, de la sécurité et de l'intervention environnementale (SSIE) de la GCC a appelé le CCC et a fourni au contrôleur un mauvais numéro de téléphone 1-800 du fournisseur local de matériel d'intervention. Le numéro de téléphone donné était en réalité celui du centre des SCTM de Sarnia, lequel ne connaissait pas le numéro de téléphone demandé mais a fourni le numéro d'un autre fournisseur de matériel d'intervention établi près de Hamilton (Ontario). Au moment de l'accident, la CGVMSL n'avait pas d'entente en matière d'approvisionnement avec un fournisseur de matériel d'intervention.
À 23 h 29, un employé de la CGVMSL a informé le contrôleur que la Corporation possédait un barrage, qui serait cependant difficile à déployer; une longueur de 300 pieds du barrage se trouvait à l'extrémité sud du canal et une autre section de 100 pieds à l'extrémité nord.
À 23 h 55, le contrôleur a communiqué avec un fournisseur établi près de Hamilton qui a été en mesure de fournir et de déployer un barrage de rétention des hydrocarbures dans le canal. Le barrage a été placé en travers du canal et en aval du Windoc à 4 h 40 le lendemain matin, soit six heures après la suggestion de déploiement initiale.
1.8 Lutte contre l'incendie
La première explosion ainsi que l'incendie qu'elle a déclenché ont été alimentés par un réservoir en charge de mazout situé près de la cheminée. Après s'être rassemblés en avant des emménagements, les membres de l'équipage ont gréé des manches à incendie et ont commencé à combattre l'incendie à l'aide de la pompe à incendie de secours du navire. Les premiers efforts de lutte contre l'incendie ont permis de réduire l'intensité du brasier mais le capitaine, craignant l'explosion des caisses journalières de mazout placées dans la salle des machines, a ordonné à l'équipage de s'éloigner du foyer de l'incendie en attachant les manches à incendie en place de façon à ce que leurs jets soient dirigés vers le feu. Après l'arrivée des équipes de pompiers municipaux sur la berge du canal près du navire à 22 h, le capitaine a dirigé l'évacuation de l'équipage à bord d'un radeau de sauvetage avant. Le capitaine et le chef mécanicien sont restés à bord pour diriger les efforts des équipes de pompiers riveraines.
Le premier signalement de l'accident fait par la population aux services policiers de la région du Niagara est survenu à 20 h 56; des policiers, des pompiers et une ambulance ont été dépêchés sur les lieux. Le service d'incendie de Thorold a envoyé des camions-citernes qui sont arrivés sur la berge est du canal à 21 h 05. Toutefois, le Windoc a commencé à dériver vers la berge ouest du canal, forçant les unités de lutte contre l'incendie à faire un détour, et elles ne sont arrivées qu'à 21 h 20 à la position finale du Windoc. Comme il n'y avait pas de fréquence radio commune, les premières communications du service d'incendie avec le navire ont consisté en des cris au capitaine. Selon les rapports initiaux des témoins, certains membres de l'équipage avaient sauté à l'eau lors de l'abandon du navire; toutefois, le capitaine du Windoc a assuré aux équipes de secours arrivées sur les lieux que tous les membres de son équipage étaient sains et saufs. Lors de l'évacuation du navire, le capitaine a confié aux membres de l'équipage un poste radio VHF portatif destiné aux équipes de pompiers riveraines afin de faciliter les communications.
Comme l'arrière du Windoc se trouvait à environ 20 m de la berge du canal et que la seule embarcation disponible pour monter à bord était le radeau de sauvetage du navire, l'embarquement des membres du service d'incendie a été retardé. Ceux-ci ont initialement combattu l'incendie à l'aide de pompes portatives et de manches à incendie dirigés à partir des échelles aériennes des camions-citernes (voir la photo 3). Le service d'incendie de Thorold ne disposait pas d'embarcations pour transporter ses pompiers jusqu'au navire. Il leur a fallu attendre l'arrivée en soirée des pneumatiques à coque rigide du service d'incendie de St. Catharines. Ni le CCC ni les services d'incendie locaux ne savaient où trouver des rampes de mise à l'eau à proximité du lieu de l'accident, ce qui a retardé l'arrivée des embarcations.

À 22 h 30, un inspecteur de navires du CGVMSL a pu, grâce au radeau du navire, monter à bord du Windoc afin d'aider le capitaine et le chef mécanicien qui étaient restés sur le navire lors de l'évacuation de l'équipage. À 23 h 30, l'inspecteur de la Voie maritime a constaté que la cloison arrière des emménagements était chaude au toucher alors que les cloisons avant étaient froides, ce qui indiquait que l'incendie était toujours circonscrit dans la partie arrière des emménagements. À 1 h 45, sept membres du service d'incendie de Thorold sont montés à bord du Windoc pour évaluer la situation et coordonner les activités de lutte contre l'incendie avec le capitaine et le chef mécanicien.
Au moment de l'accident, le plan de lutte contre l'incendie du navire était rangé dans la timonerie, laquelle a été détruite lorsque la travée du pont a heurté le navire. Il n'y avait pas d'exemplaire de ce plan à l'extérieur des emménagements. Malgré l'absence de plan, les pompiers, ayant reçu un briefing par le capitaine et le chef mécanicien, et armés de manches à incendie alimentées par les pompes de secours du navire, ont pénétré dans les emménagements pour une reconnaissance à 2 h 20. Comme ils ne connaissaient pas bien la disposition à bord du navire et à cause de la fumée épaisse, ils ne sont pas restés à l'intérieur pour combattre l'incendie et ils sont ressortis sur le pont principal à 2 h 30.
Sur les instructions de leur chef, les pompiers ont ouvert les portes avant étanches des emménagements afin de laisser sortir la fumée du compartiment. Peu après, l'incendie s'est propagé dans la partie avant des emménagements, aux cabines du capitaine et du chef mécanicien. Les équipes de lutte contre l'incendie ont alors décidé de combattre l'incendie en pointant des manches à incendie par les hublots brisés de la cloison avant.
À 7 h, les pompiers ont de nouveau pénétré dans les emménagements, déversé le contenu du système d'extinction fixe au CO2 dans la salle des machines ouverte et ouvert les vannes pour envoyer de l'eau dans le système d'extincteurs automatiques à eau. Toutefois, le réseau de distribution des extincteurs à eau avait été endommagé par le heurt violent et le feu, le rendant inutilisable. Les pompiers ont continué de lutter contre l'incendie depuis l'extérieur de la superstructure du navire pendant la journée du 12 août et cela jusqu'à ce que l'incendie soit déclaré éteint à 16 h 30.
1.9 Victimes
Aucune blessure n'a été signalée.
1.10 Avaries et dommages
1.10.1 Avaries au navire
La timonerie, le mât principal, les manches à air de la salle des machines et la cheminée ont été détruits par le contact avec la travée du pont. Le réservoir de mazout de l'incinérateur, placé à l'intérieur de l'enveloppe de cheminée, a été fendu et du mazout s'est déversé dans la salle des machines ainsi que sur le pont des embarcations. Les emménagements des divers ponts ont été détruits par le feu, la chaleur et la fumée. Le tambour-machines et la machine principale ont été endommagés par le feu, la chaleur et l'eau. Le bordé de bouchain au droit de la citerne de ballast tribord no 1 était gondolé et fendu. La cloison arrière et les varangues de bouchain étaient déformées et arrachées. Le navire a été déclaré perte réputée totale, mais aucun dommage à la cargaison n'a été signalé (voir la photo 4).

1.10.2 Dommages au pont
Le pont a subi des dommages structurels à la partie centrale de la travée levante (voir la photo 5). Les extrémités de la travée ont aussi été endommagées à cause du mouvement latéral provoqué par le heurt violent.

Si l'on excepte les réglages mineurs qui ont dû être apportés aux câbles métalliques actionnant la travée, les systèmes mécaniques ou électriques du pont n'ont pas été endommagés.
Les réparations au pont ont été effectuées alors que la travée était complètement levée pour permettre aux navires de circuler dans le canal. Après une inspection par les ingénieurs de la CGVMSL, le pont a été rouvert au trafic routier le 16 novembre 2001.
1.10.3 Dommages à l'environnement
Aucun dommage à l'environnement n'a été signalé.
1.11 Brevets et certificats
1.11.1 Certificats du navire
Le navire possédait les certificats applicables au secteur d'exploitation et au type de navire.
1.11.2 Certificat du pont
Le pont avait été inspecté par des ingénieurs de la CGVMSL; toutefois, son exploitation ne requiert pas l'obtention d'un certificat.
1.11.3 Brevets et certificats du personnel
Les membres de l'équipage possédaient les qualifications nécessaires en vertu de la réglementation en vigueur.
Le pontier n'est pas tenu d'être titulaire d'un certificat. Il avait reçu de la formation en cours d'emploi sur le fonctionnement de la travée levante.
1.12 Renseignements sur le personnel
1.12.1 Capitaine
L'expérience du capitaine remonte à 1981. Il a travaillé pour plusieurs compagnies maritimes avant de se joindre à la N.M. Paterson & Sons Ltd. en 1989. Il a été capitaine du Paterson pendant cinq ans puis capitaine de relève du Windoc avant de passer capitaine du Windoc en l'an 2000. Il a rejoint le Windoc en juin 2001 comme capitaine et il occupait ce poste au moment de l'accident.
1.12.2 Pontier
Il a d'abord été embauché comme manoeuvre pour la CGVMSL en 1979. Blessé au dos en 1985, il a été assigné à des travaux légers en 1987. Au cours des deux années suivantes, il a reçu deux semaines de formation sur la manoeuvre d'un pont et il a travaillé comme pontier. De 1991 à 1995, il a travaillé comme éclusier. En 1995, il est redevenu pontier. Au moment de l'accident, il travaillait comme pontier au pont 11 depuis 4 ans.
Les douleurs au dos du pontier sont réapparues à plusieurs occasions depuis sa blessure en 1985, le forçant à s'absenter du travail en 1988, en 1990, en 1993 et en 1994. Elles ont été soulagées au moyen de médicaments comme le Tylenol III, le Darvon-N et d'autres analgésiques narcotiques. Le pontier avait changé de médecin en 1998 et son nouveau médecin ne lui avait pas prescrit ce type de médicament. Le Darvon-N pris le matin de l'accident avait été obtenu au moyen d'une ordonnance faite en 1997. Le pontier a déclaré qu'avant ce matin-là, il y avait longtemps qu'il n'avait pas pris de Darvon-N, mais qu'il lui était arrivé de prendre des comprimés anti-stress (Ativan) et anti-douleurs (acide méfénamique) prescrits à sa femme. Il conservait ces deux médicaments dans son casier, dans le poste de commande du pont.
1.13 La Voie maritime du Saint-Laurent
1.13.1 Le Réseau de la Voie maritime du Saint-Laurent
La Voie maritime du Saint-Laurent accueille les navires à fort tirant d'eau depuis 1959 et constitue l'un des plus importants réseaux de transport par voie navigable du monde. La Voie maritime permet aux navires océaniques d'avoir accès à des ports situés à l'ouest du port de Montréal et sur les Grands Lacs. Elle peut accueillir des navires d'une longueur atteignant 225,5 m et d'un tirant d'eau de 8 m. En moyenne, huit à neuf jours de navigation séparent l'ouest du lac Supérieur de l'océan Atlantique, soit une distance d'environ 3 700 km. La saison d'exploitation va habituellement de mars à décembre.
Le passage du lac Ontario au lac Érié se fait par le canal Welland, orienté nord-sud, de 43,4 km de longueur. Le chenal navigable a une largeur de 106,7 m et une profondeur de 9,1 m. Il y a huit écluses qui permettent de franchir une dénivellation totale de 99,5 m et 10 ponts - à travée levante ou à bascule - qui laissent passer la circulation routière et ferroviaire. La hauteur maximale autorisée des navires en transit est de 35,5 m. En 1999, 3 626 navires ont emprunté le canal.
1.13.2 Corporation de gestion de la Voie maritime du Saint-Laurent (CGVMSL)
La responsabilité pour le Canada de l'exploitation de la Voie maritime a été confiée à l'Administration de la Voie maritime du Saint-Laurent (AVMSL). Société d'État fédérale créée en 1954 par une loi du Parlement, l'Administration a été chargée d'acquérir les terrains et de construire les ponts nécessaires afin d'aménager, d'exploiter et d'entretenir une voie navigable en eau profonde reliant le port de Montréal et le lac Érié. Le 1er octobre 1998, après la commercialisation de la Voie maritime, la responsabilité pour le Canada de l'exploitation et de l'entretien de l'infrastructure de la Voie maritime a été transférée de l'AVMSL à la CGVMSL, société sans but lucratif constituée d'usagers de la Voie maritime et d'autres parties intéressées. Le transfert de responsabilité a été réalisé en vertu de la Loi maritime du Canada, aux termes d'une entente renouvelable de 20 ans passée avec le gouvernement du Canada. Aux termes de l'entente mise en place, le gouvernement du Canada conserve la propriété des biens immeubles et la CGVMSL doit présenter un plan quinquennal de renouvellement des actifs. Le nombre d'employés à plein temps de la Voie maritime est passé de 794 en 1998 à 619 employés à la fin de la saison de navigation 2001. Transports Canada (TC) conserve l'autorité réglementaire sur la Voie maritime.
1.13.3 Gestion dans la région du Niagara
La CGVMSL, Région du Niagara, est responsable de l'exploitation générale et de l'entretien du canal, lequel est divisé en trois zones géographiques d'exploitation : le nord, le centre et le sud. L'accident s'est produit dans la zone sud.
Une équipe de gestion des opérations — composée de gestionnaires de secteur, d'un gestionnaire des services maritimes ainsi que de coordonnateurs maritimes et de secteur — appuie les opérations et la gestion du trafic maritime dans le canal.(Dans la zone sud, le gestionnaire de secteur était également gestionnaire des services maritimes.)
Pour gérer les opérations sur le terrain, chaque zone d'exploitation géographique possède un coordonnateur maritime et un coordonnateur de secteur. Le coordonnateur maritime est responsable de la circulation des navires et des contrôleurs de la circulation maritime; le coordonnateur de secteur est responsable de l'entretien général ainsi que des pontiers. Le coordonnateur maritime et le coordonnateur de secteur travaillent de 7 h à 19 h et de 8 h à 16 h, respectivement. De 19 h à 7 h, un seul coordonnateur maritime est de service pour les trois zones d'exploitation.
Les employés travaillent selon un horaire de quatre quarts, dont chacun est dirigé par un chef d'équipe qui relève du coordonnateur de secteur et dont le rôle est d'attribuer le travail aux employés de son équipe. Dans le secteur sud, un chef d'équipe est aussi chargé de faire appel à des employés pour faire des heures supplémentaires.
1.14 Conditions météorologiques et courants
Au moment de l'accident, alors que le crépuscule était imminent, la visibilité était bonne; il n'y avait pas de précipitations et les vents étaient légers. Sous le pont 11, le courant était de moins d'un noeud et portait en direction nord.
1.15 Abaissement de la travée du pont
La travée levante, lorsqu'elle est à son point le plus haut, offre une hauteur libre de 36,5 m au-dessus du niveau de l'eau. Même si le temps requis pour abaisser la travée de son point le plus haut à son point de repos le plus bas, soit une distance de 32,9 m, varie selon les pontiers, l'opération prend généralement de 1,5 à 2 minutes.
La travée était en train de descendre lorsqu'elle a heurté le Windoc au niveau des fenêtres avant de la timonerie, soit à une hauteur d'environ 18,6 m au-dessus du niveau de l'eau. Il faut entre 49 et 65 secondes pour abaisser la travée de 18 m. Comme le navire faisait route à une allure d'environ 5 noeuds, il devait avoir l'avant sous le pont ou juste de l'autre côté lorsque le pontier a commencé à baisser la travée. Il était sans doute possible d'apercevoir (que l'on soit assis ou debout) la superstructure arrière du navire par la fenêtre du poste de commande faisant face au sud (voir les figures 1 et 2 ainsi que les photos 6 et 7).


Légendes des figures 1 et 2 :
Les lignes continues (c.-à-d. ———) indiquent la limite inférieure du champ de vision du pontier lorsque celui-ci est assis au tableau de commande.
Les lignes pointillées (c.-à-d. ---------) indiquent la limite inférieure du champ de vision du pontier lorsque celui-ci est debout au panneau de commande.


Rien ne permet de croire qu'une défectuosité mécanique aurait empêché le fonctionnement normal de la travée au moment de l'accident. Le pontier du quart précédent n'a pas eu de problèmes avec le pont et le pontier impliqué dans l'accident avait lui-même levé et abaissé la travée à deux occasions sans problèmes entre le début de son quart et le moment où il l'a levée pour le Windoc.
Le manuel d'exploitation du pont 11 de la CGVMSL précise qu'on peut abaisser la travée lorsque l'arrière du navire a dépassé le pontNote de bas de page 7. Le pontier a déclaré avoir vu l'arrière du navire par la fenêtre nord du poste de commande (c.-à-d. en regardant vers l'aval) près de la porte.
1.16 Préparatifs d'urgence
1.16.1 Planification d'urgence, formation et exercices
En vertu de la Loi sur la protection civile, il incombe aux ministres fédéraux d'identifier les risques de crise dans leurs champs de compétence respectifs ainsi que d'élaborer un plan de protection civileNote de bas de page 8. La Voie maritime du Saint-Laurent, y compris le canal, relève du ministre des Transports.
Au moment de l'accident, il n'existait pas de plan d'intervention local à jour pour faire face à d'éventuelles situations d'urgence dans le canal. Il existait bien une version provisoire du Plan d'urgence de l'Administration de la Voie maritime du Saint-Laurent en cas de catastrophe ou d'accident majeur, datée du 21 décembre 1992, ainsi qu'un plan d'urgence maritime régional de la CGVMSL, révisé en mars 1999; toutefois, ces deux documents et leurs annexes n'étaient pas à jour. Le plan provisoire en cas de catastrophe ou d'accident majeur comprenait un scénario dans lequel un pont à travée levante était heurté par un navire, mais les modalités d'intervention étaient limitées au pont endommagé uniquement. Il n'était pas question d'autres conséquences possibles reliées au navire, à savoir des accidents et des incidents comme des incendies à bord, une évacuation et de la pollution. L'objet du plan d'urgence maritime régional était de répondre aux déversements de substances dangereuses ou toxiques, ou encore d'autres types de substances, dans le sol ou dans l'eau, dont la responsabilité relevait du CGVMSL. Cela comprenait les déversements provenant de navires empruntant le canal Welland.
Les deux plans définissaient une structure de commandement général des opérations; toutefois, cette structure de commandement ainsi que les personnes préalablement désignées pour en assumer les opérations faisaient partie de la structure organisationnelle en place à l'époque.
Les procédures de signalement d'incendie à bord et les détails de l'aide par le personnel des ponts et des écluses étaient exposés dans le Manuel de contrôle de la circulation, Région du Niagara, 2000 et dans le Manuel d'exploitation — Écluses de la CGVMSL. Les activités de lutte contre l'incendie sont assurées par les services d'incendie locaux. Le genre d'aide apportée consistait essentiellement à diriger les autorités et les services d'incendie locaux vers le lieu du sinistre et à s'assurer que le pont d'un navire à l'intérieur d'une écluse soit élevé ou abaissé à un niveau qui permette l'évacuation de l'équipage.
Aucun des employés de la CGVMSL qui sont intervenus à la suite de l'accident n'avait reçu de formation approfondie en gestion des mesures d'urgence. Certains employés de la CGVMSL avaient suivi une formation du genre, mais celle-ci était restreinte aux mesures antipollution. En 1996, six employés de la Voie maritime ont participé à une demi-journée de formation et d'exercices sur la pollution dans le canal, dispensée par la GCC. Un exercice de déploiement de barrages flottants devait être tenu dans le canal en l'an 2000, mais il a été annulé. D'autres exercices de déploiement de barrages flottants ont été organisés en 1999, 2000 et 2001 dans le secteur Montréal-lac Ontario de la Voie maritime. En 1998, une présentation sur la sécurité relative aux petites embarcations a été donnée par la GCC aux employés de la CGVMSL.
Il n'y a pas trace dans les dossiers d'exercice en cas d'urgence majeure liée à un navire et qui aurait été mené avec d'autres organismes dans le canal depuis 1990, du moins jusqu'au jour de l'accident.
1.16.2 Communications et coordination
Le CCC fournit un réseau de communication centralisé pour les opérations quotidiennes. Deux contrôleurs sont affectés à chaque quart de 12 heures. Lors de situations d'urgence, les contrôleurs du CCC assurent les communications pour la coordination des activités en vue de faire face aux situations d'urgence, tout en s'acquittant de leurs fonctions régulières de gestion du trafic.
Le Manuel de contrôle de la circulation, Région du Niagara, 2000, de la CGVMSL contient des consignes et de l'information touchant les situations d'urgence, et notamment une liste des mesures à prendre lorsqu'un accident est signalé. On y traite aussi de divers sujets, à savoir le signalement des accidents, la lutte contre l'incendie à bord des navires, les échouements, les heurts violents et les abordages, la liste des personnes-ressources de la CGVMSL à rejoindre en cas de besoin, et la pollution de l'environnement. Dans une situation d'urgence, il appartient aux contrôleurs d'assurer l'intervention initiale, lorsqu'il faut agir immédiatement (comme appeler les pompiers, la police et l'ambulance), d'obtenir de l'information sur la situation d'urgence ainsi que d'informer les coordonnateurs appropriés. Le coordonnateur des Services maritimes de la CGVMSL doit, pour sa part, transmettre l'information aux SCTM, lesquels se chargent d'avertir les autres pouvoirs publics. Le coordonnateur des Services maritimes est normalement responsable de l'enquête préliminaire lorsque survient un accident.
1.17 Cause possible de l'incendie
Un film vidéo amateur de l'accident obtenu par le BST montre de nombreux arcs électriques causés par des fils qui se sont rompus lors du heurt violent avec le pont 11. Comme la cheminée a été arrachée du tambour-machines, la tuyauterie d'échappement de la machine principale ainsi que deux génératrices ont été brisées, exposant des tuyaux brûlants et causant le dégagement de gaz d'échappement chauds et de calamine incandescente. Le collecteur d'échappement brûlant, quoique intact, au niveau de la culasse de la machine principale a aussi été exposé au contact avec des vapeurs d'essence s'échappant de la caisse à mazout fendue de l'incinérateur.
1.18 Moyens de lutte contre l'incendie
1.18.1 Équipements de lutte contre l'incendie à bord
L'équipement de lutte contre l'incendie à bord du navire ainsi que l'installation étaient conformes aux exigences réglementaires. L'équipement du bord comprenait :
- une pompe d'incendie principale électrique dans la salle des machines
- une pompe d'incendie de secours à diesel dans le compartiment du propulseur d'étrave
- un système de gicleurs dans les emménagements et une pompe de diffuseurs dans la salle des machines
- un système fixe d'extinction au CO2 dans la salle des machines
- des plans de défense contre l'incendie placés dans la timonerie
Les cloisons des emménagements internes du navire étaient faites principalement de produits du bois, ce qui n'est pas conforme aux normes modernes de protection structurelle contre l'incendie. Pour y remédier, on avait installé partout dans les emménagements un système d'extincteurs automatiques à eau très complet ainsi que des portes coupe-feu dans les puits d'escalier; la Sécurité maritime de TC avait approuvé ces mesures qu'elle considérait comme assurant un niveau de sécurité équivalent. Le réseau de distribution des extincteurs était fixé à des charpentes internes inflammables.
Tous les officiers et les membres de l'équipage, y compris ceux de l'équipage de relève, avaient reçu une formation à la lutte contre l'incendie et aux fonctions d'urgence en mer. Cependant, au moment de l'accident, huit membres de l'équipage étaient descendus à terre et n'étaient pas présents pour lutter contre l'incendie et assumer des fonctions d'intervention d'urgence.
À bord, les duplicata des plans de défense contre l'incendie étaient tous placés à l'intérieur de la structure des emménagements et, à cause de l'incendie, les pompiers n'y avaient pas accès.
1.18.2 Ressources de lutte contre l'incendie à terre
Cinq corps de pompiers municipaux (des municipalités voisines de Port Colborne, Welland et St. Catharines) dont les membres possèdent différents niveaux de connaissances, d'expérience et de formation relativement à la lutte contre l'incendie sur l'eau, étaient disponibles dans le secteur du canal. Les pompiers de Thorold, les premiers à intervenir, possédaient peu ou pas d'expérience ou de formation en matière de lutte contre les incendies à bord de navires et ne disposaient pas d'embarcations capables de transporter les pompiers entre la rive et le Windoc. Le service d'incendie de St. Catharines avait des embarcations, qu'il a mis à la disposition des équipes de lutte contre l'incendie à la demande du chef des pompiers de Thorold.
À cause de l'emplacement relativement éloigné de la position finale du Windoc, aucune conduite d'alimentation en eau municipale n'était accessible pour combattre le feu. On a donc dû se servir de camions-pompes et on s'est servi de l'eau du canal pour arroser le feu à partir des berges. À cause de la hauteur d'aspiration considérable due à la hauteur de la berge du canal, on a éprouvé initialement des difficultés à obtenir une bonne aspiration de la pompe, ce qui fait que le débit et la pression d'eau disponibles pour combattre les flammes étaient moindres que ce qu'on aurait pu espérer.
1.19 Sécurité incendie dans les ports et les havres canadiens ainsi que dans la Voie maritime
Depuis 1989, au moins neufNote de bas de page 9 incendies majeurs ont éclaté à bord de navires de divers types et de différents tonnages au Canada, nécessitant l'intervention des pompiers des municipalités riveraines.
Les accidents mettant en cause le H.M. Griffith, le Ambassador et le Petrolab sont d'un intérêt particulier. Le 27 septembre 1989, un incendie a éclaté dans le tunnel du H.M. Griffith sous la cale à cargaison no 3 alors que le vraquier circulait dans le canal. Un rapport interne de l'AVMSL paru après l'accident fait état de préoccupations touchant les communications et la coordination des efforts de lutte contre l'incendie de l'équipage du navire et des pompiers municipaux. Le rapport recommande que l'AVMSL organise une réunion avec les chefs des corps de pompiers locaux afin d'établir une marche à suivre et de préciser les rôles respectifs de la Voie maritime et des corps de pompiers municipaux. Au moment de l'accident du Windoc, il n'existait pas encore de marche à suivre ni de protocole d'entente entre la CGVMSL et les corps de pompiers riverains dans la région du canal.
Lors d'un autre accident en décembre 1994, un incendie a éclaté dans le transporteur à courroie du vraquier Ambassador pendant le déchargement d'une cargaison de phosphate de chaux naturel dans le port de Belledune au Nouveau-Brunswick. L'équipage du navire et plusieurs corps de pompiers riverains ont dû travailler main dans la main pour maîtriser l'incendie qui a été éteint complètement au bout de 28 heures.
Dans les ports canadiens, la responsabilité de l'évaluation des risques et des plans d'urgence incombe généralement au responsable du port local, alors que la lutte contre l'incendie est assurée par le corps de pompiers local. Préoccupé par le fait que de nombreux corps de pompiers municipaux n'ont pas nécessairement de personnel bien entraîné à la lutte contre les incendies à bord de navires, le Bureau avait recommandé que :
Le ministère des Transports entreprenne une vérification spéciale des installations de lutte contre l'incendie dans les ports et les havres du Canada sous sa juridiction afin de s'assurer qu'elles permettent de maîtriser les incendies à bord des navires peu importe la période de l'année.
Recommandation M96-06 du BST (publiée en octobre1996)
et que Le ministère des Transports, en collaboration avec les administrations locales des ports et havres, prenne des mesures afin de s'assurer que les services d'incendie externes qui peuvent être appelés à prêter assistance pour combattre un incendie à bord d'un navire reçoivent une formation appropriée.
Recommandation M96-07 du BST (publiée en octobre 1996)
et que Le ministère des Transports prenne les mesures qui s'imposent pour s'assurer que les navires qui font escale dans les ports et les havres du Canada ont des moyens de lutte contre l'incendie à bord en état de fonctionner et qui peuvent être promptement utilisés même par temps froid.
Recommandation M96-08 du BST (publiée en octobre 1996)
TC a répondu que c'est l'Association canadienne des chefs de pompiers (ACCP) qui est responsable de la compétence et de l'entraînement des corps de pompiers à terre. L'ACCP n'a aucun droit de regard sur les corps de pompiers non membres. La majorité des ports publics ne possèdent qu'un corps de pompiers bénévoles capables de combattre de petits incendies et dont les membres ne sont généralement pas entraînés à entrer dans des espaces fermés pour y combattre des incendies. TC a aussi indiqué que la loi n'oblige pas les ports publics à mener des activités de lutte contre l'incendie à bord des navires. Depuis l'an 2000, TC a entrepris des initiatives visant à améliorer les mesures de lutte contre l'incendie à bord de navires dans les ports et les havres (voir le paragraphe 4.1.4).
En mai 1997, l'ACCP a envoyé un questionnaire à des municipalités choisies afin de déterminer leur capacité de lutte contre l'incendie de même que le type et la qualité de l'aide sur laquelle pouvaient compter les exploitants de terminus maritimes si un incendie éclatait à bord d'un navire au port. Selon l'information fournie au BST, les corps de pompiers de la région du canal n'ont pas reçu ce questionnaire et n'ont donc pas pu participer à l'enquête. L'AVMSL n'a pas été avisée de ces initiatives en 1997. Dans l'ensemble, le sondage n'a pas connu une diffusion assez large pour fournir les renseignements utiles permettant d'évaluer le degré d'expérience de la lutte contre les incendies de navires dans les corps de pompiers municipaux.
Dans la soirée du 19 juillet 1997, une explosion s'est produite et un incendie a éclaté à bord du pétrolier Petrolab à St. Barbe (Terre-Neuve) alors que l'équipage était en train de laver des citernes de cargaison avant de charger du mazout. Le propriétaire du navire a été tué et trois membres de l'équipage ont été blessés dans l'explosion; un de ceux-ci est mort plus tard à l'hôpitalNote de bas de page 10. L'incendie qui a éclaté à bord du navire après l'explosion s'est propagé au quai de l'État. Il a fallu les efforts combinés de deux navires de la GCC et de plusieurs corps de pompiers riverains pour maîtriser les flammes. Le navire et le quai de l'État ont été détruits avant qu'on ne réussisse à éteindre complètement l'incendie quelque 63 heures plus tard.
L'enquête ultérieure a révélé que le service d'incendie local n'était pas muni de système d'extinction à mousse et que ses membres n'étaient pas entraînés à combattre des incendies de navires, spécialement des incendies à bord de pétroliers. Les pompiers n'ont donc pas été capables de maîtriser rapidement l'incendie et le feu s'est propagé dans la peinture extérieure de la coque du navire pour finalement se communiquer aux pilotis imprégnés de créosote du quai de l'État.
D'autres accidents ultérieurs, en particulier des feux de cargaison à bord du Southgate en 1998 et du Vaasaborg en 2001, ont fait ressortir encore davantage les lacunes des moyens de lutte contre les incendies de navires des corps de pompiers riverains.
1.20 Autres mesures de sécurité visant des postes importants pour la sécurité
Dans l'industrie du transport, les capacités physiques et mentales d'une personne qui occupe un poste essentiel pour la sécurité sont cruciales. Les gens de mer canadiens doivent subir un examen médical à intervalles prescrits afin de maintenir la validité de leurs brevets et certificatsNote de bas de page 11. La publication Examens médicaux des navigants - Guide du médecin (TP 11343) précise les facteurs qui doivent être pris en compte lors des examens médicaux ainsi que les critères physiques et les tests permettant d'établir si un navigant répond aux exigences. Une analyse d'urine doit être faite périodiquement lorsqu'elle est cliniquement justifiée; on ne doit cependant pas s'en servir pour le dépistage des drogues.
En mars 1991, le BST a fait enquête sur un abordage entre un brise-glace et un bateau de pêcheNote de bas de page 12. Le Bureau n'a établi aucun lien entre les problèmes médicaux du capitaine du brise-glace ou les médicaments qu'il aurait pris et l'accident. Le Bureau s'est cependant inquiété de l'absence d'un mécanisme en bonne et due forme permettant d'identifier et de surveiller les personnes qui occupent des postes critiques pour la sécurité et qui ne sont pas médicalement aptes à exercer leurs fonctions. Préoccupé par l'absence de surveillance formelle d'un membre d'équipage du navire occupant un poste critique pour la sécurité qui prenait des médicaments sur ordonnance ainsi que par l'absence d'examen médical officiel exigé d'une personne exerçant des fonctions critiques pour la sécurité qui reprend le travail au retour d'une absence du travail causée par le stress, le Bureau avait recommandé que :
Le ministère des Transports, en collaboration avec Santé Canada et la Garde côtière canadienne, établisse des politiques et des procédures pour s'assurer que les personnes qui reprennent des fonctions critiques pour la sécurité après avoir suivi un traitement médical quelconque sont aptes à exercer de telles fonctions.
Recommandation M95-05 du BST (publiée en juillet 1995)
Depuis cette recommandation, la GCC exige que les membres de ses équipages se soumettent à un examen médical avant certains voyages et après s'être absentés du travail pour cause de maladie ou de blessure. Les personnes jugées inaptes à exercer leurs fonctions ne pourront réintégrer le personnel navigant avant d'être réévaluées et jugées aptes par un médecin. Le Règlement sur l'armement en équipage des navires, qui ne s'applique pas à la GCC, a été modifié pour habiliter le ministre des Transports à exiger un nouvel examen médical d'un navigant à la demande du navigant ou de son employeur.
Avant la délivrance ou la revalidation d'une licence de pilote d'aéronef commercial canadien, le candidat doit subir un examen médical annuel et il ne doit pas être soumis aux effets ou aux effets secondaires d'un quelconque médicament pris sur ordonnance ou sans ordonnanceNote de bas de page 13.
Le 19 décembre 2001, TC a annoncé l'entrée en vigueur du Règlement médical des chemins de fer pour les employés occupant des postes classifiés comme essentiels pour la sécurité ferroviaireNote de bas de page 14. Le règlement établit un nouveau processus d'évaluation médicale et définit des exigences d'aptitude médicale pour les employés exerçant des fonctions essentielles pour la sécurité. Un manuelNote de bas de page 15 a été préparé pour fournir aux compagnies ferroviaires canadiennes et aux prestataires de services médicaux les renseignements nécessaires à la mise en application des Règles. Un autre document intitulé Règlement concernant les postes classifiés comme essentiels pour la sécurité ferroviaire a aussi été élaboré; on y trouve une définition de postes classifiés comme essentiels pour la sécurité ferroviaire et on y précise le type de dossiers que doit conserver l'employeur pour les employés aptes à occuper des postes essentiels pour la sécurité.
Aux États-Unis, le NTSB a fait enquête sur deux accidents semblables impliquant des véhicules légers sur rail qui sont survenus au même endroit à tout juste six mois d'intervalle. L'enquête a révélé que les deux conducteurs en cause dans les accidents étaient revenus de congé de maladie prolongé peu avant leur accident. On leur avait prescrit des médicaments qui pouvaient avoir des effets secondaires comme de la fatigue et de la somnolence. Étant donné que l'enquête a révélé que l'autorité n'exigeait pas que les employés occupant des postes critiques pour la sécurité fassent savoir qu'ils prennent des médicaments sur ordonnance ou en vente libre avant de faire fonctionner de l'équipement, le NTSB a conclu que l'autorité ne possédait pas toute l'information pouvant avoir une incidence sur la condition et le rendement de tels employés. Par conséquent, le 23 janvier 2001, le NTSB a fait la recommandation suivante (R-01-25) à la Federal Transit Authority des États-Unis :
[Traduction] Il faudrait autoriser et encourager les réseaux de transport en commun sur rail à exiger que leurs employés occupant des postes essentiels pour la sécurité les informent lorsqu'ils prennent des médicaments sur ordonnance ou en vente libre afin que l'entreprise puisse faire évaluer par du personnel médical qualifié les effets possibles des médicaments sur le rendement de l'employé.
À la suite de la recommandation du NTSB, la réponse de la Federal Transit Authority indique que celle-ci a pris un certain nombre de mesures pour satisfaire à cette recommandation, comme la mise sur pied d'un programme d'aide destiné au secteur du transport en commun relativement aux dangers possibles de la prise de médicaments. Des trousses contenant des aide-mémoire, du matériel pédagogique et de la documentation sur les contre-indications médicales étaient également en voie de préparation pour la formation des gestionnaires, des superviseurs et des employés du secteur des transports en commun.
La CGVMSL n'avait aucune consigne pour obliger les employés occupant des postes essentiels pour la sécurité à faire l'objet d'une surveillance médicale ou à faire savoir lorsqu'ils prennent des médicaments sur ordonnance.
2.0 Analyse
2.1 Conscience de la position du navire
Le pontier n'a répondu ni à l'appel radio VHF du Windoc ni aux coups de sifflet destinés à lui faire prendre conscience que le navire était toujours engagé sous le pont. Le pontier n'a probablement pas pu entendre le message radio VHF car le poste de commande du pont est très bruyant lorsque la travée mobile est en mouvement. Selon les constatations que les enquêteurs du BST ont faites dans le poste de commande du pont 21, très semblable à celui du pont 11, le niveau de bruit maximal mesuré pendant que la travée est abaissée normalement atteint 92,5 décibels pondérés en gamme A (dBA)Note de bas de page 16. D'autres pontiers ont indiqué qu'il leur arrivait d'entendre les transmissions VHF pendant que la travée était en mouvement mais qu'il leur était impossible d'en saisir le contenu. Dans le cas à l'étude, compte tenu du fait que le sifflet était très près du pont, ainsi que de la tonalité aiguë et du niveau de décibels du sifflet, le pontier aurait dû pouvoir entendre le sifflet du navire. Des personnes demeurant en amont du pont ont déclaré être sorties de leur maison pour connaître la raison des coups de sifflet répétés.
Quoi qu'il en soit, le pontier a déclaré avoir vu l'arrière du navire par la fenêtre nord du poste de commande (où se trouve la porte). Si tel avait été le cas, le navire aurait été sorti du pont au moment où la travée a été abaissée. L'analyse de la position du navire avant et pendant l'impact montre que le Windoc était clairement visible dans la fenêtre sud du poste de commande lorsque le pontier a commencé à abaisser la travée (voir le paragraphe 1.15, figures 1 et 2).
2.2 Effets des médicaments et de l'alcool sur le rendement du pontier
Aucune analyse toxicologique n'ayant été faite après l'accident, il n'a pas été possible de déterminer avec précision les substances qui auraient pu influer sur le comportement du pontier. En présumant que le taux de transformation métabolique du Darvon-N a été normal, le pontier devait avoir du propoxyphène et du norpoxyphène dans son organisme au moment de l'accident. Sans résultat d'analyse toxicologique, on n'a pu déterminer les concentrations précises des substances en question. Et même si on avait un résultat d'analyse toxicologique, il ne serait pas possible de déterminer à coup sûr les effets de ces substances sur le rendement à cause des nombreuses variables qui influencent la rapidité avec laquelle une personne métabolise ces substances ainsi que l'impact de ces substances sur le rendement humain.
Les résultats des analyses quantitatives réalisées par le groupe d'analyse de la parole du NTSB étaient sensiblement affectés par le manque d'échantillons définitifs de la parole du pontier à l'état normal. Même si on lui a fourni des échantillons de communications faites pendant les mois précédant l'accident, le groupe d'analyse de la parole ne pouvait pas être sûr que les paroles prononcées sur ces échantillons n'étaient pas affectées par les effets de la fatigue et d'autres facteurs confusionnels. Les membres du groupe d'analyse de la parole ont noté plusieurs cas dans l'échantillon de référence où le pontier ne semblait pas totalement alerte. On n'a donc pas pu observer de changements dans les propriétés physiques de la parole du pontier qui indiqueraient que ses facultés étaient affaiblies temporairement par l'alcool, les médicaments ou la fatigue. On n'a pas relevé de différences statistiquement significatives dans la fréquence fondamentale, le débit ou la latence, ni d'erreurs lors de la comparaison des échantillons de paroles de la nuit de l'accident avec les échantillons de référence des mois précédents.
Un autre examen réalisé par le groupe d'analyse de la parole a porté sur le contenu et la qualité des paroles du pontier la nuit de l'accident. Cet examen a révélé des indices qui ont été associés à une diminution du rendement causée par l'alcool et les médicaments prescrits. Le groupe a noté une détérioration de l'intelligibilité des paroles du pontier entre le moment où le pontier a pris son quart à 18 h 30 le jour de l'accident et la période précédant immédiatement l'accident. Une analyse spectrographique a révélé que le pontier articulait moins bien ou avait la voix plus pâteuse dans les communications qui ont précédé l'accident que dans les communications antérieures le même soir. En ce qui concerne la parole du pontier au moment de l'accident, le groupe a noté ce qui suit :
[Traduction] . . . le débit du pontier semblait précipité et ses paroles étaient parfois difficiles à comprendre avant l'accident. Comparativement à des échanges antérieurs au cours desquels le pontier échangeait des plaisanteries cordiales avec ses collègues, le pontier semblait avoir l'esprit plus lent et son expression ainsi que le ton de sa voix n'étaient pas toujours adaptés à ceux des interlocuteurs. À deux reprises, il a mal identifié un collègue (avec lequel il venait de plaisanter), et a semblé confus relativement aux problèmes avec le téléphone ainsi qu'à l'accident lui-mêmeNote de bas de page 17.
Ces observations du comportement du pontier pendant la période entourant l'accident laissent croire que le rendement de celui-ci pouvait être diminué lorsqu'il a décidé d'abaisser la travée mobile. Selon la définition du document DSM IVNote de bas de page 18, l'intoxication par les drogues ou les médicaments provoque [Traduction] « un comportement mésadapté ou des changements psychologiques significatifs du point de vue clinique dus aux effets du médicament ou de la drogue sur le système nerveux central (p. ex. belligérance, instabilité d'humeur, diminution des facultés intellectuelles, détérioration du jugement, détérioration du fonctionnement social ou professionnel). » Selon le DSM IV, l'intoxication par l'alcool provoque les mêmes effets, auxquels s'ajoutent un ou plusieurs des symptômes suivants : voix pâteuse, manque de coordination, démarche instable, nystagmus, manque d'attention ou de mémoire, stupeur ou coma.
Si l'on en juge par les communications enregistrées au cours de la période entourant l'accident, l'état de confusion du pontier, sa voix pâteuse, ses trous de mémoire et sa mauvaise évaluation de la gravité de l'accident sont typiques d'une intoxication aux médicaments ou aux drogues et/ou à l'alcool. Les commentaires des contrôleurs du CCC après leur conversation avec le pontier montrent qu'ils ont envisagé cette possibilité. Il est donc probable que le rendement du pontier était diminué lorsqu'il a abaissé la travée sur le Windoc.
2.3 Aptitude des titulaires de postes essentiels pour la sécurité à remplir leurs fonctions
Il est essentiel que les personnes qui occupent des postes où leur comportement peut avoir un impact majeur sur la sécurité des personnes, des biens matériels ou de l'environnement soient aptes à s'acquitter de leurs tâches. On n'a pas procédé à l'identification des postes essentiels pour la sécurité puisque la CGVMSL considérait comme tels tous les postes liés à l'exploitation et à l'entretien, étant donné la nature du travail. Toutefois, aucune mesure n'a été prise pour s'assurer que les personnes qui occupent ce genre de poste sont compétentes et aptes à faire leur travail.
Au moment de l'accident, les nouveaux employés embauchés par la CGVMSL passaient un examen médical préalable, lequel comprenait une évaluation en physiothérapie ainsi qu'un examen standard de leur dossier médical. Après cet examen médical, les employés permanents n'étaient pas réévalués périodiquement à moins de raisons précises, comme par exemple dans le cas d'un employé qui reprend son poste après une blessure au travail, circonstance où les employés sont tenus de fournir un certificat médical. La décision touchant l'aptitude à remplir les fonctions était prise par un médecin contractuel après une évaluation clinique de l'information soumise. Lorsque la CGVMSL n'était pas satisfaite de l'information fournie par le médecin de l'employé selon laquelle ce dernier était apte à faire son travail, on envoyait alors l'employé subir un examen par un médecin désigné exerçant en cabinet.
La divulgation de la prise de médicaments était, dans ces cas, laissée à la discrétion de l'employé. Rien n'empêchait l'employeur de demander à l'employé s'il prenait des médicaments, mais celui-ci n'était pas tenu de le révéler de lui-même. L'effet possible de la prise de médicaments sur le rendement d'un employé était pris en compte dans la décision de permettre à celui-ci de reprendre son poste. Pour que cette information reste confidentielle, et conformément aux dispositions législatives en matière de droits de la personne et de protection des renseignements personnels, c'est l'infirmière en santé du travail qui en était dépositaire. Les superviseurs et les gestionnaires étaient informés lorsqu'un employé était jugé apte à reprendre le travail, on leur indiquait toute diminution de ses habiletés, le cas échéant, mais sans préciser les conditions pathologiques particulières ni les médicaments que l'employé pouvait prendre. Ces mêmes modalités valaient pour tous les postes de la CGVMSL.
Le pontier impliqué dans l'accident à l'étude possédait des antécédents de douleurs lombaires chroniques depuis qu'il avait été blessé au dos en 1985. Ses malaises l'avaient obligé à s'absenter du travail de façon répétée et on lui avait prescrit du repos et des analgésiques comme le Darvon-N et d'autres narcotiques. Les dossiers médicaux de la CGVMSL concernant le pontier ne faisaient nulle mention du fait que celui-ci prenait du Darvon-N.
Le Darvon-N a des effets sur le système nerveux central et les patients qui en prennent sont avertis que le médicament peut diminuer leurs capacités physiques ou mentales et les rendre, de ce fait, moins aptes à exécuter des tâches pouvant être dangereuses comme conduire un véhicule automobile ou faire fonctionner des machines. Un médecin du travail ne permettrait normalement pas à quelqu'un qui prend régulièrement du Darvon-N d'occuper un poste essentiel pour la sécurité. Cependant, pour porter un jugement éclairé, il faut que le médecin soit au courant du médicament pris ainsi que du fait que l'employé exerce des fonctions essentielles pour la sécurité. Sans obligation de faire connaître les médicaments pris et sans mécanisme pour identifier les fonctions essentielles pour la sécurité, il est peu probable que le médecin puisse prendre une décision éclairée. Le régime en place pour contrôler l'aptitude des employés à exercer leurs fonctions, particulièrement ceux qui occupent des postes essentiels pour la sécurité, laissait donc à désirer.
2.4 Supervision des employés
Le pontier était le seul qui pouvait et devait s'assurer qu'il n'y avait pas de navire sous le pont avant d'abaisser la travée mobile. La formation et la supervision des pontiers étaient donc importantes pour assurer la sécurité aux ponts de la Voie maritime du Saint-Laurent.
Les employés deviennent normalement pontiers lorsqu'ils possèdent assez d'ancienneté pour être admissibles à la formation, laquelle est donnée en grande partie en cours d'emploi par un pontier expérimenté. Avant d'être admissible à travailler comme pontier, l'employé doit avoir passé un examen écrit sur la façon de lever et d'abaisser la travée mobile en situation normale et d'urgence et il doit actionner celle-ci dans les diverses circonstances en présence d'un coordonnateur. Une fois le nouveau pontier qualifié, il n'est pas obligé de suivre de formation de rafraîchissement ni de se requalifier. Un employé travaille normalement comme pontier de relève jusqu'à ce qu'il ait accumulé assez d'ancienneté pour occuper lui-même à plein temps un poste de pontier. Beaucoup de temps peut s'écouler entre le moment où un employé se qualifie pour faire fonctionner le pont et celui où il devient titulaire du poste.
Une fois confirmés dans leur poste, les pontiers font des quarts de 12 heures, seuls sur le pont. Ils ne communiquent avec le CCC que par téléphone ou par radiotéléphone VHF et avec un coordonnateur lors d'une visite au pont. Les coordonnateurs ne sont pas tenus de regarder fonctionner le pont au cours de leurs visites, lesquelles n'ont normalement pas lieu la nuit à moins de problème particulier.
Cette façon de procéder fait que les coordonnateurs et les gestionnaires ont très peu d'occasions d'observer les employés pour voir s'ils sont compétents et aptes à remplir leurs fonctions. Il est difficile pour un superviseur/gestionnaire de déceler les employés qui ont des difficultés à faire leur travail.
Il existe peu de procédures officielles pour contrôler le rendement et la sécurité entre pairs. Les changements de quart sur les ponts se font de manière informelle. L'absence de procédure spécifique en matière de changement de quart ne laisse que peu d'occasions au pontier d'observer la capacité de son remplaçant à remplir ses fonctions.
Les contrôleurs du CCC ont de fréquentes interactions verbales avec les pontiers; toutefois, la nuit de l'accident, les contrôleurs de service n'ont informé personne de leur inquiétude concernant l'état du pontier ni pris de mesures pour s'assurer que celui-ci était apte à poursuivre son travail.
En somme, les pontiers travaillent très souvent seuls et la direction n'a pas beaucoup d'occasions de s'assurer qu'ils s'acquittent de leurs fonctions correctement et en toute sécurité.
2.5 Capacités de lutte contre l'incendie du navire et des corps de pompiers municipaux
À cause de la rapidité avec laquelle un incendie peut se propager à bord d‘un navire, il est capital que le brasier soit circonscrit dès sa découverte. Après l'explosion du mélange air/combustible dans la partie supérieure du tambour-machines et sur le pont des embarcations du Windoc, l'alimentation en combustible du feu s'est trouvée limitée. Les enregistrements magnétoscopiques de l'accident montrent que les opérations de lutte contre l'incendie menées par l'équipage du navire ont réussi à circonscrire et à réduire le feu sur le pont des embarcations.
Le capitaine, craignant l'explosion de la caisse journalière de carburant dans la salle des machines et voyant les pompiers municipaux qui arrivaient sur la berge du canal, a ordonné à ses équipes de lutte contre l'incendie de se mettre à l'abri à l'avant de la superstructure des emménagements. Les pompiers des environs n'avaient cependant pas d'embarcations pour se rendre jusqu'au Windoc et y monter.
Même si les manches à incendie du navire ont été fixées de façon à circonscrire l'incendie, les efforts pour éteindre le feu ont été retardés de plusieurs heures, le temps que les pompiers à terre obtiennent des embarcations pouvant les transporter jusqu'au navire, ce qui a permis au feu de se propager aux emménagements dont la charpente était inflammable.
Pour assurer l'étanchéité du navire par gros temps, on bouche toutes les ouvertures des navires. Les mêmes dispositifs qui permettent de rendre un navire étanche, comme les portes étanches et les volets d'obturation, permettent aussi de rendre le navire hermétique en cas d'incendie. Grâce aux premiers efforts de lutte contre l'incendie et à la promptitude avec laquelle l'équipage du Windoc a fermé les volets d'obturation de même que les portes étanches/coupe-feu, l'incendie était circonscrit dans le tambour-machines et la partie arrière des emménagements lorsque les équipes de pompiers municipaux sont montées à bord à 1 h 30 le 12 août.
Les pompiers municipaux sont arrivés rapidement sur les lieux de l'incendie; toutefois, une fois sur les lieux, les pompiers ont dû affronter une situation à laquelle leur entraînement à terre ne les avait pas préparés. À cause de l'étanchéité à l'eau de la structure des emménagements, l'eau projetée sur le navire depuis la grande échelle était peu efficace, sinon pour assurer un refroidissement périphérique. Une fois à bord, les pompiers municipaux ont hésité à pénétrer dans les emménagements en flammes et ne se sont pas rendu compte que les flammes étaient en partie circonscrites par l'étanchéité à l'air assurée par les volets d'obturation et les portes étanches. Se fiant à leur entraînement et à leur expérience, les pompiers municipaux ont cru que s'ils ouvraient les portes étanches, cela permettrait d'évacuer la fumée, mais cela a eu pour effet d'assurer un apport d'air frais au feu qui s'est rapidement propagé vers l'avant dans la superstructure des emménagements. Le manque de formation et d'expérience des pompiers municipaux dans la lutte contre l'incendie à bord de navires et le fait que les pompiers ne disposaient pas de l'équipement nécessaire pour parvenir au navire ont gêné la lutte contre l'incendie.
Il y avait à bord plus d'un exemplaire du plan de défense contre l'incendie. Comme tous les exemplaires des plans étaient placés à l'intérieur de la superstructure, à l'arrière, ils étaient hors d'accès au moment de l'incendie. Un plan de défense contre l'incendie comprend généralement des renseignements sur l'emplacement des coupe-feu, des systèmes d'extincteurs automatiques à eau, du matériel d'extinction (comme les prises d'eau, les manches à incendie, le raccord international de jonction avec la terre, etc.), le système de ventilation et l'accès aux différents compartiments. Tous ces renseignements sont essentiels pour prendre des décisions éclairées pour lutter efficacement contre un incendie, car chaque seconde compte. D'après les règles élémentaires du matelotage, un exemplaire du plan de défense contre l'incendie devrait toujours être placé dans un conteneur étanche à l'extérieur du rouf de sorte qu'il soit accessible au personnel riverain luttant contre l'incendie. L'avantage d'une telle pratique a été reconnu par l'Organisation maritime internationale (OMI) et est mentionnée dans la règle 20 du chapitre II-2 de la Convention internationale pour la sauvegarde de la vie humaine en mer (convention SOLAS), dans la circulaire 451 du Comité de la sécurité maritime (MSC/Circ. 451), Guidance concerning the Location of Fire Control Plans for Assistance of Shoreside Fire-fighting Personnel, ainsi que dans les règlements de TC touchant les navires visés par la convention SOLAS. Malgré les avantages d'une telle exigence pour la sécurité, les navires non-visés par la convention SOLAS comme le Windoc ne font pas l'objet des mêmes considérations.
L'installation d'un système d'extincteurs automatiques à eau dans les emménagements à bord des navires plus anciens vise à assurer un niveau de sécurité équivalent lorsque les cloisons et les structures internes des emménagements renferment des matériaux combustibles. Toutefois, l'efficacité de ce genre d'installation peut être compromise si le réseau de distribution n'est pas fixée à des surfaces inflammables. L'examen du Windoc après l'incendie a révélé que le réseau de distribution des extincteurs à eau était relié à des composants combustibles des emménagements, dont la destruction par les flammes a entraîné l'effondrement du réseau et a rendu le système inutilisable.
2.6 Préparatifs d'urgence
La planification, la formation et l'organisation d'exercices au niveau local sont les meilleurs moyens de se préparer à faire face à des situations de crise. Les stratégies susceptibles de favoriser une intervention adéquate et mesurée en situation de crise doivent être consignées dans un plan d'urgence, pour le bénéfice de toutes les personnes qui pourraient avoir à mener de telles opérations, parce que les décisions doivent être prises à l'avance afin d'assurer une intervention rapide. L'état de préparation peut être encore amélioré grâce à de la formation et à l'organisation périodique d'exercices qui permettent de déceler les lacunes du plan. La formation permet au personnel d'être prêt à intervenir. Les exercices permettent de vérifier le bien-fondé des décisions et d'améliorer l'état de préparation général.
En général, l'intervention d'urgence comprend cinq phases :
- la phase d'alerte et d'avertissement (personnel, ressources et pouvoirs publics);
- la phase d'évaluation de la situation et de mobilisation du personnel et des ressources;
- la phase des opérations d'intervention proprement dites;
- la fin de l'intervention;
- le débreffage du personnel de l'évaluation de l'intervention.
Les modalités de chacune de ces phases doivent être exposées de façon détaillée dans un plan d'urgence. En pratique, ces phases se chevauchent souvent lors de l'intervention sur le terrain. Des problèmes et des lacunes ont été notés au niveau des préparatifs d'urgence à la CGVMSL et au niveau des services d'incendie et ambulanciers de Thorold et de St. Catharines.
2.6.1 Corporation de gestion de la Voie maritime du Saint-Laurent
Les plans d'urgence de la CGVMSL préparés pour faire face à des situations d'urgence touchant des navires sur le canal étaient inadéquats et désuetsNote de bas de page 19. Ils n'ont pas été utilisés au moment de l'accident et ils n'étaient pas facilement accessibles au personnel, dont certains membres n'en connaissaient même pas l'existence.
La prompte communication de renseignements capitaux est primordiale pour l'efficacité des services d'urgence, spécialement lorsque la vie humaine et les biens matériels sont menacés et lorsqu'il est question d'évacuer un secteur. Environ trois minutes après que la travée du pont 11 eut heurté le Windoc, les contrôleurs du CCC ont commencé à répondre à des appels de la police, du service d'incendie et des services ambulanciers s'enquérant de l'accident. Les contrôleurs du CCC, qui avaient déjà parlé au pontier du pont 11 et savaient que la travée mobile avait été abaissée sur le navire, n'ont communiqué qu'une partie de l'information dont ils disposaient alors. Les renseignements touchant l'état du pontier n'ont pas été transmis aux services d'urgence. De plus, les renseignements concernant le navire et sa cargaison n'ont été communiqués que lorsque le service d'incendie en a fait la demande.
Les caméras de la CGVMSL ne permettaient pas aux contrôleurs de bien voir le navire et le pont, et ceux-ci ne se sont pas renseignés auprès des services d'urgence ou du personnel de la CGVMSL présents sur place. Par conséquent, les intervenants qui étaient en contact avec les contrôleurs du CCC en se dirigeant vers le lieu de l'accident n'ont pas été informés des détails de l'accident et n'étaient pas en mesure de se préparer à intervenir dès leur arrivée. L'obtention de renseignements sur l'état et la position du navire aurait aidé à la coordination des services d'urgence et de l'intervention du personnel de la CGVMSL.
Il n'y avait ni protocole de communication ni liste de rappel ou d'avertissement qui aurait aidé les contrôleurs du CCC à prévenir les services et organismes d'intervention d'urgence. Une liste de permanence à domicile pour la période du 10 au 17 août 2001 existait et avait été fournie aux contrôleurs du CCC. Sur cette liste ne figuraient que des membres du personnel de la CGVMSL et il s'agissait surtout de personnes-ressources pour des questions d'exploitation courantes. Le Manuel de contrôle de la circulation, Région du Niagara, 2000 renseigne sur la façon de signaler les accidents et les incidents; les contrôleurs du CCC doivent transmettre les renseignements pertinents au coordonnateur des services maritimes qui, lui, retransmettra l'information à la GCC.
Les pouvoirs publics — TC, la GCC, le CID du ministère de l'Environnement de l'Ontario, Environnement Canada et le BST — n'ont pas été informés immédiatement de l'accident. Hormis le BST, ces parties intéressées ont appris la nouvelle de l'accident à la suite de demandes de renseignements faites par les médias environ une heure après l'accident. Lorsque les représentants des pouvoirs publics ont appelé le CCC pour avoir des informations complémentaires, les contrôleurs ne leur ont pas donné tous les renseignements qu'ils avaient. Ce retard à communiquer avec les pouvoirs publics a augmenté le risque de blessures, de dommages matériels et de pollution de l'environnement.
La disponibilité et le déploiement rapide de barrages de rétention des hydrocarbures sont capitaux pour minimiser les dommages à l'environnement que peut causer le déversement de polluants dans l'eau. Dans le cas qui nous occupe, il a fallu six heures pour trouver et déployer un barrage de rétention des hydrocarbures. L'absence de dispositions préalables pour l'acquisition d'équipement d'intervention a accru encore davantage le risque de blessures, de dommages matériels et de pollution de l'environnement.
Les exercices menés en 1996 ainsi que les exercices de déploiement de barrages flottants, avaient une portée limitée, de sorte que l'efficacité de l'intervention d'urgence multi-organismes n'a pas pu être évaluée correctement. C'est ce qui ressort de l'absence de plan d'urgence approprié et à jour pour faire face à des situations d'urgence à bord de navires et du manque de formation spécifique aux situations d'urgence du personnel de la CGVMSL, facteurs qui sont parmi les causes des difficultés éprouvées au cours de l'intervention relative à cet accident.
Essentiellement, l'intervention de la CGVMSL a consisté en une série de mesures ad hoc, ce qui a gêné la coordination et retardé le déploiement de l'équipement et du personnel d'intervention.
2.6.2 Utilisation efficace des ressources de lutte contre l'incendie
Les incendies de navire sont assez rares dans la plupart des juridictions; bien des corps de pompiers municipaux n'ont jamais eu l'occasion d'intervenir dans une telle situation. S'ils devaient être appelés à combattre un incendie à bord d'un navire, il serait cependant vital qu'ils bénéficient au préalable d'une familiarisation avec les navires et les caractéristiques des incendies de navire. De plus, les centres d'intervention d'urgence devraient être au courant des capacités et de l'expérience des unités d'intervention qu'ils envoient.
Le pont 11 se trouve sur le territoire du service d'incendie de Thorold, le seul des cinq services d'incendie de la région du canal dont les membres n'ont ni expérience ni formation dans la lutte contre les incendies de navire.
Sur la terre ferme, l'usage veut que le premier corps de pompiers qui arrive sur les lieux d'un incendie assume le commandement général de l'intervention. Il lui incombe alors de bien examiner la situation à la lumière des connaissances, de l'expérience et des capacités de ses membres, quitte à demander de l'aide si nécessaire. Hormis une demande d'embarcation, aucune aide n'a été sollicitée des services d'incendie voisins, pourtant plus expérimentés; en conséquence, les ressources de lutte contre l'incendie disponibles dans le secteur du canal n'ont pas été utilisées efficacement afin de contenir et d'éteindre l'incendie à temps pour empêcher la destruction des emménagements du navire.
2.6.3 Communications du navire avec la Voie maritime et/ou le pont 11
En cas de problème avec les opérations de la Voie maritime, des communications directes, claires et rapides constituent un moyen d'assurer la sécurité. Lors d'un appel radio destiné à prévenir le CCC que la travée était abaissée, le capitaine du Windoc ne s'est pas identifié et n'a pas précisé de quel pont il s'agissait. Toutefois, il était dans la timonerie d'un navire qui approchait rapidement d'un pont dont on était en train d'abaisser la travée et il voulait transmettre des avertissements le plus rapidement possible. Même si des procédures de radiocommunication standard avaient été suivies, cela n'aurait probablement pas suffi à alerter le pontier. Les machines des ponts à travée levante du canal sont si bruyantes qu'il est presque impossible aux pontiers de saisir le contenu des radiocommunications VHF.
3.0 Faits établis
3.1 Faits établis quant aux causes et aux facteurs contributifs
- Le Windoc qui approchait était visible du poste de commande lorsque le pontier a commencé à abaisser la travée mobile.
- Le rendement du pontier était probablement diminué au moment de l'accident.
- La Corporation de gestion de la Voie maritime du Saint-Laurent (CGVMSL) n'avait pas identifié les postes essentiels pour la sécurité ni défini de critères à cet égard, et le système mis en place ne permettait pas de s'assurer que les personnes qui occupent ces postes étaient compétentes et aptes à remplir leurs fonctions.
- L'intervention de la CGVMSL a consisté en une série de mesures ad hoc, ce qui a gêné la coordination et retardé le déploiement de l'équipement et du personnel d'intervention.
- Le manque de formation et d'expérience en ce qui concerne la lutte contre les incendies de navire des pompiers qui ont mené l'intervention, le manque d'équipement pour se rendre sur le navire, de même que l'inaccessibilité des plans de défense contre l'incendie, ont entravé la lutte contre l'incendie.
- Les ressources de lutte contre l'incendie qui existaient dans la région du canal Welland n'ont pas été utilisées efficacement pour circonscrire le feu et l'éteindre à temps pour prévenir la destruction des emménagements du navire.
3.2 Faits établis quant aux risques
- Le régime mis en place par la CGVMSL pour s'assurer que les employés, surtout ceux qui occupent des postes essentiels pour la sécurité, sont médicalement aptes à exercer leurs fonctions, laissait à désirer.
- Le pontier était le seul qui pouvait et devait s'assurer qu'il n'y avait plus de navire sous le pont avant d'abaisser la travée.
- Les pontiers travaillent très souvent seuls et la direction n'a pas beaucoup d'occasions de s'assurer qu'ils s'acquittent de leurs fonctions correctement et en toute sécurité.
- Les machines des ponts à travée levante du canal Welland sont si bruyantes que les pontiers peuvent difficilement entendre les communications VHF d'urgence lorsque la travée est en mouvement.
- Le système d'extincteurs automatiques à eau installé sur le Windoc est devenu inutilisable quand le réseau de distribution des extincteurs s'est effondré, les structures qui le supportait ayant été détruites par les flammes.
4.0 Mesures de sécurité
4.1 Mesures de sécurité prises
4.1.1 Avis de sécurité maritime concernant les capacités physiques et mentales des employés
En novembre 2001, le BST a envoyé l'Avis de sécurité maritime no 08-01 à la Corporation de gestion de la Voie maritime du Saint-Laurent (CGVMSL) concernant les lacunes liées au régime mis en place par la CGVMSL pour contrôler les capacités physiques et mentales de ses employés, et spécialement ceux qui occupent des postes essentiels pour la sécurité.
En réponse, la Corporation a pris les mesures suivantes :
- une politique provisoire sur les consignes relatives à la consommation d'alcool et de drogue, comprenant des tests de dépistage, a été préparée;
- afin de communiquer aux employés les attentes des gestionnaires et le processus d'adoption de mesures correctives, un programme de gestion des présences, un code de conduite ainsi qu'un code de discipline ont également été mis en place;
- la politique de la Corporation sur les congés de maladie a été modifiée en ce qui concerne la présentation des documents.
De plus, à l'heure actuelle, la Corporation :
- identifie les postes essentiels pour la sécurité;
- envisage la possibilité de requérir les services d'un médecin du travail.
4.1.2 Avis de sécurité maritime concernant la planification d'urgence
En janvier 2002, le BST a envoyé l'Avis de sécurité maritime no 02-02 à la CGVMSL concernant les préparatifs d'urgence de la Corporation pour faire face aux situations d'urgence dans la Voie maritime.
En réponse, la CGVMSL a mis sur pied un comité de planification d'urgence. Ce comité doit mener à bien les tâches suivantes d'ici décembre 2002 :
- élaboration d'une politique de planification d'urgence pour la CGVMSL;
- examen et mise à jour des plans d'urgence actuels;
- coordination des plans avec les organismes externes;
- identification et élaboration de programmes de formation;
- élaboration d'exercices de formation;
- promotion de la planification d'urgence.
Après avoir terminé les travaux ci-dessus, le comité de planification d'urgence s'attaquera à la mise à jour des plans et à la surveillance des exercices. Il devra aussi faire rapport chaque année de l'évolution de la situation au comité de gestion de la CGVMSL.
Le 29 mai 2002, une politique de planification des mesures d'urgence avait été mise au point . Un employé de la CGVMSL a depuis reçu de la formation sur la conception d'exercices.
4.1.3 Avis de sécurité maritime touchant la supervision des pontiers
En février 2002, le BST a envoyé l'Avis de sécurité maritime no 03-02 à la CGVMSL concernant l'adéquation de la supervision des pontiers pour s'assurer que ceux-ci sont en mesure de s'acquitter en tout temps de leurs fonctions de manière appropriée et en toute sécurité.
En réponse, la CGVMSL a restructuré ses opérations, les changements prenant effet avec l'ouverture de la saison de navigation de 2002. Quatre postes de chef de quart ont été créés pour superviser le personnel assigné aux opérations, y compris les pontiers, dans le canal Welland. Les chefs de quart doivent également visiter les pontiers de chaque pont, et ce, à chaque quart de travail. Ils sont sous la supervision des gestionnaires de secteur qui, à leur tour, rendent directement compte au vice-président de la région du Niagara.
De plus, un programme a été instauré pour assurer la surveillance des ponts à distance, depuis un centre des opérations, ce qui permettra une meilleure surveillance des pontiers.
La CGVMSL va aussi mettre en place des procédures structurées de prise en charge verbale par le pontier lors de la relève du quart.
4.1.4 Avis de sécurité maritime sur la lutte contre l'incendie
En mars 2002, le BST a envoyé l'Avis de sécurité maritime no 05-02 à la Sécurité maritime de Transports Canada (TC) pour l'avertir des risques constants posés par la préparation insuffisante des pompiers riverains à la lutte contre les incendies de navires. L'avis proposait en outre que la Sécurité maritime de TC, en collaboration avec les organismes fédéraux, provinciaux et municipaux, prenne d'autres mesures pour s'assurer que les pompiers des municipalités canadiennes limitrophes d'installations portuaires et de la Voie maritime sont formés et équipés pour intervenir lors de feux de navires.
TC a répondu qu'il avait pris les mesures suivantes depuis l'an 2000 :
- TC a rendu disponibles 77 raccords internationaux de jonction avec la terre pour utilisation par les services d'incendie de trois (Atlantique, Ontario et Pacifique) des cinq régions. Dans la Région du Québec, il existe 12 emplacements où ces raccords sont disponibles pour les pompiers.
- Quatre régions (Atlantique, Québec, Ontario et Pacifique) ont élaboré des mesures pour mettre en place des plans d'urgence dans certains ports et certaines installations portuaires. À l'heure actuelle, 49 plans d'urgence sont établis dans les ports et les installations de ports publics.
- Des ateliers de sensibilisation pour les pompiers susceptibles d'être appelés à lutter contre des incendies de navires dans un port public ont été dispensés dans quatre régions (Atlantique, Québec, Ontario et Pacifique). Ces ateliers avaient pour but de donner de l'information, pour fins de discussion, sur la façon d'intervenir en cas d'incendie à bord de navires. Au total, 37 ateliers ont eu lieu dans 31 communautés et ports, et 1 023 personnes y ont assisté.
En octobre 2002, lors d'une présentation dans le cadre d'une réunion des groupes opérationnels de l'Association des administrations portuaires canadiennes tenue à Prince Rupert (Colombie-Britannique), on a souligné le fait que de graves incendies de navire peuvent survenir, que les pompiers municipaux ne possèdent pas la formation requise et qu'une coordination préalable à un incident s'avère nécessaire.
4.1.5 Services d'incendie municipaux / Mesures de lutte contre l'incendie prises par la CGVMSL
À la suite de cet accident, les services d'incendie de quatre municipalités (y compris celui de Thorold) en bordure du canal Welland ont mis sur pied deux comités régionaux pour étudier les moyens de lutte contre l'incendie. L'un de ces comités est chargé d'examiner la question de l'équipement de lutte contre l'incendie à bord de navires. L'autre s'intéresse à la formation, notamment la formation touchant les lignes directrices de la United States National Fire Protection Association en ce qui concerne la lutte contre l'incendie à bord de navires ainsi que les procédures d'exploitation normales. Les deux comités ont tenu des réunions au cours des 12 derniers mois et ont rencontré la CGVMSL ainsi que certaines entreprises de navigation.
Le service d'incendie de Thorold a commencé à suivre un programme de visites de navires mis en rade dans le canal Welland pendant la saison hivernale afin de se familiariser avec les installations de navires. Des visites de certains navires qui empruntent la Voie maritime sont également prévues.
4.1.6 Changements apportés aux modalités de communication
En date du 1er mai 2002, la CGVMSL a instauré de nouvelles modalités de communication pour tous les ponts indépendants situés entre Montréal et Port Colborne. Dorénavant, immédiatement avant d'amorcer la séquence d'abaissement/fermeture du pont, le pontier devra effectuer un appel par radio VHF, sur la voie de travail normale, au dernier navire à passer sous le pont. En cas de problème, le fardeau de la réponse incombera au navire.
4.2 Mesures à prendre
4.2.1 Aptitude à l'exercice des fonctions et supervision des employés occupant des postes essentiels pour la sécurité
Le Bureau reconnaît que la CGVMSL a manifesté son intention de remédier aux lacunes relevées au cours de l'enquête. En réponse à l'Avis de sécurité maritime no 08-01, concernant les capacités physiques et mentales des employés, la CGVMSL a fait ressortir plusieurs mesures adoptées à ce sujet, comme l'identification des postes essentiels pour la sécurité, l'élaboration provisoire d'une nouvelle politique sur les tests de dépistage d'alcool et de drogue, ainsi que la mise à jour de la politique sur l'assiduité au travail et les congés de maladie. En réponse à l'Avis de sécurité maritime no 03-02, portant sur la supervision des pontiers, la CGVMSL a indiqué qu'elle avait augmenté le nombre de postes de supervision, et instauré de nouvelles modalités de prise en charge du quart et de nouvelles règles de communication entre les navires et les structures opérationnelles. Toutefois, le Bureau demeure préoccupé par la façon dont la CGVMSL envisage d'assurer l'aptitude physique et mentale des employés à exercer leurs fonctions, laquelle a été décrite en réaction à la communication des avis précités. Voici la position adoptée par la CGVMSL sur ce sujet :
- tous les postes d'exploitation (opérations et entretien) sont considérés comme essentiels pour la sécurité;
- les personnes sont jugées aptes à exercer leurs fonctions lorsqu'elles satisfont aux critères du processus de sélection, ainsi qu'aux exigences des examens médicaux préalables à l'emploi et des autres procédures approuvées par le syndicat;
- le verdict d'aptitude physique et mentale d'un employé à exercer ses fonctions est rendu par un médecin contractuel à la suite d'une évaluation clinique et c'est l'employé qui communique les résultats à l'employeur;
- le régime en place pour contrôler l'aptitude physique et mentale des employés est conforme aux dispositions de la Loi canadienne sur les droits de la personne concernant la protection des renseignements personnels.
L'action conjuguée de ces directives limite les possibilités ainsi que la responsabilité des pairs, des superviseurs et des gestionnaires d'identifier les employés dont l'aptitude à exercer leurs fonctions peut être compromise pour un motif quelconque et également de traiter avec ces employés. Bien qu'il soit probable que le régime en place pour contrôler les capacités physiques et mentales des employés ne contrevient pas à la Loi canadienne sur les droits de la personne, les dispositions de cette loi pourraient permettre un contrôle plus serré que celui qu'exerce actuellement la CGVMSL.
En juin 2002, la Commission canadienne des droits de la personne a publié une politique sur le dépistage des drogues et de l'alcool, fondée sur la détection et la prévention de tout genre d'altération des facultés en milieu de travail. En voici un extrait :
Hormis la consommation abusive d'alcool ou de drogues, il existe bien d'autres causes, notamment la fatigue, le stress, l'anxiété et les problèmes personnels, pouvant expliquer la situation de l'employé et étant susceptibles de constituer un risque pour la sécurité au travail. La Commission encourage les employeurs à adopter des programmes et des politiques où l'accent est mis sur les méthodes de repérage des entraves à la sûreté de fonctionnement des employés et dont la nature est curative plutôt que répressive. Ceux-ci peuvent prendre la forme d'un programme d'aide aux employés, de mesures de surveillance ou d'examen accrues et d'un encadrement par les pairs axés sur la réadaptation plutôt que sur la répression. Quant aux tests, leur rôle devrait se limiter à indiquer le degré réel d'altération de l'aptitude à s'acquitter de ses fonctions ou des obligations essentielles du poste.
En adoptant une telle philosophie, l'employeur dispose d'une certaine marge de manoeuvre, en particulier en ce qui concerne les postes jugés « essentiels pour la sécurité ». Pour les besoins de la politique, [Traduction] « un poste essentiel pour la sécurité est un poste pour lequel l'inaptitude causée par l'altération de ses facultés résultant de la consommation de drogue ou d'alcool peut entraîner directement un risque important de blessure à l'employé, à autrui ou à l'environnement. »
Par exemple, la jurisprudence a récemment permis de clarifier que la Loi canadienne sur les droits de la personne autorise la divulgation obligatoire d'une consommation abusive de drogue ou d'alcool, actuelle ou antérieure, lorsqu'il s'agit de postes essentiels pour la sécurité. Il est également concevable que la divulgation obligatoire de la prise de médicaments sur ordonnance soit considérée comme une exigence professionnelle normale au sens de l'article 15 de la loi, pourvu que l'on s'efforce de répondre de façon raisonnable aux besoins des personnes visées par cette mesure. La loi prévoit également qu'un test de dépistage de la consommation de drogue ou d'alcool effectué pour un motif valable ou faisant suite à un incident peut être .autorisé dans un environnement où la sécurité est primordiale et dans des circonstances particulières (c'est-à-dire lorsque le dépistage fait partie d'un programme plus large d'évaluation, de contrôle et de soutien médicaux).
Par conséquent, étant donné que la CGVMSL dispose d'un éventail restreint de moyens d'identifier les employés aux prises avec des problèmes personnels pouvant affecter leur capacité de s'acquitter de leurs fonctions, les gestionnaires de la CGVMSL devraient revoir leurs modalités de supervision et de contrôle à l'égard de l'aptitude physique et mentale des employés à remplir leurs fonctions afin de les resserrer dans toute la mesure autorisée par la loi. En conséquence, le Bureau recommande que :
La Corporation de gestion de la Voie maritime du Saint-Laurent réévalue et identifie clairement, au sein de son organisation, les postes essentiels pour la sécurité pour lesquels l'état d'incapacité associé aux facultés affaiblies pourrait entraîner un risque important de blessure à l'employé, à autrui ou à l'environnement.
Recommandation M02-01 du BST
et que
La Corporation de gestion de la Voie maritime du Saint-Laurent mette en place des programmes et des politiques fondés sur une approche proactive pour aider les gestionnaires, les superviseurs et les pairs à détecter rapidement l'état d'incapacité associé aux facultés affaiblies, dans le cas des employés occupant un poste essentiel pour la sécurité, et pour assurer qu'il y ait un mécanisme efficace permettant d'apporter des mesures correctives.
Recommandation M02-02 du BST
4.2.2 Planification d'urgence
Les décisions relatives aux mesures d'intervention doivent être prises avant que survienne la situation d'urgence et elles doivent être exposées dans un plan d'urgence destiné aux personnes appelées à intervenir en cas d'urgence. Toutefois, des exercices périodiques sur les modalités d'intervention sont essentiels pour évaluer l'état de préparation. Ces exercices permettent à ceux qui préparent le plan d'obtenir une rétroaction sur son efficacité (et sur le système d'intervention établi), et les enseignements qui s'en dégagent peuvent servir à améliorer à la fois le plan et la formation dispensée au personnel d'intervention. L'intervention type à bord d'un grand navire fait entrer en jeu divers organismes et agences, et l'action de chacun d'entre eux doit être coordonnée et intégrée à l'ensemble des opérations.
En réponse à cet accident, la CGVMSL a mis sur pied un comité de planification d'urgence qui sera notamment responsable de la coordination du plan d'urgence établi avec les organismes extérieurs, ainsi que de l'élaboration de programmes et d'exercices de formation. Ces dispositions devraient prendre place vers la fin de l'année en cours. La Corporation a élaboré une politique de planification d'urgence, dont l'un des principes directeurs est le renforcement de la coordination des activités avec celles des organismes d'intervention extérieurs.
Le travail actuel de la CGVMSL concernant la planification des interventions d'urgence à bord de navires est pris en compte par le Bureau. Toutefois, celui-ci est préoccupé par le fait que rien n'indique que la CGVMSL ait prévu de mener des exercices en cas d'urgence liée à un navire nécessitant l'intervention de plusieurs organismes. Ce genre d'exercice est nécessaire pour évaluer la planification d'une intervention d'urgence majeure. D'autres organismes ont organisé des exercices similaires sur le Saint-Laurent et les Grands Lacs, mais la participation de la CGVMSL était plutôt limitée. Le Bureau observe également que, depuis 1992, la Saint Lawrence Seaway Development Corporation, organisme gouvernemental américain responsable de l'exploitation de la Voie maritime à l'intérieur des frontières des États-Unis, participe chaque année à des exercices en cas d'urgence liée à des navires (ou en est l'hôte) nécessitant l'intervention d'organismes locaux, fédéraux, ou des États.
Pendant la saison de navigation 1999-2000, 3 141 navires ont emprunté le canal Welland, y compris des pétroliers et des chimiquiers. Les situations d'urgence liées à un navire et se produisant à proximité de secteurs densément peuplés le long de la Voie maritime, y compris le canal Welland, peuvent présenter un risque pour la sécurité de la population de ces secteurs. Par conséquent, ces situations d'urgence présentent une difficulté particulière pour les intervenants parce qu'elles nécessitent la coordination et l'intégration de l'action des divers organismes d'intervention. Aucun exercice en cas d'urgence majeure liée à des navires et faisant appel à d'autres organismes n'a été effectué sur le canal Welland. Étant donné que les risques associés à une mauvaise coordination sont plus grands que les risques associés à une coordination globale, le Bureau recommande que :
La Corporation de gestion de la Voie maritime du Saint-Laurent effectue, en collaboration avec les autorités et les organismes concernés, des exercices en cas d'urgence liée à un navire sur la Voie maritime, y compris sur le canal Welland, afin d'évaluer sa capacité à intervenir en cas d'urgence majeure liée à un navire.
Recommandation M02-03 du BST
À la suite de la commercialisation de la Voie maritime, dont la CGVMSL a la responsabilité de l'exploitation au Canada, TC a exercé peu de surveillance, voire aucune, pour assurer l'établissement de plans d'urgence, de formation et d'exercices permettant de répondre adéquatement aux urgences liées à des navires sur la Voie maritime. Bien que la CGVSLM soit responsable de l'exploitation de la Voie maritime, c'est TC qui conserve l'autorité réglementaire et c'est à ce Ministère qu'il incombe de s'assurer que les dispositions nécessaires sont en place en cas d'urgence liée à un navire sur la Voie maritime. En conséquence, le Bureau recommande que :
Le ministère des Transports s'assure que la planification générale est appropriée pour assurer une intervention efficace en cas d'urgence liée à un navire sur la Voie maritime.
Recommandation M02-04 du BST
4.2.3 Protection d'un pont contre un abaissement accidentel
Une étude réalisée par TC en 1982 intitulée Vulnérabilité des ponts dans les eaux canadiennes révèle que les ponts à travée levante ou les ponts tournants qui enjambent des cours d'eau étroits sont statistiquement plus susceptibles de heurter des navires. Cette étude révèle notamment que :
Quand on examine les caractéristiques d'un pont, il est nécessaire de s'attacher aux aspects de son fonctionnement ainsi qu'aux éléments physiques et à son mode de construction; il faut tenir compte de toutes ces données dans le contexte de l'environnement total du pont.
L'exploitation de tous les ponts à travée levante de la CGVMSL fait appel à une interaction étroite entre le pontier, le personnel du CCC, le pont et son appareillage; le pontier doit constamment être prudent et avoir une bonne idée de la situation. Toutefois, la présente enquête a révélé des lacunes liées au rendement du pontier et à la surveillance exercée par la direction à l'égard de l'exploitation du pont 11 la nuit de l'accident. Voici quelques-unes de ces lacunes :
- Le régime mis en place par la CGVMSL pour s'assurer que les employés, surtout ceux qui occupent des postes essentiels pour la sécurité, sont médicalement aptes à exercer leurs fonctions, laissait à désirer.
- La CGVMSL n'avait pas identifié les postes essentiels pour la sécurité ni défini de critères à cet égard, et le système de contrôle mis en place ne permettait pas de s'assurer que les personnes occupant ces postes étaient compétentes et aptes à remplir leurs fonctions.
- Les pontiers travaillent très souvent seuls et la direction n'a pas beaucoup d'occasions de s'assurer qu'ils s'acquittent de leurs fonctions correctement et en toute sécurité.
- Il est probable que le rendement du pontier était diminué au moment de l'accident.
Compte tenu des circonstances au pont 11 le soir de l'accident, un pontier travaillant seul ne constituait pas une protection suffisante contre l'abaissement par inadvertance de la travée levante du pont sur un navire. Des mécanismes de secours fiables sont donc essentiels pour prévenir ce genre d'accident.
Un consultant engagé par la CGVMSL pour examiner les éléments physiques permettant d'empêcher la fermeture prématurée du pont a indiqué que l'installation de ce genre de mécanisme n'est pas courante en Amérique du Nord. Le BST fait remarquer que, même si les ponts du canal Welland manoeuvrés à distance font l'objet d'une surveillance rigoureuse par caméra vidéo, la caméra du pont 11 n'offrait pas une vue suffisante pour permettre au personnel du CCC de contrôler l'environnement du pont. De plus, le BST a déterminé qu'un dispositif à infrarouge permettant de détecter la présence de navires à proximité des ponts est utilisé sur certains ponts régis par la Garde côtière américaine.
À la suite de cet accident, la CGVMSL a restructuré ses opérations et a créé des postes de supervision additionnels; elle a apporté des changements aux méthodes de travail de sorte que les chefs de quart doivent visiter chaque pont lors de chaque quart de travail, et elle a modifié les modalités de communication entre les pontiers et les navires. En outre, un programme à long terme d'automatisation des ponts a été mis en branle dans la région du canal Welland. Le Bureau se réjouit de ces faits; les mesures prises par la CGVMSL constituent une démarche positive pour remédier aux lacunes relevées dans le rapport en matière de procédures et de supervision. Le Bureau constate toutefois qu'en l'absence de systèmes de surveillance auxiliaires efficaces, la compétence du pontier demeure le seul moyen de protection pour prévenir l'abaissement par inadvertance de la travée sur un navire. En conséquence, le Bureau recommande que :
La Corporation de gestion de la Voie maritime du Saint-Laurent mette en place des moyens de protection physiques et administratifs pour s'assurer que les ponts de la Voie maritime ne puissent pas heurter les navires en transit.
Recommandation M02-05 du BST
4.3 Préoccupations liées à la sécurité
4.3.1 Accessibilité des plans de défense contre l'incendie
Sans plan en cas d'incendie, les pompiers, dont la connaissance des installations d'un navire peut s'avérer limitée au départ, ne peuvent pas savoir où se trouve le matériel de lutte contre l'incendie à bord du navire. Le Bureau souligne que TC est actuellement à réviser le Règlement sur le matériel de détection et d'extinction d'incendie. Toutefois, le Bureau est préoccupé par le fait que, d'ici à ce qu'on exige que les plans soient placés à l'extérieur du rouf sur les navires canadiens non visés par la Convention, l'inaccessibilité de ces plans sur les navires continue de faire obstacle à la capacité des services d'incendie municipaux de lutter contre ce genre d'incendie, ce qui accroît le risque de blessures au personnel et de dommages matériels.
4.3.2 Installation de systèmes d'extincteurs automatiques à eau
À la suite de l'accident, l'examen du système d'extincteurs automatiques à eau du Windoc a révélé que le réseau de distribution avait été fixé à des structures en bois. Une fois que le feu eut détruit les composants en bois des emménagements, le réseau de distribution des extincteurs s'est effondré et est devenu inutilisable. À la suite de deux incendies mortels mettant en cause des navires canadiens en 1979 et en 1981, on a installé sur beaucoup de vieux navires canadiens des systèmes d'extincteurs automatiques à eau dans les charpentes des emménagements. C'est pourquoi le Bureau s'inquiète du fait que ces vieux navires puissent être équipés de systèmes d'extincteurs automatiques à eau fixés à des structures internes combustibles, tout comme sur le Windoc, et que l'exposition de ces systèmes au feu risque de rendre ces systèmes inutilisables.
Annexes
Annexe A : Croquis du secteur de l'accident
Annexe B : Sigles et abréviations
- ACCP
- Association canadienne des chefs de pompiers
- IAPA
- Industrial Accident Prevention Association
- Ar.
- arrière
- Av.
- avant
- AVMSL
- Administration de la Voie maritime du Saint-Laurent
- BST
- Bureau de la sécurité des transports du Canada
- CCC
- centre de contrôle de la circulation
- CGVMSL
- Corporation de gestion de la Voie maritime du Saint-Laurent
- CID
- Centre d'intervention en cas de déversement
- CO2
- dioxyde de carbone
- dBA
- décibel pondéré en gamme A
- DSM IV
- Diagnostic and Statistical Manual of Mental Disorders
- GCC
- Garde côtière canadienne
- h
- heure
- HAE
- heure avancée de l'Est
- km
- kilomètre
- kW
- kilowatt
- m
- mètre
- M
- mille marin
- N
- nord
- NTSB
- National Transportation Safety Board
- OMI
- Organisation maritime internationale
- SCTM
- Services de communications et de trafic maritimes
- SI
- système international d'unités
- SSIE
- Direction du sauvetage, de la sécurité et de l'intervention environnementale
- TC
- Transports Canada
- UTC
- temps universel coordonné
- VHF
- très haute fréquence
- W
- ouest
- °
- degré
- ′
- minute
- ″
- seconde